





Management of traumatic pancreatic pseudocyst associated with pancreatic duct laceration is controversial. Surgical therapy has been clasically considered the treatment of choice for those pseudocysts. However, several authors have published good results with percutaneous drainage. Percutaneous drainage can be performed easily, with minimal complication and may facilitate the resolution of a pseudocyst.
We present a case of a 16-year-old boy who sustained blunt abdominal trauma in a vehicle accident. A large pancreatic pseudocyst developed, with complete disruption of the main pancreatic duct. Percutaneous drainage under ultrasound guidance was performed and was associated with the administration of octreotide (to inhibit exocrine pancreatic secretion). The drainage flow decreased gradually until ceasing, and the pseudocyst disappeared.
El manejo de pseudoquistes pancreáticos de origen traumático asociados con el desgarro del conducto pancreático es polémico. Tradicionalmente, el abordaje de elección para dichos pseudoquistes ha sido el tratamiento quirúrgico. No obstante, varios autores han publicado buenos resultados con el drenaje percutáneo. El drenaje percutáneo se puede realizar de forma sencilla, con mínimas complicaciones y podría ayuda a resolver el pseudoquiste. Presentamos el caso de un joven de 16 años que sufrió traumatismo abdominal contuso en un accidente de coche. Se desarrolló un pseudoquiste pancreático de grandes dimensiones que causó trastorno absoluto del conducto pancreático principal. Se realizó drenaje percutáneo bajo vigilancia ecográfica junto con la administración de octreótida para inhibir la secreción exocrina del páncreas. El flujo del drenaje descendió de forma gradual hasta su cese completo y la desaparición del pseudoquiste.
Pancreatic trauma is a relatively infrequent phenomenon, representing only 1–12% of all abdominal trauma.1–6 In the pediatric and adolescent age groups, abdominal trauma is usually a blunt injury, its most frequent complication being a pseudocyst.4 The treatment of pancreatic pseudocysts in childhood and adolescence differs from that of adults, and tends to be more conservative, using total parenteral nutrition or percutaneous drainage. This is probably due to the healthy state of children in general, including their pancreas.5 Traditionally, whenever major rupture of the pancreatic duct was involved, the treatment had been surgical. However, various authors have published good results using percutaneous drainage in these cases.6–8
We present a case of a 16-year-old male who sustained rhabdomyolysis and complete disruption of the pancreatic corporocaudal junction, which resolved satisfactorily without surgery, but rather with percutaneous drainage under ultrasound guidance, associated with the administration of octreotide.
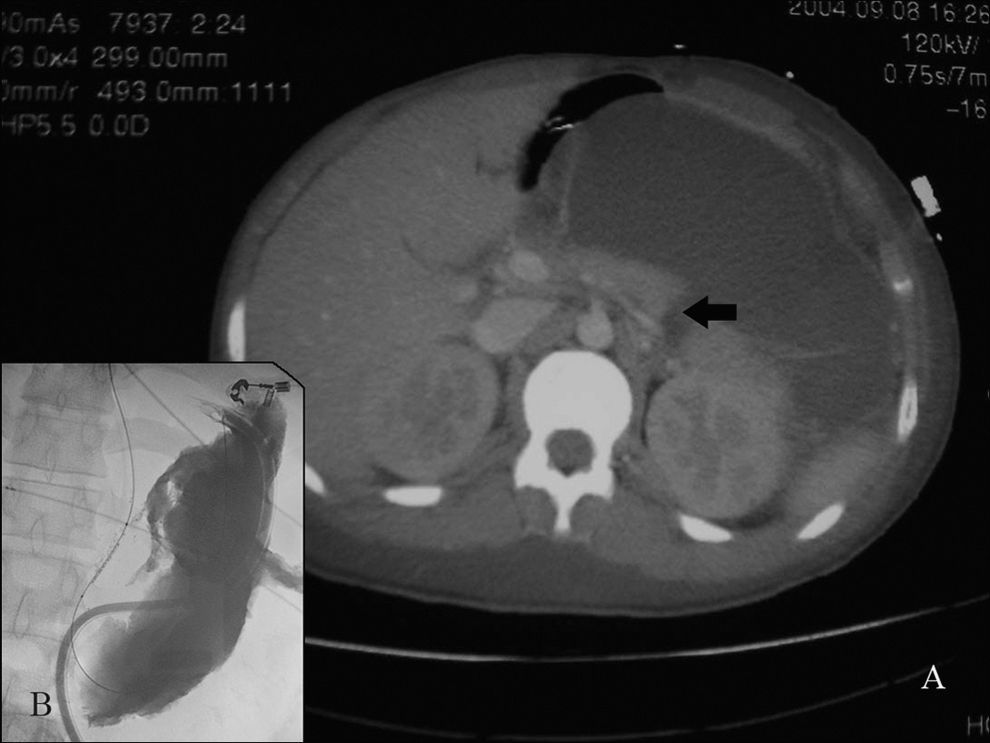
Clinical caseA 16-year-old male, of approximately 50kg in weight and 160cm in height, was admitted to the emergency service of our hospital after being trapped under a tractor for 4h. The patient was conscious, oriented and only referred anesthesia in the L2–L5 territory. The rest of the physical exam was normal and there were no other visible injuries. An abdominal-pelvic computerized tomography scan showed a fracture of the sacral foramen of S4 and a contusion of the left paravertebral and psoas musculature. No fractures of the spinal column were observed in reconstructive CT images. Blood lab work-up including amylase and lipase, were normal (46 and 38UI/L, respectively). The biochemistry results showed a CPK of 65000UI. During the first 24h of hospital admission in the Orthopedic Surgery service, the patient suffered progressive deterioration of renal function. He was diagnosed with rhabdomyolysis and was transferred to the Intensive