


Malignant colorectal obstruction is a serious complication of advanced cancers. The obstruction can be caused by colorectal cancer, adjacent organ cancer or distant metastases. Rectal metastases from gastric cancer are rare. Foreign body ingestion is not a rare event and the majority of them causes no symptoms or complications. Nevertheless, they are likely to stop at any narrowing or angulation of the intestinal lumen. The authors describe a rare clinical presentation of an impacted foreign body in a pathological narrowing secondary to rectal metastasis of a gastric neoplasia that caused an acute malignant colonic obstruction. After endoscopic removal of the foreign body, there was complete resolution of symptoms avoiding surgery or palliative stenting. This case report highlights the need of careful inspection of colonic malignant strictures before stenting to exclude other causes of colonic obstructions, as an impacted foreign body.
A obstrução colorretal maligna é uma complicação de neoplasias em estadio avançado. A obstrução pode resultar de neoplasias colorretais, neoplasias de órgãos adjacentes ao cólon ou metastização. A metastização cólica de neoplasias gástricas é rara. A ingestão de corpos estranhos não constitui um evento raro e a maioria dos casos cursa sem sintomas ou complicações. Contudo, estes podem ficar retidos em áreas de estreitamento ou angulação do lúmen intestinal. Os autores descrevem uma rara forma de apresentação clínica de impactação de corpo estranho numa estenose retal maligna secundária a metástases de neoplasia gástrica, que condicionou obstrução cólica maligna. Após remoção endoscópica do corpo estranho, verificou-se resolução da sintomatologia sem necessidade de tratamento cirúrgico ou colocação de prótese. Este caso ilustra a importância da inspeção minuciosa das estenoses malignas previamente à colocação de prótese para exclusão de outras causas de obstrução cólica, como corpo estranho impactado.
Gastric signet ring cell carcinoma (SRC) is a mucin-secreting adenocarcinoma. Ninety-nine percent of SRC occurs in the stomach, mainly in body or lower stomach and it is more common in younger patients.1,2 Advanced SRC is more often associated with larger tumors, lower curative rates, more serosal invasion and greater peritoneal dissemination compared with other advanced gastric cancers.2
