

Literature on healthcare supply chain management has shown that the kanban system can provide significant benefits. However, very few benefits have been empirically demonstrated and the extent of each remains unknown. This study aims to measure nurses’ satisfaction with kanban systems in logistics of medical consumables and assesses possible advantages and differences among user groups through an anonymous survey at Hospital Universitario Virgen Macarena of Seville, Spain. Treatment of responses included an exploratory factor analysis, and a CAPTCA analysis. The results showed a high level of satisfaction for each aspect of the kanban system. Moreover, it highlighted the differences of opinion between groups of individuals according to workplace, nursing units, job category, seniority, age and kanban training. The exploratory factor analysis revealed that two factors underlie the collected assessments: the inherent advantages of a kanban system, and the logistics system performance as a whole. Thus, hospital managers should promote the implementation of kanban systems, since it increases nurses’ satisfaction and provides significant benefits.
La literatura sobre cadena de suministro en sanidad ha mostrado que el sistema kanban puede proporcionar importantes ventajas a las organizaciones sanitarias. Sin embargo, muy pocas de ellas se han demostrado y valorado empíricamente. Este trabajo tiene como objetivo medir la satisfacción de la enfermería con el sistema kanban, valorar cada una de sus posibles ventajas e identificar posibles diferencias entre diferentes grupos de usuarios. El trabajo ha consistido en realizar una encuesta anónima en el Hospital Universitario Virgen Macarena de Sevilla, España. El tratamiento de las respuestas incluye un análisis factorial exploratorio y un análisis CAPTCA. Los resultados muestran un alto nivel de satisfacción con cada aspecto del sistema kanban y la existencia de diferencias entre individuos según centro de trabajo, unidad de enfermería, categoría laboral, antigüedad, edad y formación en kanban. El análisis factorial exploratorio señala la existencia de dos factores subyacentes a las valoraciones recogidas: las ventajas inherentes del sistema kanban y el rendimiento del sistema logístico en su conjunto. Como conclusión, los directivos hospitalarios deberían promover la implantación de sistemas kanban ya que ello incrementa la satisfacción de enfermería y proporciona importantes beneficios.
The increased demand for health services, together with the economic realities, highlights concerns regarding public health system sustainability, making it necessary to seek maximum efficiency in their management. Patient care is supported by a wide array of activities including inventory management, purchasing, and the distribution of supplies to the point of care. These activities, referred to by many as healthcare logistics, or supply chain management, aim to ensure the delivery of the right products where and when needed, at the quality and quantity required to provide services while preventing any stock disruptions. As these logistic services use approximately 30–40% of the hospital's operating budget (Landry & Beaulieu, 2013), these activities are often cited as areas for improvement (Aguilar-Escobar & Garrido-Vega, 2013; Aguilar-Escobar, Garrido-Vega, & Godino-Gallego, 2013; Callender & Grassman, 2010). Logistics therefore become not only a source of savings in terms of support services, but may also render clinical professionals more productive as they can increase dedication to their daily work.
Various management tools have been used to improve logistic and supply chain services. In recent years, the Lean approach has experienced increasing popularity for the improvement of processes. Lean aims to focus on the value desired by the end-customer, to eliminate waste by identifying the value streams of the organization processes, to maintain a continuous flow or pull between process steps, and finally, to continuously improve (Womack & Jones, 2003). Due to Lean's success in the automotive and manufacturing industries, a significant number of other sectors, including services industries such as healthcare, started to adopt Lean principles (Aguilar-Escobar & Garrido-Vega, 2013; Domínguez-Machuca, González-Zamora, & Aguilar-Escobar, 2007a, 2007b; Spear, 2005). Lean principles have been proposed to bring considerable improvements in healthcare (Jarrett, 2006). A recent literature review on Lean applications in healthcare revealed that the most common areas of improvement included timeliness of service, cost reductions, productivity enhancements, and several quality aspects involving reduction in errors, and improved staff and patient satisfaction (Mazzocato, Savage, Brommels, Aronsson, & Thor, 2010).
The Lean approach can be viewed through two perspectives (Hines, Holweg, & Rich, 2004): at a strategic level, focusing on principles and organizational culture for long-lasting outcomes; and, at an operational level, focusing on tools and techniques. Various techniques have been linked to the Lean approach, such as just-in-time, resource reduction, improvement strategies, defect control, standardization, and scientific management practices (Pettersen, 2009). Accordingly, one of the most common and widely spread Lean tools is kanban (Adams & Ruiz-Ulloa, 2003).