Care Unit. At 48h post-trauma, the patient presented vomiting, abdominal distension and a palpable mass in the left hemi-abdomen. Another CT scan showed a collection measuring 10cm in diameter occupying the gastroesplenic space and a disruption of the continuity of the pancreatic tail, suggesting pancreatic rupture with pseudocyst formation (Fig. 1). Since we were dealing with a pancreatic rupture with a symptomatic pseudocyst in absence of active bleeding, and given our previous positive experience with the procedure, a percutaneous approach was decided on by the Radiology service. Percutaneous drainage through the stomach resulted in immediate drainage of 950cm3 of serohematic material. The amylase level in the extracted liquid was 12130UI/L. Treatment was begun with total parenteral nutrition and intravenous octreotide (0.1mg/day) with progressively increasing doses of up to 0.4mg/day. When the drainage stopped being productive 20 days after the catheter was placed, the catheter was clamped and removed. Over this period, the renal function normalized, the patient began to tolerate oral diet and was discharged after 28 days. The CT scan at one week follow-up showed a small pseudocyst of approximately 3cm in its largest diameter, which resolved in two months without treatment (Fig. 2). At four years follow-up, there is no evidence of recurrence.
 Abdominal CT scan suggests a transected pancreas in the corporocaudal junction (black arrow). Pseudocyst is also seen. (B) Pseudocystography of drained cavity, eight days later.")

Located in the retroperitoneum and relatively protected by the ribcage, vertebral column and the rest of the abdominal viscera, the pancreas is an infrequently injured gland, comprising only 1–12% of abdominal trauma injuries.1–6,9 In childhood and adolescence, the most common cause of pancreatic injury is blunt abdominal trauma resulting from different causes: bicycle handlebar injuries, traffic accidents, physical abuse, etc.2,4,7 According to some authors, a child suffering from blunt pancreatic trauma will develop a pancreatic pseudocyst up to 40% of the time,4,5 although this is probably an underestimate of the real incidence, since minor incidents may not be recorded.
Up to 50% of traumatic pancreatic pseudocysts resolve with medical treatment, complete bowel rest and total parenteral nutrition.4,5,9–11 However, if there is persistent abdominal pain, fever and increase in size as seen in an ultrasound scan, or when there is no spontaneous resolution, drainage is necessary in order to avoid complications; hemorrhage, perforation, infection, or intestinal or biliary tract obstruction4,5,10 can be seen in up to one-third of the cases.
Rupture of the main pancreatic duct is considered an indication for surgery, which uses one of the following techniques: internal drainage, external drainage or excision, depending on the location of the injury.7,11 While percutaneous drainage is reserved for those cases in which the pancreatic duct remained intact.9,11 In recent years, however, thanks to advances in imaging techniques, cases similar to ours have been published, where major pancreatic duct involvement did not condition surgical treatment. In studies by Shilyansky et al.,10 Ohno and Ohgami,8 Burnweit et al.,4 Jaffe et al.7 or Lucaya et al.,5 among others, surgery appears to be reserved for those cases where percutaneous drainage is not effective. Thus, ultrasound guided percutaneous drainage appears to be a safe and effective option. Nevertheless, there are so few published cases of this sort, that it is does not allow for establishing universal recommendations strictly based on scientific evidence. Therefore, percutaneous drainage should probably be considered as only a promising alternative and not a standard treatment for these patients.
