




Casos Clínicos en Gastroenterología y Hepatología
Más datosInfectious diarrhoea is one of the most common diseases in the world and it is considered one of the five most important causes of death in resource-limited settings.1 Infectious diarrhoea is commonly self-limited and the major causes are viruses although it is also caused by bacteria (Salmonella, Campylobacter, Shigella, Yersinia, enterotoxigenic E. Coli, etc.) and protozoa (Cryptosporidium, Giardia, Entamoeba, etc.).
Different treatments can be useful since supportive management to hospitalization.2
The use of empirical antibiotic therapy in acute diarrhoea (AD) is unclear. Recent studies demonstrate that the use of antibiotic has not statistical difference in terms of length of hospital stay3 and they can cause side effects as promotion of bacterial resistance, eradication of intestinal normal flora and fungal overgrowth.
Fluoroquinolones has been historically the main therapy when indicated, with Salmonella infection as leading target, despite the decline in the last 10 years. Empirical therapy depends on suspicion. Recent studies define Campylobacter spp. as the main infectious agent in United States and Europe causing AD being resistant to fluoroquinolones over the 90% of cases, reason why macrolides are becoming first-line treatment.2
A descriptive retrospective study was carried out including stool cultures with pathogen isolation collected between 2018 and 2019 in patients older than 14 years old from a tertiary hospital with a health area of more than 160,000 people. The variables analysed were age, sex, place of request for stool culture (hospitalization, Emergency Room, Fist Care and Specialty Care Medicine), origin of the patient (Urban or Rural area), isolated pathogens and sensitivity and antibiotic resistance.
Pathogens isolated were collected in the following groups: Aeromonas, Campylobacter spp, Salmonella spp, Yersinia spp and Other (Plesiomonas, Helicobacter Pullorum and Shigella). Antibiotic sensitivity and resistance were tested against fluoroquinolones (Ciprofloxacin) and macrolides (Erythromycin).
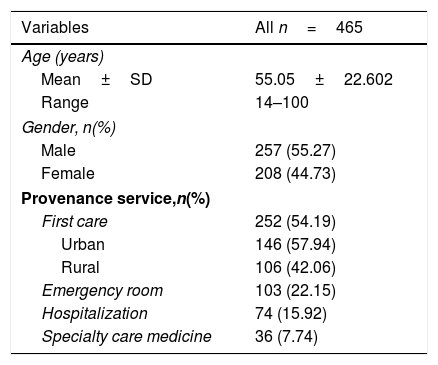
A total of 465 stool culture were analysed between January 2018 and December 2019. The epidemiological characteristics of the patients are shown in Table 1. 257 stools became from men (55.3%) and there were not statistically significant differences between male and female. The average age was 55.05 years old (SD±22.60). First Care was the main place of request for stool cultures (54.19%) followed by the Emergency Room (22.15%) and hospitalized patients (15.92%). 54% of First Care stool cultures became from urban areas, without statistical significance differences.
Demographic characteristics of the patients.
| Variables | All n=465 |
|---|---|
| Age (years) | |
| Mean±SD | 55.05±22.602 |
| Range | 14–100 |
| Gender, n(%) | |
| Male | 257 (55.27) |
| Female | 208 (44.73) |
| Provenance service,n(%) | |
| First care | 252 (54.19) |
| Urban | 146 (57.94) |
| Rural | 106 (42.06) |
| Emergency room | 103 (22.15) |
| Hospitalization | 74 (15.92) |
| Specialty care medicine | 36 (7.74) |
Campylobacter spp. was isolated in 251 stools (53.99%) followed by Salmonella spp. (20.22%) and Aeromonas spp. (17.63%) without statistical significance differences between 2018 and 2019. Sensitivity analysis showed that 98.4% of Campylobacter spp. were sensitive to Azithromycin and 1.6% resistant, while 8.8% sensitive to Ciprofloxacin. 100% of Salmonella spp. analysed were sensitive to Ciprofloxacin.
Campylobacter spp. has replaced pathogens as Salmonella spp. and enterotoxigenic E. coli as the leading bacteria related to AD of infectious aetiology in developed countries nowadays. Empirical antibiotic therapy, limited to patients with comorbidity, advanced age, and severe disease, constitutes a therapeutic tool of great interest in these cases, being necessary to adjust to the most frequent pathogens.4
The findings of our study provide one more justification to impose macrolides as first-line empirical therapy being sensitive over the 95% of the cases of Campylobacter, limiting quinolones to patients with a high suspicion of salmonellosis since Campylobacter spp. has been resistant in more than 90% of the analysed cases. Unfortunately, macrolide-resistant Campylobacter strains are progressively increasing, but macrolide resistance in Europe is still below 5%.2
Although Aeromona spp. has been found in a non-negligible number of stool cultures analysed, the role of Aeromona spp. in gastrointestinal disease has been debated. Even recent studies support pathogenic properties, there are not enough evidence to conclude the role in infectious diarrhoea and the need of specific treatment when detected in stool culture.5
Constant analysis of etiological agents in infectious pathologies is indispensable. Over time and, on each geographical area, infectious agents change as well as their sensitivity and resistance to antibiotic treatments, that makes essential a periodic study.
Conflict of interestNone.