The Japanese word kanban, meaning “signboard”, is a system that allows for the management of the overall supply chain by strategically and operationally linking production demands and the management of supplies. Kanban traces its roots to the early days of the Toyota Production System when Taiichi Ohno, a Vice President of Toyota, developed kanban cards to implement just in time (pull) production and minimize work in progress (WIP) by means of a simple visual tool. The kanban creates a “pull” material flow requiring employee participation to control and improve processes between workstations. The idea behind the kanban concept is that workstations produce/deliver desired components only when needed, thanks to a visual signal in the form of the reception of a card, box, or empty container (Sugimori, Kusunoki, Cho, & Uchikawa, 1977). Thus, kanban systems normally create cost reduction not only by eliminating waste, but also by being more responsive to change, facilitating quality control, and giving importance, trust and support to the employees running the processes (Chalice, 2007).
In hospitals, material distribution normally follows a periodic inventory system where material is replenished in batches. Some hospitals use exchange carts, or par level, but usually material distribution is a demand-based ordering system where nursing staff conduct regular inventory counts combined with consumption estimates. Products identified as low in inventory are noted on a requisition form that is then forwarded, either manually or electronically, to the material management department. Based on this requisition, required supplies are picked and shipped to the appropriate wards. Under this system, nursing personnel are often assigned the task of putting away the supplies in the storage units (Landry & Beaulieu, 2010).
Kanban started to appear in healthcare in the late 1980s through the development of a two-bin system (also called no-count), by Danish and Dutch companies (Landry & Philippe, 2004), for medical supplies.1 Thus, the quota of each item in this double-bin system is evenly distributed into two compartments. When one compartment is empty, the nurses use the second (or backup compartment), and identify that a bin has been emptied. Material handlers normally conduct rounds of the nursing units to be replenished according to a fixed schedule. Rather than drawing on their experience only and “eyeballing” the materials as with par level, the kanban card initiates replenishment for a predetermined quantity (Leone & Rahn, 2010). Thus, material handlers can simply scan the kanban cards and transfer the requests to the material management's information system. For items stored in the central warehouse, a pick list is generated from the material management's information system. For direct purchases (items sourced externally), a requisition is transmitted to suppliers. Finally, material handlers deliver medical supplies directly into the empty bins, thereby ensuring stock rotation in each unit. In a few hospitals, the scanning process (in the form of replenishment-ordering rounds) has been eliminated with the use of RFID-enabled kanban cards, which create an automatic replenishment request once the card is placed on the reader board (Bendavid, Boeck, & Philippe, 2010).
In hospitals, kanban has been used to manage medical supplies, commonly dispensed drugs, office supplies, linen and other commodities (Landry & Philippe, 2004; Persona, Battini, & Rafele, 2008). For many hospitals, kanban replenishment systems have given better inventory management results than traditional requisition-based methods using order on request, exchange carts, par level, or the more expensive automated cabinets (Graban, 2008; Landry & Beaulieu, 2010; Landry, Blouin, & Beaulieu, 2004; Leone & Rahn, 2010). Landry and Philippe (2004) found multiple benefits of the two-bin (kanban) system in their study of various replenishment systems in hospitals. The ordering process was faster, as there were built-in decision rules, no counting was required, and only empty compartments were scanned (or retrieved) by material handlers, thereby triggering the replenishment process. Furthermore, the use of kanban systems drastically reduced the material management workload of the nursing staff, and even eliminated it when material handlers were employed; thereby permitting nurses to focus on care rather than on material management activities. Moreover, as material handlers would spend less time in the nursing units and reduce product handling, there was less chance of disruption in clinical activities. Additional benefits, linked to the utilization of two-bin systems and point-of-use information, include the built-in stock rotation and lower average inventory levels which, in turn, reduced the number of expired products (Landry & Philippe, 2004). Another study of kanban implementation, in a hospital setting, showed considerable savings in terms of replenishment activities (Landry et al., 2004). In this kanban study, a material handler, in only 35min, would typically scan products in 18 stocking locations spread across nine wards, which was four to seven times faster than in traditional systems. In summary, several benefits linked to kanban usage in healthcare settings have been found. Among these we can highlight: