




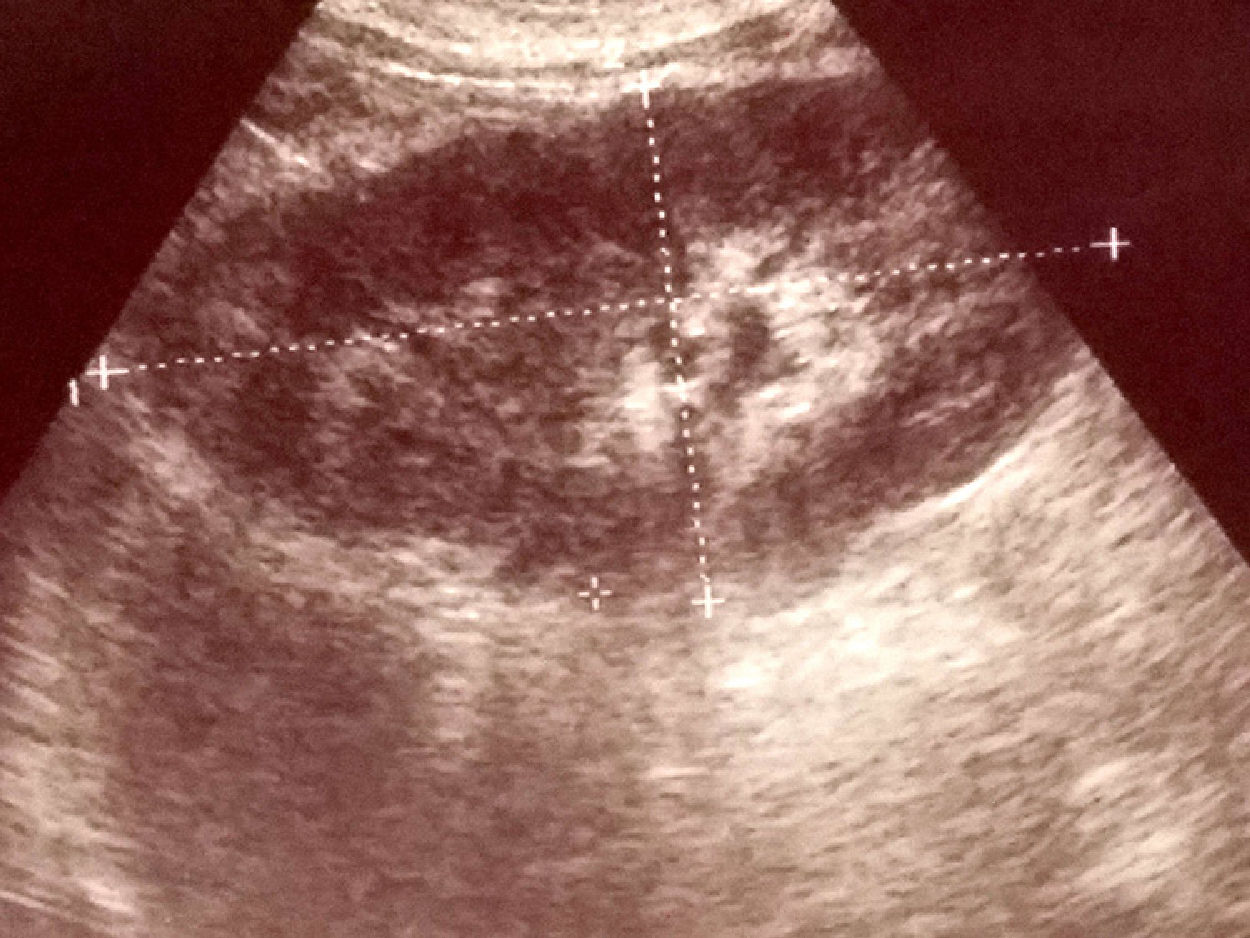
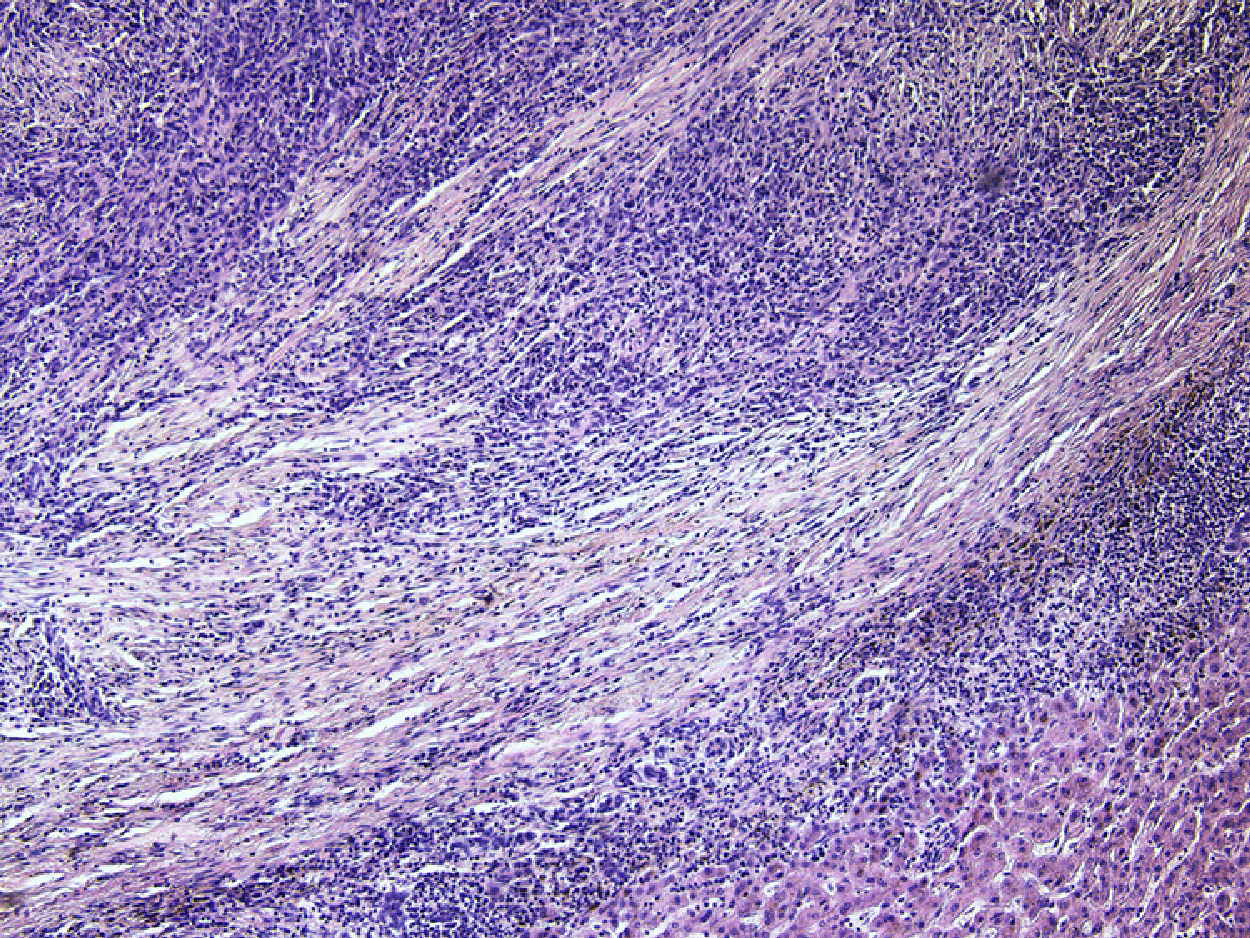
Hepatic inflammatory pseudotumor (HIP) is a liver manifestation of a systemic disease that can occur in organs like lungs, salivary glands and pancreas. Etiology and pathogenesis of the disease is not clear with autoimmune etiology being the most common theory.1 Recently, an attempt to explain the pathophysiology of the lesion in correlation with IgG4 has been undertaken. Pathological processes of inflammation can lead to specific set of changes in the tissue structure: lymphoplasmacytic inflammatory cells with fibrosis.2 Herein, we report a case of HIP diagnosed by laparoscopic resection (Figs. 1–2).
Case report

A 60-year-old man with a 5-years history of alcohol-related chronic pancreatitis with suspected liver tumors seen on routine CT has been referred for diagnosis. CT scans showed two poorly visible hypoechoic infiltrations; one in the segment II with a diameter of 28mm and the one in segment VI with a diameter of 20mm. On ultrasound only the tumor in segment II with a diameter of 14mm has been noted. The segment VI was free of any pathology on intraoperative ultrasound. Percutaneous liver fine needle biopsy has been performed with cytology showing chronic inflammatory cells. Laboratory data showed increased serum concentrations of bilirubin and white blood cells. The patient has been referred for a laparoscopic biopsy. The surgical resection of the segment II of the liver was performed by laparoscopy. On the 5th postoperative day the patient presented with abdominal pain, distention and signs of peritonitis. On emergency laparotomy bile peritonitis has been diagnosed. The leaking stump of a bile duct has been sewn and abundant peritoneal lavage performed. Further postoperative course was uneventful. Histopathological examination of the liver tumor showed diffuse inflammatory infiltration with lymphoid cells coinciding with the diagnosis of IgG4 related HIP. The blood test examination showed serum IgG4 level of 19.1g/l.