The most frequent metastatic locations of gastric cancer are to the liver, peritoneal surfaces, and distant lymph nodes. Colonic metastases from gastric cancer are rare.3
Our case report highlights a pathological narrowing of the intestinal lumen secondary to rectal metastasis of a gastric neoplasia that resulted in an impacted chicken bone causing an acute malignant colonic obstruction.
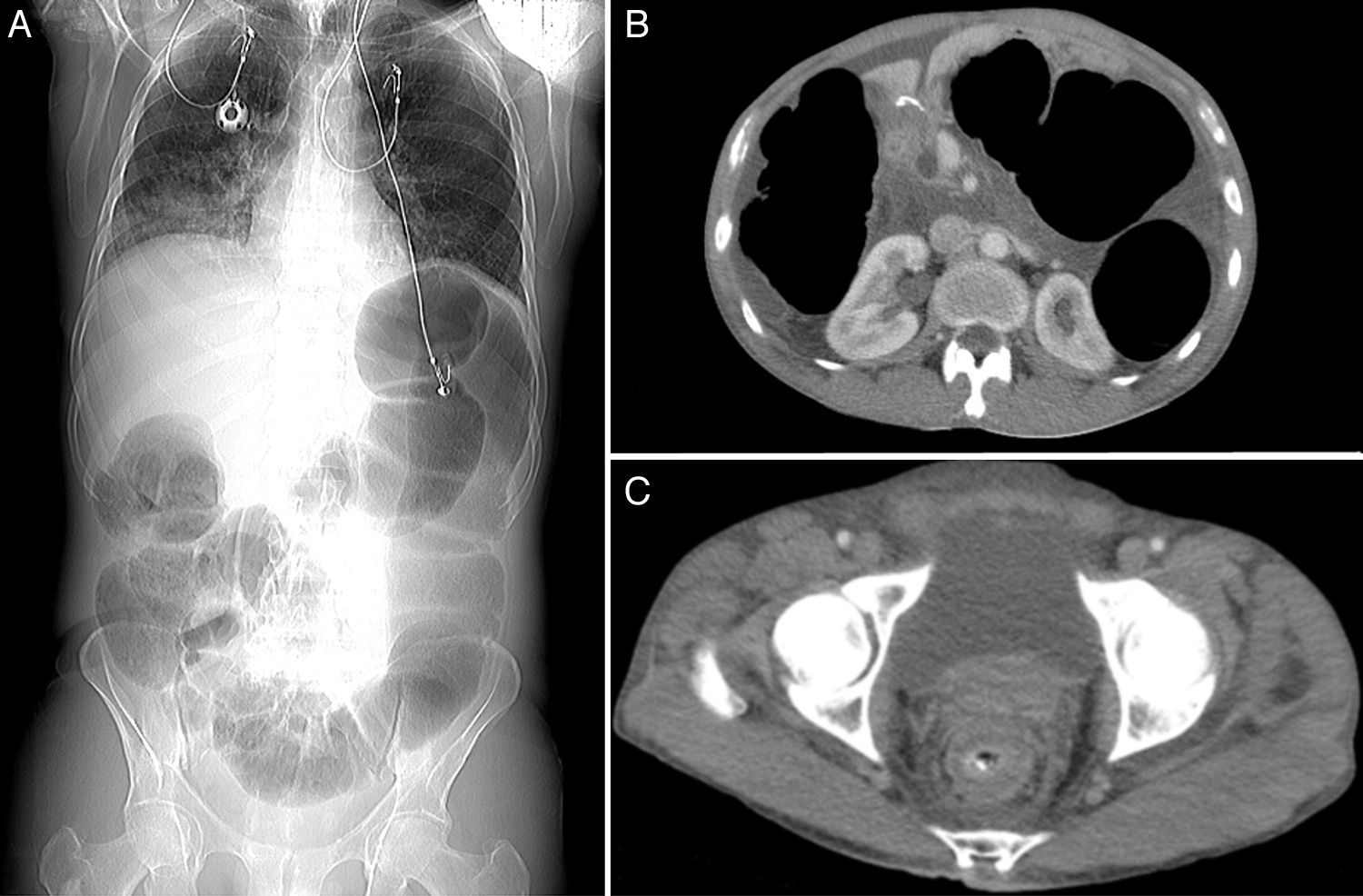
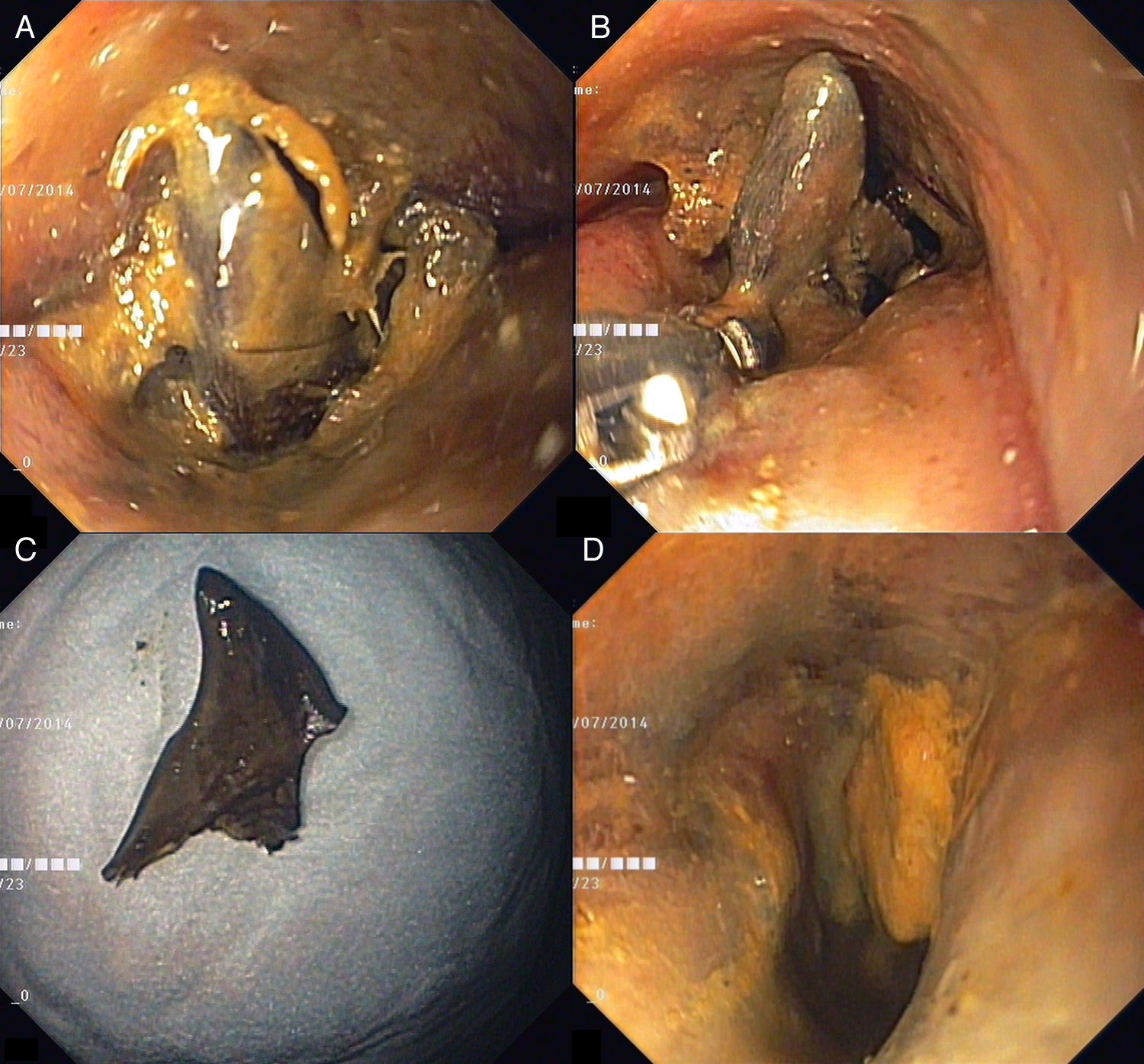
2Case reportA 51-year-old man presented with a 1-day history of intense abdominal pain, vomiting, constipation and inability to pass gas. His past medical condition comprised an advanced gastric SRC (T3N2M0), diagnosed when the patient was 47 years old. He was submitted to distal gastrectomy and adjuvant chemotherapy and three years later, palliative chemoradiotherapy for non-obstructive rectal and prostate metastasis. Physical examination revealed no signs of peritoneal irritation. Laboratory tests showed an acute kidney injury. An abdominal X-ray demonstrated marked colonic distension and computed tomography (CT) revealed a malignant rectal stenosis with proximal colonic dilation (Fig. 1A–C). Considering his medical condition, the patient was referred for palliative stenting and underwent a sigmoidoscopy. The sigmoidoscopy depicted a malignant stricture with an impacted chicken bone leading to edema and complete obstruction (Fig. 2A). After removal of the foreign body with a rat-tooth forceps (Fig. 2B and C), the colonoscope was easily passed beyond the stricture (Fig. 2D). Due to reestablishment of bowel movements, stenting was postponed. Upon CT review, a radiopaque object was found within the rectal stricture (Fig. 1C).
 proximally to a rectal stenosis with thickened wall and a radiopaque image in its lumen (C).")
, which was removed with a rat-tooth forceps (B). After extraction of the foreign body (C), the malignant stricture was easily traversed and was only causing a minor narrowing of the lumen (D).")