acceleration of the ordering process, better organization of storage, fewer expired items, and less work for the nursing personnel (Graban, 2008; Khorajia, Farris, & Haas, 2009; Landry & Beaulieu, 2010; Landry et al., 2004; Landry & Philippe, 2004; Persona et al., 2008). All these benefits exert a positive influence on supply chain performance and should lead to greater work satisfaction of nurses. One way to measure this satisfaction could be to collect opinions about potential benefits and overall satisfaction of the nursing staff towards kanban systems. Several authors believe that internal customer satisfaction should be included in the primary indicators of supply chain performance (Aguilar-Escobar et al., 2013; Gunasekaran, Patel, & McGaughey, 2004; Heikkilä, 2002; Otto & Kotzab, 2003). Additionally, several studies (Heinbuch, 1995) have shown that materials management should focus on internal customers of the hospital, such as nurses, doctors, and administrative staff. They even suggested the need for logistics managers to prove that internal customer demands were met and satisfaction evaluated (Heinbuch, 1995). Some authors have suggested and tested (Murrells, Clinton, & Robinson, 2005; Penz, Stewart, D’Arcy, & Morgan, 2008) that the failure to have adequate supplies influences the work satisfaction of the nursing staff since this failure prevents them from providing quality care. However, to the best of our knowledge, very little literature has focused on evaluating, analysing and empirically proving that nursing personnel are satisfied with kanban implementations and that this system provides the expected results in supply management. Consequently, this paper seeks to further investigate nurses’ satisfaction and evaluate potential advantages of kanban systems in hospital supply chains. Additionally, two complementary objectives are studied: (1) to see whether there are satisfaction level differences between user groups; and (2) to determine whether the original 12 variables used in the study can be reduced to only a few factors (2 or 3). To achieve these goals, we conducted a survey of nursing staff at AHVM.
2Methodology2.1Case study and data collectionThis study was conducted in a 955-bed hospital group, Hospital Universitario Virgen Macarena y Área (AHVM), located in Seville, Spain between December 2012 and March 2013. At that time, the AHVM had 2 hospitals, 3 specialized centres, and 27 operating theatres. In 2006, the AHVM developed a comprehensive logistics plan that included the creation of a logistics platform in 2007 and the implementation of a kanban system (Aguilar-Escobar & Garrido-Vega, 2013).
Prior to the implementation of the kanban system, the nursing supervisor in each department took care of ordering material using a procurement informatics system that transmitted replenishment requests to the logistics and purchasing department. On average, they would place material orders once a week. There was no standardized process; each nursing supervisor would order with variable frequencies and quantities. However, it was agreed that the order quantity should not exceed one month's consumption for items that had no location in the central store (Type 1), and 15 days for items that did have a location (Type 2). The financial management department supervised and authorized each order. The implementation of the modular double-bin (kanban) shelving units completely changed their replenishment system. This new ergonomical system provided the possibility of easy access to both first bin and second bin locations, of configurable size. Each first bin was identified with a label that included critical information such as the location number, product name, code, quantity and a bar code. The bar code included the product code, the location and cost centre. The information contained on the label was unique for each item and standardized within the hospital group. The second bin was identical to the first bin. Once a bin was empty, the nursing personnel was responsible for turning the first bin label from the white to the red side to indicate a replenishment need, and proceeded to use the material located in the second bin. The logistics clerks were now responsible for the replenishment orders in the units. They passed through each unit according to a specific schedule. The logistic clerks completed their rounds by scanning all the red tags in the units and the associated information was directly uploaded to the system via Wi-Fi. This created replenishment orders to the central material store. Orders were now more frequent, twice instead of once per week, thereby generating the need to offer break-bulk picking. In cases of exceptionally high usage, the system allowed additional requests which prevented potential stock-outs. The orders were prepared and delivered the same day by logistic clerks. The materials were brought to the units, unboxed and placed into the bins. The clerks would also move the remaining material from the second to the first bin and replenish the second bin; thereby ensuring stock rotation was completed. Once this last step was accomplished, the logistic clerks turned the labels to show the white side to indicate that the item had been replenished. The whole process, from the bar code reading to the replenishment, normally took under 24h.
