




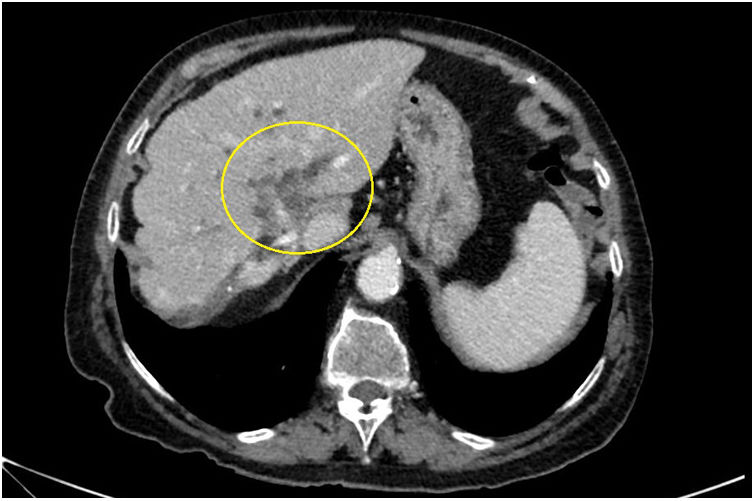
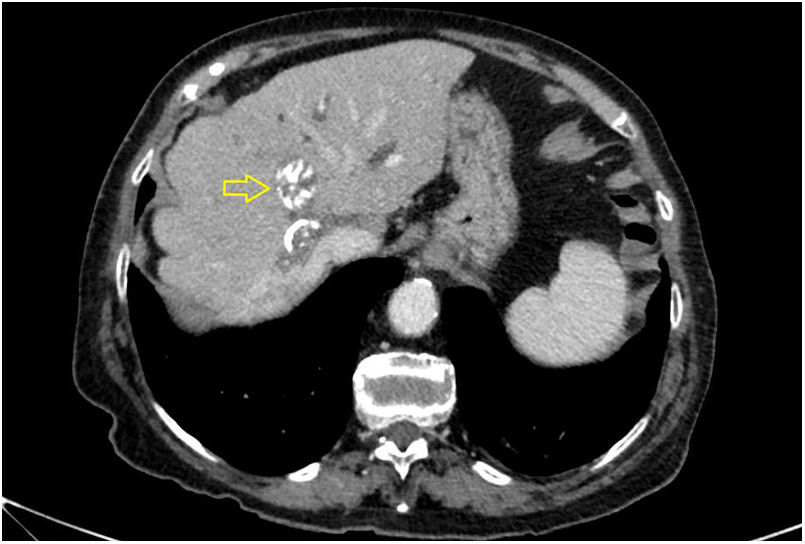
An 87-year-old woman was admitted for painless obstructive jaundice (bilirubin 5.8 mg/l) with dilation of the intrahepatic bile duct and a suspected Klatskin tumour on a computed tomography (CT) scan (Fig. 1). An adjacent calcified cystic lesion was also reported (Fig. 2).
.")
.")
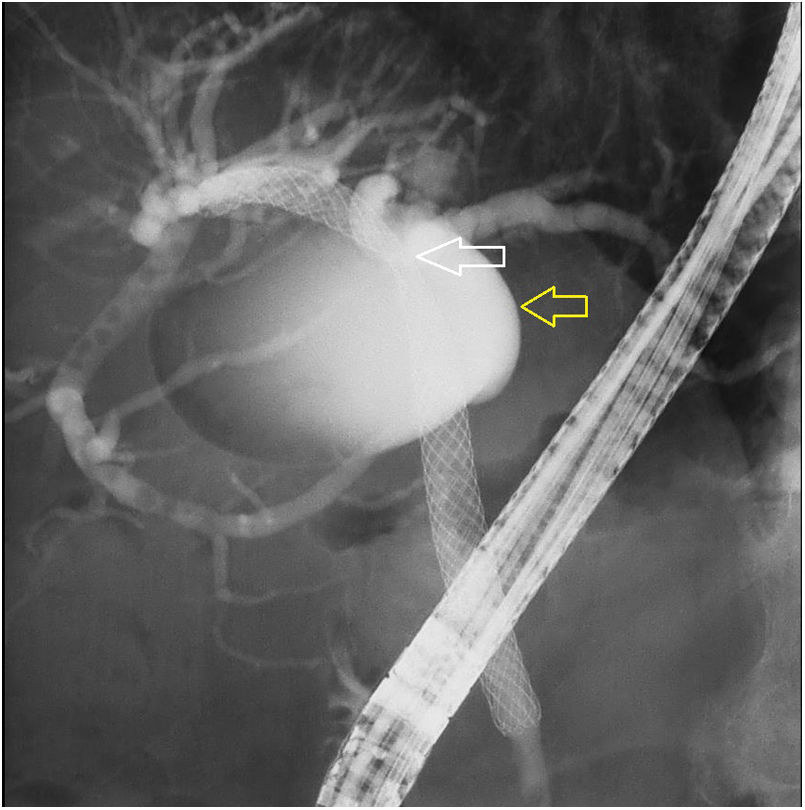
Endoscopic retrograde cholangiopancreatography showed a filled cyst in the hilum of the liver fistulised to the bile duct and causing secondary bile duct stenosis and compression (Fig. 3). Given the patient’s age and risk of the cyst re-filling, a decision was made to place an 8-cm uncoated metal biliary stent and confirm contrast emptying. Subsequent clinical and laboratory resolution.
 fistulised to the biliary tract, causing stenosis (white arrow), for which reason an uncoated metal biliary stent with a length of 8 cm and a calibre of 1 cm was placed and drainage was confirmed.")
Endoscopic retrograde cholangiopancreatography image showing a cystic lesion which filled with contrast (yellow area) fistulised to the biliary tract, causing stenosis (white arrow), for which reason an uncoated metal biliary stent with a length of 8 cm and a calibre of 1 cm was placed and drainage was confirmed.
Hydatid disease is a zoonotic infectious disease caused by Echinococcus granulosus (with a prevalence of 5%–10% in the Mediterranean region) associated with dogs and livestock1–3 and primarily affecting the liver (45%–75%).1
Although most patients remain asymptomatic, serious complications such as fistulisation have been reported.2
Fistulas (2%–75%) may be due to a connection between the cyst and the duct releasing hydatids into the biliary tract or to a hidden connection between bile duct branches (these usually remain asymptomatic).4
Various factors in fistulisation have been reported such as size (>8.8 cm), cyst type (Gharbi type 3 or 45) and location in the hilum.2,3
Advances in endoscopy enable non-invasive management; placement of a biliary stent, with or without balloon dilation, is the management option of choice.3
Please cite this article as: Saldaña C, Bolado F, González de la Higuera B, Borobio E, Casi MA. Estenosis biliar secundaria a quiste hidatídico fistulizado que simula tumor de Klatskin. Gastroenterol Hepatol. 2020;43:455–456.
