




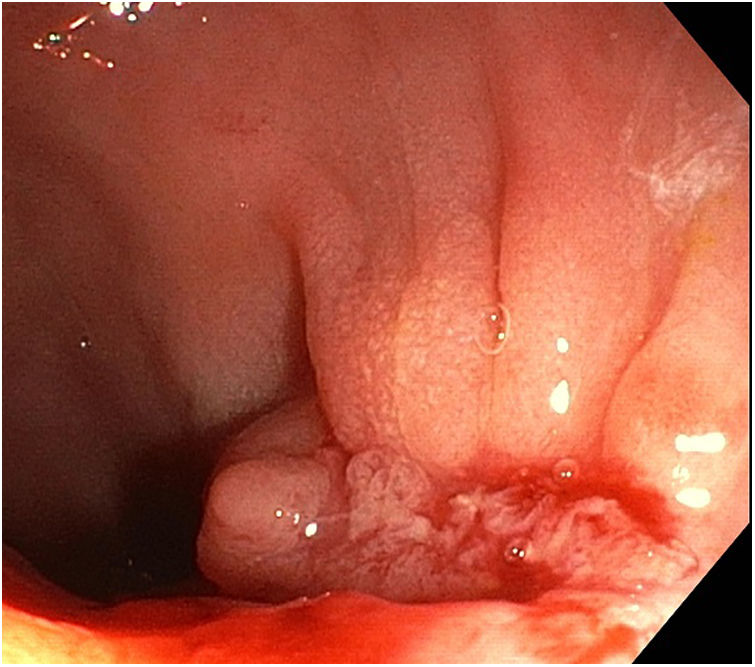
A 57-years old woman visited our institution for evaluation of diarrhea. Her familiar history included colorectal cancer (CRC) in her 75-year-old father. Among her medical records, three years before the patient complained about episodes of diarrhea with blood, and a colonoscopy was performed identifying multiple diverticula in the sigmoid colon. Other causes for diarrhea were excluded, and this episode resolved spontaneously. In this occasion, she presented with diarrhea and rectal bleeding of seven days of duration. Along with the blood, she had passed an ovoid specimen of tissue, which he brought to the hospital for investigation. Pathologic examination of the ovoid specimen showed it to be a polypoid carcinoma, 2.4cm×2.2cm. Physical examination was normal. Routine laboratory test and enhanced CT scan of the thorax, abdomen and pelvis disclosed no abnormality. At the second colonoscopy multiple diverticula were identified in the sigmoid colon. In the rectum (12cm from external anal margin) a flat elevated with central depression lesion (0IIa+0IIc) was identified (Fig. 1). The anatomopathological analysis showed a intramucosal adenocarcinoma. MRI showed a thickening of the upper rectal wall, of 17mm, above the peritoneal reflection, and there was no evidence of extramural extension or suspicious lymph nodes. A CT scan was performed ruling out metastasis.

A low anterior resection with partial mesorectal excision was performed, and a laparoscopic colorectal latero-terminal mechanical anastomosis. In the surgical piece a 2cm well-differentiated rectum adenocarcinoma that was invasive to the muscularis propria was found. No evidence of disease was found in the 15 lymph nodes retrieved. An immunohistochemistry analysis of MLH1, MSH2, MSH6 and PMS2 expression was performed confirming normal expression. The postoperative evolution of the patient was satisfactory.
The rate of a CRC after a colonoscopy is estimated of 3–4%.1 The possible explanations for these intervals CRC are missed lesions or the result of a prior incompletely resected polyp,1 or sometimes because of fast growth are considered as new CRC. In our case, a complete colonoscopy was performed 3 years before, no polypoid lesions were identified but only multiple diverticula in the sigmoid colon. It has been speculated that the presence of diverticulosis could impede the endoscopist's ability to visualize intervening mucosa, as well as making the exploration technically more difficult.2
In adults, spontaneous amputation of malignant colonic polyp is rare. To our knowledge, only 4 cases of autoamputation of colonic polyps have been reported.3–5 The first two documented cases in adults were described by Paul et al.3 in 1974; and one of these two cases is the only reported case of a colonic polypoid carcinoma being autoamputated. The case we report would constitute the second confirmed case of autoamputation of a polypoid carcinoma, but located in the rectum.
Autoamputation can be accompanied by abdominal pain and bleeding3 or be asymptomatic. Asyntomatic cases can present with disappearance of an elevated lesion, which is the ulcerated stump of the pedicle remaining after autoamputation of a polyp.4 Autoamputation presumably occurs because peristalsis induces traction on the stalk with ischemia followed by necrosis and sloughing of the polyp.4
Our patient's polypoid carcinoma was found in the rectum and was sessile. We hypothesized that in our case, traction may result in twisting of the polyp, causing a colonic pseudo-obstruction with increased bowel peristalsis, pain and diarrhea; and polyp necrosis and amputation with consequent rectal bleeding. The present case with documented endoscopic image after the autoamputation is the fifth reported case of an autoamputated polyp in the colon; and the second case of a confirmed polypoid carcinoma.
Conflict of interestsThe authors declare no conflicts of interest.

