


A 57-year-old African woman was admitted to our clinic with a 1-week history of dysphagia and hematemesis. Her medical history was relevant for recently diagnosed human immunodeficiency virus (HIV). On admission she was hypotensive and tachycardic. On physical examination she had multiple purplish papules on the extremities and trunk. Laboratory tests revealed severe anemia (6.1g/dL), thrombocytopenia (32.0×109/L), very low CD4 cell count (3U/L) and high HIV viral load (12,000copies/mL). Upper endoscopy showed a violaceous plaque-like lesion at the gastroesophageal junction (Fig. 1A) and several patchy erythematous and hemorrhagic lesions in the stomach (Fig. 1B and C). As the skin lesions have already been biopsied and our patient had severe thrombocytopenia, we decided not to perform gastric biopsies. The histologic examination of the skin biopsies showed slit-like vascular spaces, extravasated erythrocytes and a specific sign – the promontory sign (small blood vessel and its stroma project like a promontory into a vascular space) (Fig. 2). These findings were suggestive of Kaposi's sarcoma (KS). The patient was started on antiretroviral therapy and liposomal doxorubicin, with clinical improvement, without evidence of new bleeding episodes and nearly complete resolution of the cutaneous lesions. KS is a vascular tumor caused by human herpesvirus 8 (HHV8) infection. There are 4 types of KS: classic – occurs specially in elderly men and it is associated with visceral disease just in 10% of cases, endemic/African – more common in children, iatrogenic – for example as a result of suppressed immunity in organ transplantation and acquired immune deficiency syndrome (AIDS) related KS. Kaposi syndrome is the most common neoplasm in AIDS patients (15–20%). Skin is the most affected organ (78%) and even