The AHVM's finance and administration manager ordered the procurement and logistics distribution department to implement the kanban system in 36 stores. The project started in early February 2010 with a first pilot implementation and ended in late August 2010 with activities such as analysis, planning, software development, and procurement. From mid-November 2010 to mid-November 2011, the kanban system was implemented in the remaining 35 stores with an average of 3 implementations per month (one every 10 days). Currently, the AHVM has implemented the kanban system in 60% of their stores (i.e. 36 of a total of 60 stores). The main criteria to determine whether the store was to receive a kanban system, were the existence of a minimum storage space of 5m2 and that the store contained medical consumables.
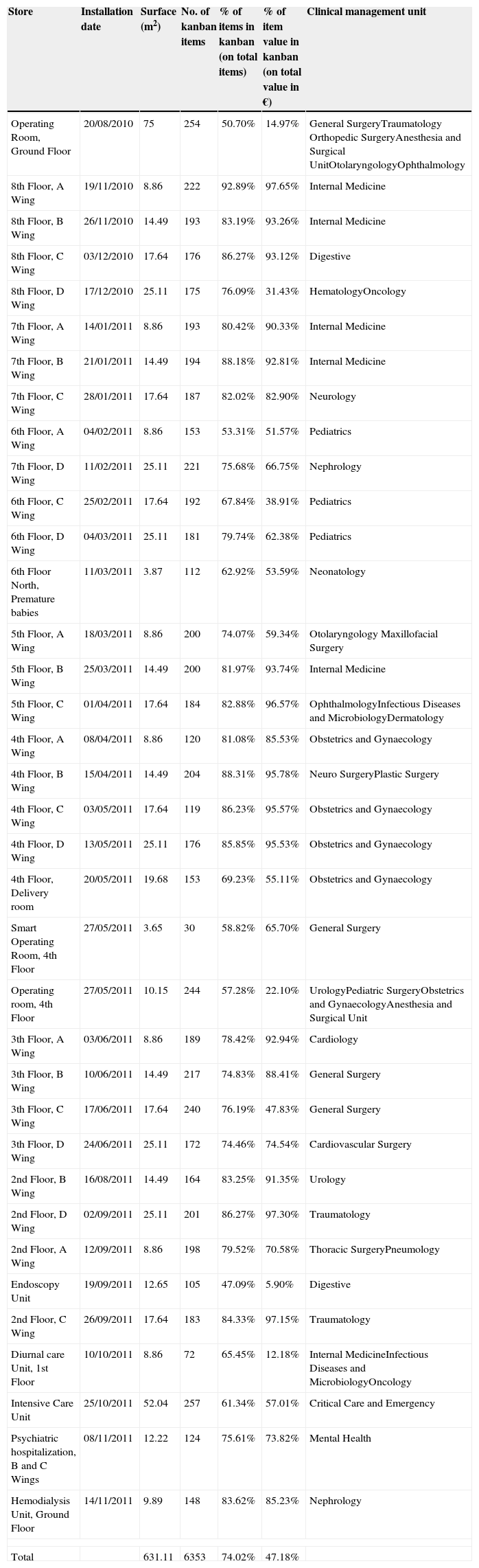
Table 1 shows the kanban stores that have been implemented, the implementation date, the number of items within the kanban system, the percentage of items in the kanban system on the total amount of items, and finally the percentage representing the value of items in the kanban system on the total stock value in the year 2013 (weighted average value in euros).
Description of the various stores that had implemented kanban by April 2014.