Endoscopic images showing a congestive rectal mucosa and a narrowed lumen with an impacted chicken bone occluding the luminal passage (A), which was removed with a rat-tooth forceps (B). After extraction of the foreign body (C), the malignant stricture was easily traversed and was only causing a minor narrowing of the lumen (D).
Malignant colorectal obstruction is a serious complication of advanced cancers, including colorectal cancer, adjacent organ cancer or distant metastases.4 In advanced digestive cancers, bowel obstruction is usually insidious and presents with non-specific gastrointestinal symptoms, such as vomiting, abdominal pain and distension.4,5 In opposition, our patient manifested an atypical presentation with an acute malignant colonic obstruction resulting in an abrupt clinical course. Self-expanding metallic stents represent a palliative treatment approach that can be offered to patients with incurable disease.4 Although foreign body ingestion is not a rare event and the majority of them causes no symptoms or complications, they are likely to stop at any narrowing or angulation of the intestinal lumen.6 Ingested foreign bodies can lead to complications such as abscess and fistula formation, perforation and bowel obstruction, or even to the incidental diagnosis of an occult neoplasia.6,7 To our knowledge, only a few similar cases of colonic malignant obstruction with an impacted foreign body have been recently described.8,9 In these case reports, the ingestion of the foreign body which was recalled by the patients, has led to the incidental diagnosis of an occult neoplasia, which was managed surgically.8,9 In contrast to the previous reports, our patient was not aware of the ingestion of the foreign body and had known rectal metastasis, explaining the initial referral for palliative stenting. After recognition of the impacted foreign body, the patient was managed endoscopically with resolution of symptoms.
This case report highlights the need of careful inspection of malignant strictures before stenting and the rare clinical presentation of an impacted foreign body whose ingestion was not recalled by the patient, causing an acute malignant colonic obstruction.
Conflicts of interestThe authors have no conflicts of interest to declare.
Grant supportGrant support was not provided for this article.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
