


Substantial variation exists between schools and countries as regards the role of ethics, law and professionalism in medical curricula. Greater consistency of approach is needed between schools and countries to better safeguard standards of professional practice. From an international perspective these subjects are the focus of increasing attention as the nature of medical practice and regulation changes. This paper offers practical suggestions for raising the educational profile and integrating ethics, law and professionalism into medical curricula. Dealing with the subjects effectively during early medical training helps provide an appropriate grounding for future learning and practice.
Existen diferencias sustanciales entre las escuelas y los países en cuanto al papel de la ética, el derecho y el profesionalismo en los currículos de medicina. Entre las escuelas y los países se necesita una mayor consistencia en el enfoque para garantizar los estándares de la práctica profesional. Desde una perspectiva internacional, estos temas son el foco de creciente atención ya que la naturaleza de la práctica médica y su regulación han cambiado. Este documento ofrece sugerencias prácticas para elevar el perfil educativo y la integración de la ética, el derecho y el profesionalismo en los planes de estudio en Medicina. Hacer frente a estos temas de manera efectiva durante la formación médica temprana ayuda a proporcionar las bases apropiadas para el aprendizaje y la práctica futura.
In many countries, medical curricula include a formal, substantial component of ethics, law and professionalism to ensure that graduates are prepared for the roles they will eventually play as part of the health workforce, but the picture overall is uneven. As a construct, professionalism is relatively well understood, reflected in professional codes of conduct and shared understanding;1 however, it is not always clear if, when, where and how ethics and law, which underpin professionalism, fit in terms of formal instruction. We advocate the adoption of an integrated approach to teaching and learning for ethics, law and professionalism.2 These domains need to be consistently addressed in medical curricula, and educators may want to reflect on how best they fit alongside more firmly established scientific and clinical components of the curriculum.
The suggestions we make are about broad points of principle rather than fine detail. The latter is best worked out at local level, when local considerations relating to the regulation and accreditation of schools can be taken into account. While institutional factors, such as staffing and resource considerations have to be taken into account as well pressures on curriculum time and competing educational agenda, we acknowledge all of these difficulties when proffering advice on the development and implementation of ethics, law and professionalism curricula within schools of medicine. To help achieve this goal, we identify twelve key points for educators to consider, and if adopted these steps could help improve consistency in relation to both educational and professional standards (The authors define professionalism as a concept that applies to a category of persons, their attributes and behaviours, in [and possibly out of] the workplace. Unprofessional behaviours are those that fail to conform to normative standards set by an independently regulated profession, such as medicine).
1Agree where these subjects sit within a curriculumIntegration should be horizontal as well as vertical; for instance, ethics and law can be addressed as part of a professionalism theme (horizontal), alongside foundation and clinical sciences, which can be visited at regular intervals throughout the programme (vertical) as clinical reasoning gradually becomes more prominent. This approach is preferable to cramming materials into a short, intense course whereby information may not be retained and where it can appear to be disconnected from future health roles. Trainees do not want to find themselves in challenging situations without appropriate tools for solving problems, and it makes sense for curriculum content to be graduated, going from a taught, relatively factual base on to clinical scenarios where more complex judgments might have to be made. The more important topics should be reinforced at intervals throughout the course.
2Select the topics to be includedCurriculum time is necessarily limited, and topics need to be selected with a high degree of relevance to clinical practice. Few medical students are motivated by having abstract formulations to consider, especially if the language and the style are unfamiliar and too philosophical. Content can be grouped into categories to include topics such as patient rights, autonomy and consent, confidentiality and data protection, mental health and capacity, reproductive and end-of-life decision-making, health care organisation and delivery, and professional behaviour both in and out of the workplace.
3Agree on clear educational goals and learning outcomesLearning objectives should be clearly defined and matched to intended-learning outcomes. While the process may be time-consuming in the first instance, it is necessary step to take in order to meet external requirements for accreditation. For example, in the UK, the process is overseen by the medical regulator, and explicit requirements are set for ethics, law and professionalism.3 By contrast, in developing countries such as India and Pakistan, it is possible to graduate without ever having been taught or assessed in these areas. When doctors move across national boundaries, this poses a particular challenge, which can give rise to poor educational outcomes for trainees, who may be changing cultures as well as countries.
4Ensure that learning outcomes align with regulatory frameworksRegulatory frameworks are set at different levels (regional, federal, national and/or international), and most schools develop curriculum content in line with their own local guidelines. Bodies such as the World Medical Association or the United Nations Education, Scientific and Cultural Organization provide points of reference4,5 but standards should be grounded in such a way as to reflect local laws and values, as well as local structures for delivering health care. Universal templates cannot necessarily address these issues and could be based on assumptions about resources and values systems that simply do not apply. Balance, therefore, needs to be drawn between reliance on collective reasoning and local expertise. Since medical regulators and licensing boards typically accredit schools and programs, it is to them that educators should probably turn first.