The contrast-enhanced CT is probably the best test for diagnosing possible abdominal lesions in children who have suffered abdominal trauma. However, while CT images confirm parenchymal lesions in most cases, they do not allow for directly detecting a disruption of the main pancreatic duct. In our case, the first CT performed upon hospital admission did not show the ductal lesion, which was evidenced in the second CT after the abdominal symptoms appeared and when the pseudocyst was observed. Given the potential inaccuracy of the CT in detecting possible lesions of the main pancreatic duct, some authors propose early ERCP in all children with traumatic pancreatitis.13 Others, on the other hand, do not support their use or reserve it for patients with pseudocysts that have not resolved satisfactorily after various weeks of non-surgical treatment.6 In our opinion, the ERCP is definitely a good technique for determining if the lesion of the duct is complete or incomplete, or for the treatment in some cases by means of transpapilary stent placement.13 However, ERCP is not free of harm, and its potential complications must be considered (hemorrhage, infection, pancreatitis, perforation). Moreover, it usually requires general anesthesia in the pediatric population. Most importantly, the experience of the endoscopist must be taken into consideration. Therefore, we believe that it should be performed only when the results can be used to modify posterior treatment, and should always be done in institutions having sufficient experience with interventional endoscopy. In any case, if we decide on using a conservative approach with percutaneous drainage, knowing whether or not the duct is lesioned will not change our decision, in which case ERCP could be avoided in the majority of cases.5,6 In our opinion, ERCP would be reserved for those patients presenting persistence of external fistula and failure of the percutaneous drainage, in which case, a possible surgical intervention must be planned. Magnetic retrograde cholangio-pancreatography has recently been used to delineate the pancreatic duct and according to Degiannis et al.,12 it could replace ERCP as a first-line investigation in the future. However, this technique is not always available in all institutions.
The surgical approach for placing the drainage catheter varies according to the author's preference. Jaffe et al.7 recommends placing it between the left hepatic lobe and stomach or between the stomach and spleen, because the transgastric approach is more prone to catheter dislodgement due to respiratory and peristaltic movements. On the contrary, Burnweitt et al.4 prefer the transgastric method. In our case, we were obliged to use the transgastric approach due to the large size of the pseudocyst. The outcome was positive and there was no evidence of peritonitis, hemorrhage, fistula or catheter dislodgment. Therefore, we consider this approach a good option in similar situations. Drainage should be maintained until it ceases to be productive; this normally occurs between the third and fourth weeks. Before withdrawing the drainage catheter, we advise clamping the catheter and starting oral feedings to confirm the absence of drainage output. Follow-up with ultrasound and CT scans allows us to know the posterior state of the pseudocyst.
In our case, a small cyst of 3cm in diameter persisted after removing the drainage. This small cyst, as in other publications,7 resolved spontaneously and only required ultrasound scan follow-ups.
Percutaneous drainage does not shorten hospital stay duration compared to surgical treatment, since it is still necessary for the patient to be hospitalized for some time. However, we can avoid laparotomy-associated morbi-mortality by using the percutaneous technique.
Octreotide is not widely used and little is known about its utility in childhood and adolescent groups. No comparative studies have been done on percutaneous drainage with and without octreotride administration. Octreotide is an octopeptide analogue of somatostatin, sharing a similar mechanism but with a half-life of 90–113min, thereby allowing its administration by subcutaneous or intravenous routes. Octreotide, among its other known actions, has been shown to inhibit exocrine pancreatic secretion, as seen used in postoperative pancreatic fistulas, decreasing pseudocystic drainage output.14 The initial recommended dose is 0.1mg/day, though it can be increased if it continues to be productive in 2–3 days. In our case, the dose had to be increased up to 0.4mg/day. Complications from the use of octreotide have been described, such as pain at the injection site, gallstones or growth changes, none of which we experienced with our patient.
Conservative treatment is being used more and more frequently in abdominal trauma with different visceral injuries (liver, spleen, kidney) in children.4–6 For pancreatic trauma cases, however, these results, though well demonstrated, have not been generally applied to the surgical setting. According to our experience, the pancreatic pseudocyst with major rupture of the pancreatic duct could add itself to the list of injuries to be treated conservatively, since treatment with percutaneous drainage associated with octreotide use is safe and effective, as long as human and material means are available to carry out the procedure.

