




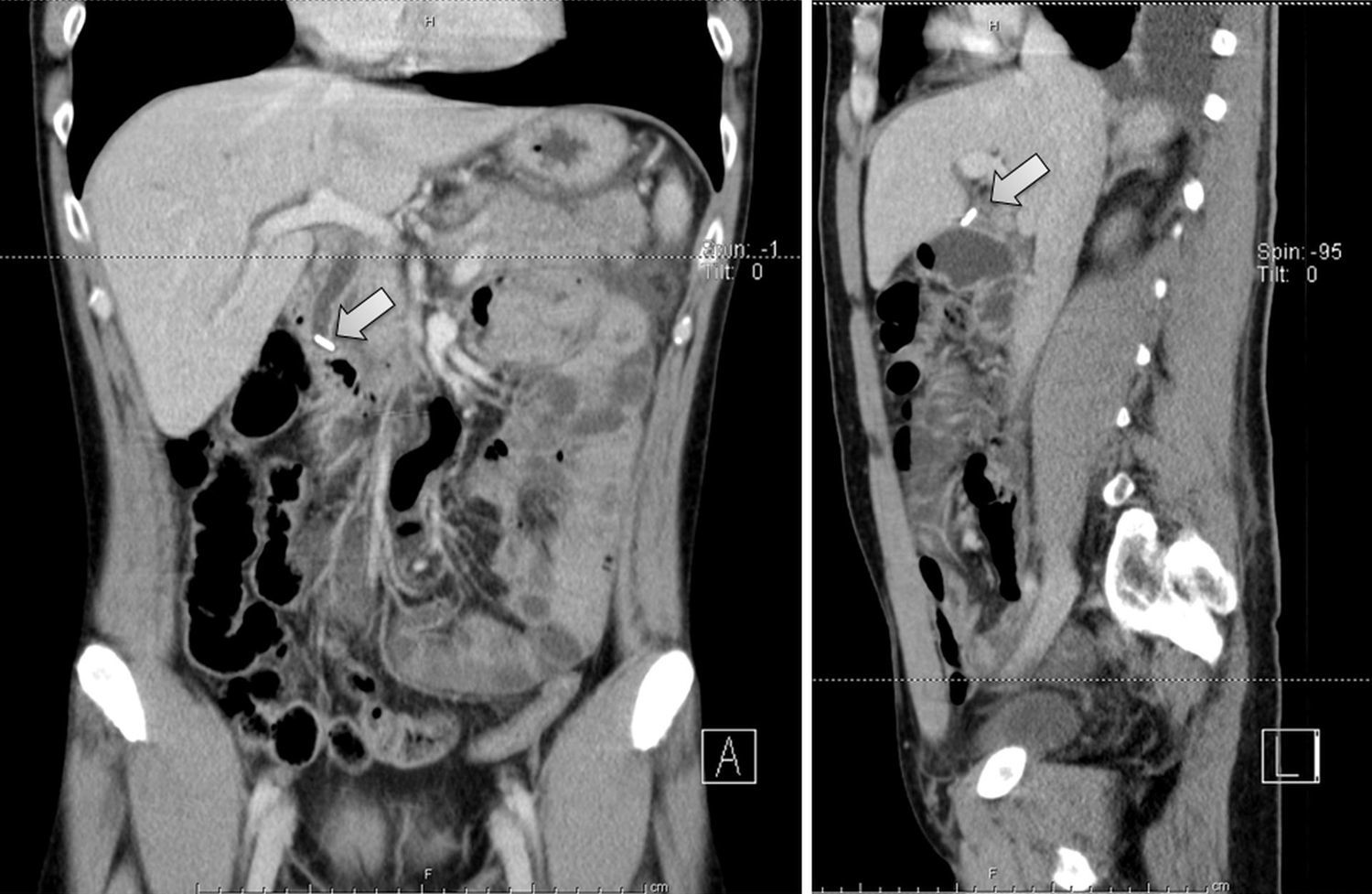
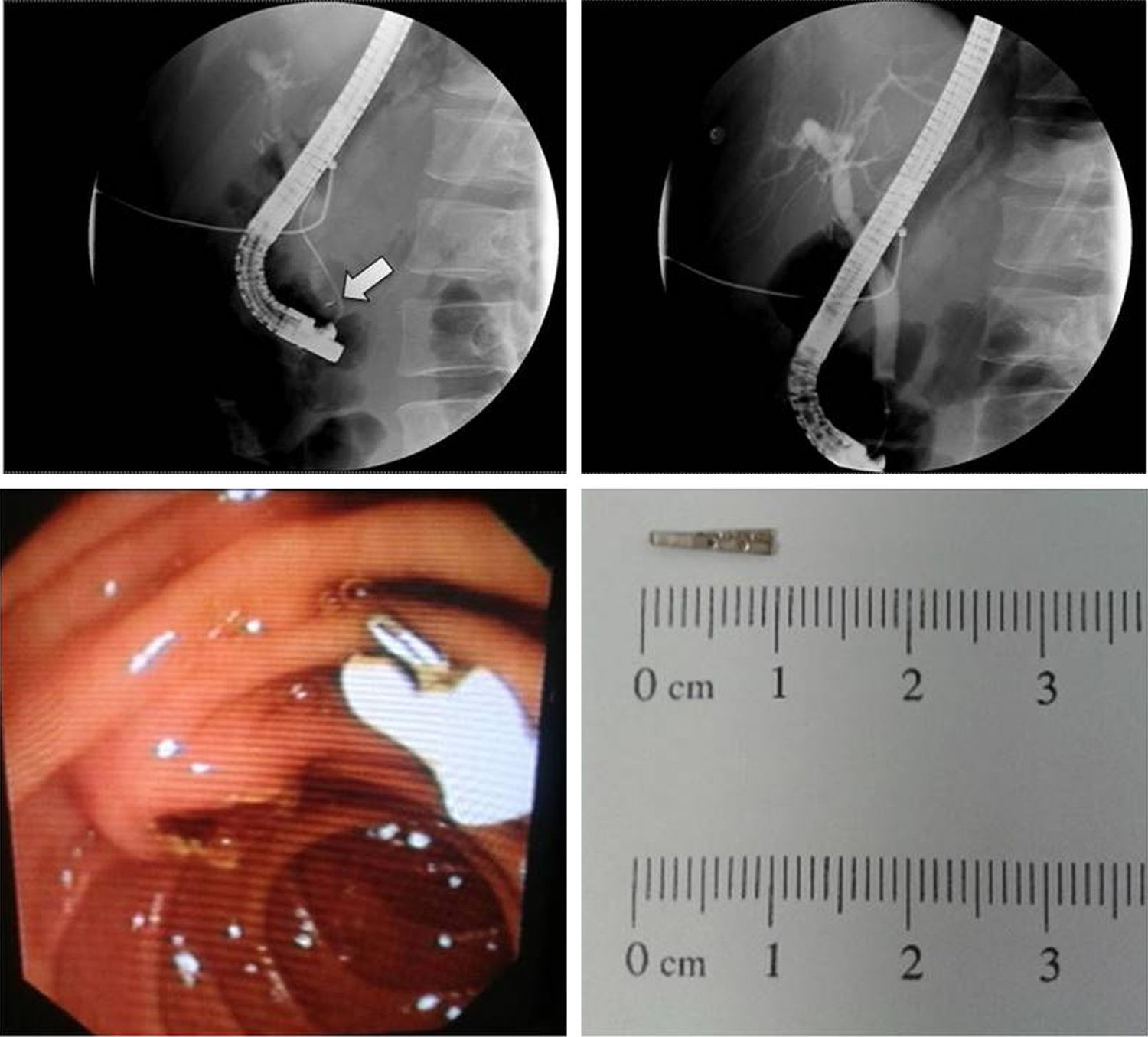
A 58-year-old male was admitted at our hospital for severe epigastric pain, nausea and vomiting. On physical examination patient was sweaty, restless and with marked tenderness in the epigastrum. Five years earlier he had gone through an uneventful laparoscopic cholecystectomy (LC) for cholelithiasis. Initial laboratory blood test were as follows: WBC: 11.6×109/L; ALT: 1124IU/L; AST: 1042IU/L; ALP: 149IU/L; TB: 3.6mg/dL; Amylase: 3793U/L; and CRP: 3mg/L. The initial imaging exams did not show abnormalities (chest and abdominal X-ray; abdominal ultrasound). There was a clinical deterioration in the first 48h with the development of fever, hemodynamic instability, increasing inflamatory parameters (WBC: 15.6×109/L; CRP: 96mg/L) and augmented TB (7.5mg/dL). Given the suspicion of a concomitant acute cholangitis, patient started antibiotics and an abdomen computed tomography (CT) scan (Fig. 1) was performed, revealing discreet extrahepatic ductal dilatation secondary to ocluding hyperdense material in the lower common bile duct and features compatible with acute pancreatitis. The radiological characteristics of the foreign body were consistent with a metal endoclip used in the previous LC. The patient underwent and emergent endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy and immediate removal of the migrated clip (Fig. 2). The posterior bile duct exploration was negative for lithiasis. This resulted in a hasty clinical and laboratorial improvement. Metal endoclips migrations after LC are a rare and unpredictable event with an unclear pathophysiological mechanism. In literature there are reports of endoclip migration into the common bile duct leading to stone formation, obstruction, cholangitis, stenosis and pancreatitis.1 In the absence of guidelines, from literature reports and our own experience, we consider that an ERCP should be deliberated as the first approach, since almost all cases are solved with sphincterotomy and surgery should be reserved to the unsuccessful procedures.1–5 Nevertheless, a previous multidisciplinary discussion with surgeons should be performed when managing this type of pathology.
Compartir