5Ensure that teaching methods are consistent with the overall curriculum designIf a curriculum as a whole is integrated, then ethics, law and professionalism should consistently sit alongside scientific and clinical curriculum content. Learning methods need to be aligned by means of accompanying lectures and small-group case discussions, supplemented by on-line resources for self-directed learning.6-8 Mixed learning models, balancing classroom activity and lectures in the early stages, with opportunities for small-group discussion allowing time for reflection and case-based study in the later stages, work reasonably well. Interactive case discussion and panel debates help to engage students and make the subjects seem interesting and relevant. Although dedicated specialist staff would be needed in order to do justice to the subject, clinical tutors may also need to be involved.
6Articulate clearly how ethics and law relate to professionalismThe relationship between the domains of ethics, law and professionalism is not self-evident, and learners need to be clear what they are studying, and why. Overall, we argue that ethics and law are necessary and important components of professionalism, professionalism being concerned with attributes and behaviours, whereas medical ethics and law are more about social frameworks and points of reference. Since ethics and law are grounded within professionalism, these subjects may well overlap; however, not all challenges to professionalism are about ethics and law, and not all points of ethics and law directly address points of professionalism.
In our view, risks associated with not covering these topics adequately extend all the way to include patients being harmed through poor practice. While this is not the place to explore disciplinary procedures, it is important to consider the implications when someone fails to grasp these fundamental concepts. Patients can be affected and so can careers, and while there is no single ‘right’ approach to addressing poor professionalism, medical graduates do need adequate grounding in these areas in order to be appropriately mindful when going about their work later on. Responsibility for this enterprise is effectively shared between educator and trainee.
7Ensure that relevant learning outcomes are appropriately assessedAssessment matters, and if is it not dealt with properly, learners can be disadvantaged and the subject risks losing credibility. While attitudes typically precede behaviours, it is neither feasible nor desirable to try and assess attitudes. However, if and when attitudes manifest as troublesome behaviours, whether in the classroom or the clinic, schools need to take note and take appropriate action. The cultivation of high standards of professional conduct needs to begin as early as possible (e.g., before students go out on the wards), and this should be re-enforced continuously throughout the programme.9 The factual basis of ethics and law can be assessed with relative ease at the level of knowledge recall; however, more meaningful assessment tools need to be employed at the level of applied knowledge and reasoning and integrated into assessments for clinical management.
8Ensure progress decisions include achievement of professionalism learning outcomesUnless un-remediated poor professionalism has consequences, learners may deduce that this area of a curriculum is unimportant. Furthermore, low scores for assessments in ethics, law and professionalism should not be compensable by the achievement of high scores for scientific knowledge and clinical skill.
While a well-designed, stand-alone, high stakes exam has its place, the adoption of a coloured flag system for tracking problems, beginning early in the course, can prove to be effective. Under the scheme, learners with yellow flags face remediation, and those with several flags potentially face exclusion and/or even have to consider alternative careers. While remediation takes time and effort, peer pressure, mentoring support and multi-source feedback can be effective in producing remedial change, especially when used in combination.10 Such systems send a message to students that these subject areas should not just be ignored. Students typically make strategic choices in terms of which lectures to attend and which subjects to revise, and if a subject does not rank highly enough in their minds, then it will be ignored, including by those who most need the requisite the knowledge and understanding.
9Take steps to ensure that institutional regulations are robustSchools need to have robust processes in place in order to help minimise the risk of decisions being overturned on appeal. This entails checking to ensure that systems and processes are aligned internally within the university, as well as externally with affiliated institutions, such as teaching hospitals. While different parties to the wider enterprise of training doctors fulfil different roles, lack of congruity between and within institutions can lead to perverse outcomes. Disciplinary hearing outcomes are often challenged, and taking the necessary steps first should eventually save time, money and effort.
10Take into consideration the likely resource implicationsIn order for these areas to be properly taught and assessed, they need specialist staff. While staffing levels are linked to student numbers and budgets, leading the subject cannot easily be fitted around multiple other responsibilities. This is especially the case with the integrated approach, since teaching demands can occur at different points throughout the week (e.g., when classes need to be duplicated for different groups). However, the impact can partly be offset by enlisting support from faculty members with relevant interests and skills, as well as from part-time external experts. Additionally, clinical teachers may need occasional reminders to factor in ethical, legal and professional issues into case-based learning and teaching.
11Engage with students as an integral part of the processStudents need to be engaged in the process of curriculum development and evaluation, and if carefully managed there is no reason for this to result in confusion of roles.11 As with other subjects, dull teaching can translate into poor engagement and poor levels of attendance. Involving students in each stage of the process, including student representation on professionalism panels, should help to promote good practice, highlight poor teaching, and improve student engagement. Furthermore, if students are asked to comment on a programme or contribute towards the development and evaluation of a new curriculum, feedback should not be ignored by faculty if the integrity of the process is to be respected.