though the visceral involvement is less frequent, occurs up to 25% of AIDS patients. The gastrointestinal tract is the most frequently involved extracutaneous site, followed by lungs, liver, spleen and kidney, with the stomach being affected in 55% of cases.1 Among these, 80% of cases have concomitant skin lesions.1 Nevertheless, in up to 81.5% of all cases the patients are asymptomatic.1,2 Nausea, vomiting, GI bleeding and gastric outlet obstruction are uncommon manifestations.1 AIDS-related KS is not curable and its treatment with HAART and liposomal doxorubicin pegylated (LD) is palliative. LD is the chemotherapeutic of choice because it accumulates preferentially in KS tissue, reducing the dose and drug toxicity.1 Previous studies have shown a better overall response to LD of gastric lesions compared with cutaneous lesions, with 73% of the patients obtained a complete response of the gastrointestinal KS lesions comparing with 13% of patients with cutaneous lesions.3 The incidence of relapse is 13%/year, occurring especially during the first year after completing LD. 33% of these patients would not respond to LD and paclitaxel is actually the second line agent.2 Therefore, screening endoscopy in selected asymptomatic patients has been suggested by some authors.2 A recent study found that CD4<100cell/μl, men who have sex with men and the presence of cutaneous KS are significant predictors of GI-KS.2
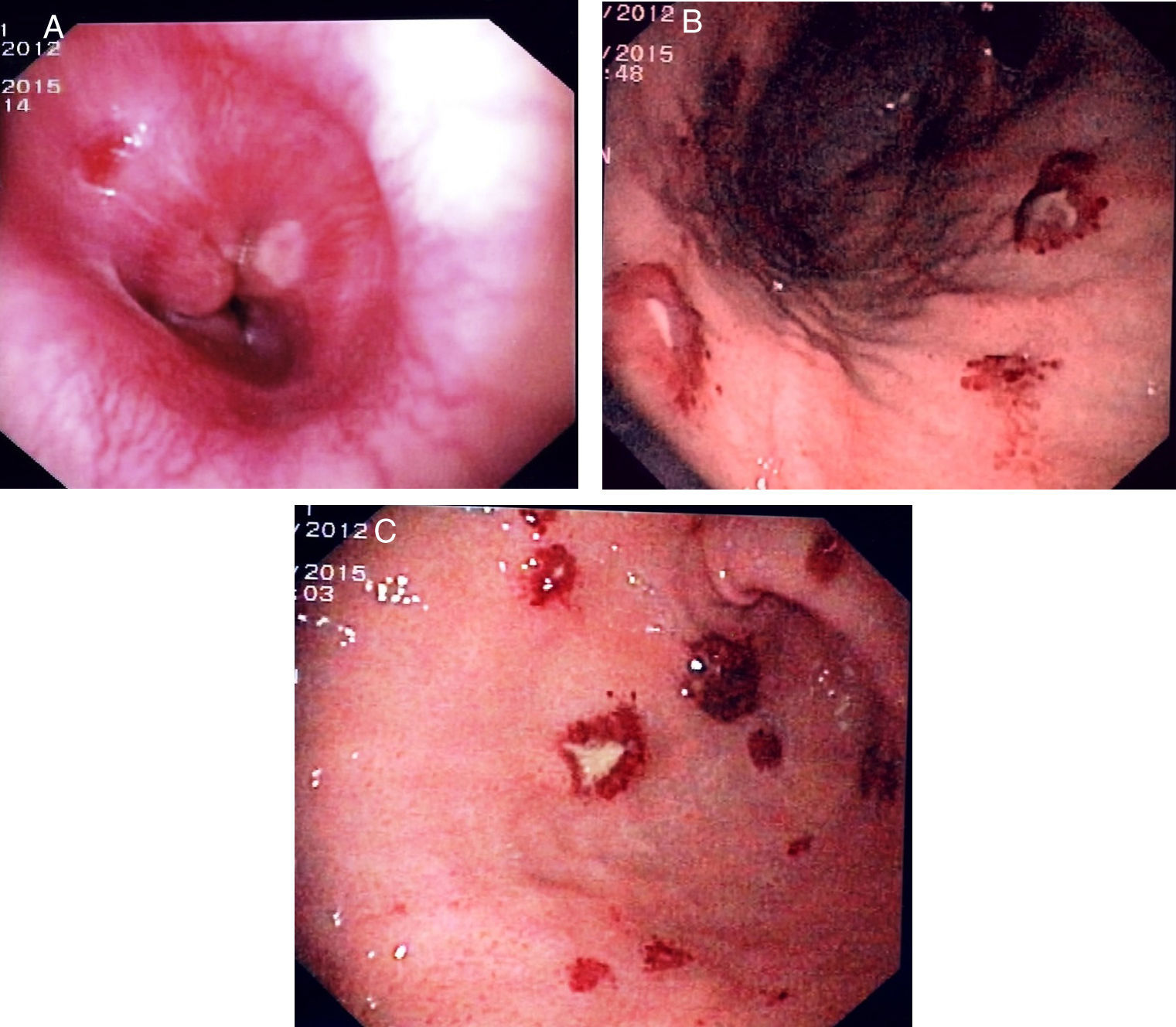
 Upper endoscopy showing in the esophagus–gastric transition a violacea and papular lesion. (B and C) Upper endoscopy showing fundus, body and antrum of the stomach with multiples patchy, raised, erythematous and hemorrhagic lesions with 8mm of diameter.")
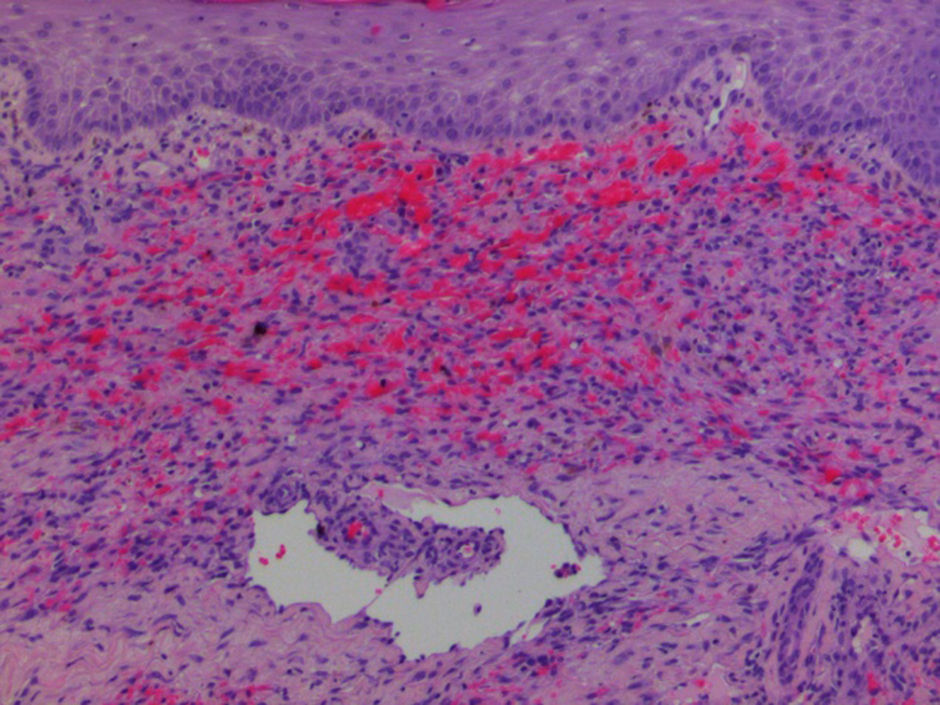
 (H&E ×200).")
The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