DiscussionThe differential diagnosis of a HIP is difficult.3 On imaging studies a HIP can mimic a metastatic disease, primary liver cancer or a benign lesion.4 Patients with HIP tend to be over 60 years old and more often (8×) men than women. There were several cases of exposure to industrial solvents, dust, lubricants and pesticides.1 In the differential diagnosis one has to consider especially Inflammatory pseudotumor which can occur in various locations (frequently in the lung). It can mimic malignant tumor. The lesion is composed of proliferation of fibrous tissue with presence of numerous inflammatory cells (plasma cells, lymphocytes, neutrophils, macrophages, multinucleated giant cells and eosinophils). HIP can be a IgG4-related disease. In our case there were two histological features of IgG4 – dense lymphoplasmacytic infiltrate and extensive fibrosis. On immunohistochemistry IgG stain showed many IgG-positive plasma cells and a number of IgG4-positive cells (focally >10cells/HPF; but altogether IgG4/IgG (+) cell ratio was about 10–20%). Other tumors to be considered in differential diagnosis of HIP are tumors of parasitic origin (for example Entamoeba), neoplasms (inflammatory myofibroblastic tumor) and other causes of inflammatory infiltration in the liver.
In the majority of patients the diagnosis can be achieved by needle liver biopsy, however, as in our patient, resection is sometimes required to reach the diagnosis.5
Unfortunately, the risk of serious and even life threatening complications after this procedure is much higher than after non-surgical diagnostic procedures.6 The full histopathological evaluation of the lesion, together with laboratory finding can give way to a firm diagnosis of a specific type of HIP.7 Once the diagnosis is established treatment with steroids is suggested.3 In patients who were diagnosed by biopsy alone, liver resection can also be required as a definitive treatment when steroid therapy is futile.5
Conflict of interestsThe authors declare no conflict of interests.
This work has been presented during 6th Biennial Congress of the Asian-Pacific Hepato-Pancreato-Biliary Association in Yokohama, Japan, 7–10 June 2017.