12Remember that professional development continues throughout someone's careerContinuing medical education increasingly plays a part in the life of a doctor. To this end, students need to be aware of the existence and purpose of the regulatory bodies, and it makes sense for representatives to talk with students prior to graduation. Learning and teachings for ethics, law and professionalism should not be restricted to either pre- or post-graduation. While grounding in these areas is an essential part of basic medical education, addressing them at regular intervals throughout someone's career, is equally important and should be of benefit to all concerned.
ConclusionEthics and law sit within the wider framework of professionalism; these subjects connect, and they need to be firmly established within basic medical education curricula, which means integrating them into learning and teaching using specialist staff. Education on these areas should continue after graduation as an essential part of continuing medical education. However, such an approach may be ineffective unless graduates have the opportunity to acquire an appropriate grounding in ethics, law and professionalism during early phases of their training. This rationale is equally applicable in developing and well as developed countries; failure to address educational inconsistencies, with the subjects under discussion sometimes being omitted altogether, is neither good for educational outcomes, nor for standards of professional practice more widely (Table 1).
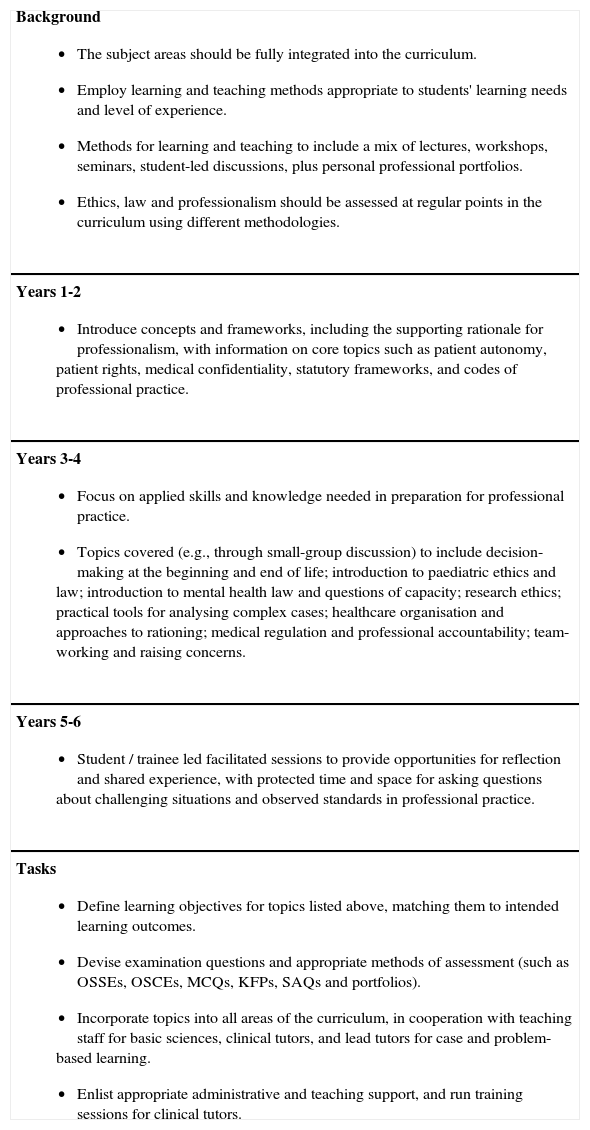
Suggested model for curriculum design for medical ethics, law and professionalism.
Background
|
Years 1-2
|
Years 3-4
|
Years 5-6
|
Tasks
|
- 1.
Determine where, when and how ethics, law and professionalism best fit within the programme as a whole.
- 2.
Make decisions on which topics to cover, when, and in what depth.
- 3.
Match intended learning outcomes to curriculum goals.
- 4.
Consider outcomes in relation to broader goals to try and achieve balance between collective wisdom and local contextual knowledge.
- 5.
Take steps to ensure that learning and teaching methods are appropriate to the task.
- 6.
Make clear to students why these subjects are taken seriously, and ensure they understand where ethics and law sit in relation to professionalism.
- 7.
Integrate methods of assessment into the broader curriculum as part of good practice for learning and teaching.
- 8.
Take steps to ensure that systems and procedures for remediation and progression from one stage are clear and robust.
- 9.
Apply institutional regulations fairly across the spectrum.
- 10.
Consider qualified staffing requirements including the training needs of tutors.
- 11.
Afford students the opportunity to play a part in curriculum development as well as learning and teaching and evaluations for professionalism.
- 12.
Help students to be aware of the role played by regulatory bodies prior to graduation, while emphasizing the importance of life-long learning.
RW: Wrote the first draft, including the table.
GB: Had extensive discussions with RW about ethical content.
RH: Contributed ideas on medical education and professionalism as well as suggestions for editing.
None of the authors received financial support that contributed to the writing of the paper.
None of the authors has any conflict of interest to disclose.
Ideas underpinning the paper were presented at the 16th Ottawa Conference on the Assessment of Competence in Medicine and the Healthcare Professions, Ottawa, Canada (2014), and at the 2014 Conference of the Australian and New Zealand Association for Health Professional Educators, Queensland, Australia.