| Store | Installation date | Surface (m2) | No. of kanban items | % of items in kanban (on total items) | % of item value in kanban (on total value in €) | Clinical management unit |
|---|---|---|---|---|---|---|
| Operating Room, Ground Floor | 20/08/2010 | 75 | 254 | 50.70% | 14.97% | General SurgeryTraumatology Orthopedic SurgeryAnesthesia and Surgical UnitOtolaryngologyOphthalmology |
| 8th Floor, A Wing | 19/11/2010 | 8.86 | 222 | 92.89% | 97.65% | Internal Medicine |
| 8th Floor, B Wing | 26/11/2010 | 14.49 | 193 | 83.19% | 93.26% | Internal Medicine |
| 8th Floor, C Wing | 03/12/2010 | 17.64 | 176 | 86.27% | 93.12% | Digestive |
| 8th Floor, D Wing | 17/12/2010 | 25.11 | 175 | 76.09% | 31.43% | HematologyOncology |
| 7th Floor, A Wing | 14/01/2011 | 8.86 | 193 | 80.42% | 90.33% | Internal Medicine |
| 7th Floor, B Wing | 21/01/2011 | 14.49 | 194 | 88.18% | 92.81% | Internal Medicine |
| 7th Floor, C Wing | 28/01/2011 | 17.64 | 187 | 82.02% | 82.90% | Neurology |
| 6th Floor, A Wing | 04/02/2011 | 8.86 | 153 | 53.31% | 51.57% | Pediatrics |
| 7th Floor, D Wing | 11/02/2011 | 25.11 | 221 | 75.68% | 66.75% | Nephrology |
| 6th Floor, C Wing | 25/02/2011 | 17.64 | 192 | 67.84% | 38.91% | Pediatrics |
| 6th Floor, D Wing | 04/03/2011 | 25.11 | 181 | 79.74% | 62.38% | Pediatrics |
| 6th Floor North, Premature babies | 11/03/2011 | 3.87 | 112 | 62.92% | 53.59% | Neonatology |
| 5th Floor, A Wing | 18/03/2011 | 8.86 | 200 | 74.07% | 59.34% | Otolaryngology Maxillofacial Surgery |
| 5th Floor, B Wing | 25/03/2011 | 14.49 | 200 | 81.97% | 93.74% | Internal Medicine |
| 5th Floor, C Wing | 01/04/2011 | 17.64 | 184 | 82.88% | 96.57% | OphthalmologyInfectious Diseases and MicrobiologyDermatology |
| 4th Floor, A Wing | 08/04/2011 | 8.86 | 120 | 81.08% | 85.53% | Obstetrics and Gynaecology |
| 4th Floor, B Wing | 15/04/2011 | 14.49 | 204 | 88.31% | 95.78% | Neuro SurgeryPlastic Surgery |
| 4th Floor, C Wing | 03/05/2011 | 17.64 | 119 | 86.23% | 95.57% | Obstetrics and Gynaecology |
| 4th Floor, D Wing | 13/05/2011 | 25.11 | 176 | 85.85% | 95.53% | Obstetrics and Gynaecology |
| 4th Floor, Delivery room | 20/05/2011 | 19.68 | 153 | 69.23% | 55.11% | Obstetrics and Gynaecology |
| Smart Operating Room, 4th Floor | 27/05/2011 | 3.65 | 30 | 58.82% | 65.70% | General Surgery |
| Operating room, 4th Floor | 27/05/2011 | 10.15 | 244 | 57.28% | 22.10% | UrologyPediatric SurgeryObstetrics and GynaecologyAnesthesia and Surgical Unit |
| 3th Floor, A Wing | 03/06/2011 | 8.86 | 189 | 78.42% | 92.94% | Cardiology |
| 3th Floor, B Wing | 10/06/2011 | 14.49 | 217 | 74.83% | 88.41% | General Surgery |
| 3th Floor, C Wing | 17/06/2011 | 17.64 | 240 | 76.19% | 47.83% | General Surgery |
| 3th Floor, D Wing | 24/06/2011 | 25.11 | 172 | 74.46% | 74.54% | Cardiovascular Surgery |
| 2nd Floor, B Wing | 16/08/2011 | 14.49 | 164 | 83.25% | 91.35% | Urology |
| 2nd Floor, D Wing | 02/09/2011 | 25.11 | 201 | 86.27% | 97.30% | Traumatology |
| 2nd Floor, A Wing | 12/09/2011 | 8.86 | 198 | 79.52% | 70.58% | Thoracic SurgeryPneumology |
| Endoscopy Unit | 19/09/2011 | 12.65 | 105 | 47.09% | 5.90% | Digestive |
| 2nd Floor, C Wing | 26/09/2011 | 17.64 | 183 | 84.33% | 97.15% | Traumatology |
| Diurnal care Unit, 1st Floor | 10/10/2011 | 8.86 | 72 | 65.45% | 12.18% | Internal MedicineInfectious Diseases and MicrobiologyOncology |
| Intensive Care Unit | 25/10/2011 | 52.04 | 257 | 61.34% | 57.01% | Critical Care and Emergency |
| Psychiatric hospitalization, B and C Wings | 08/11/2011 | 12.22 | 124 | 75.61% | 73.82% | Mental Health |
| Hemodialysis Unit, Ground Floor | 14/11/2011 | 9.89 | 148 | 83.62% | 85.23% | Nephrology |
| Total | 631.11 | 6353 | 74.02% | 47.18% | ||
The average store size, for the 36 implemented kanban systems, was of 17.5m2, and the median (which is representative of a typical store size) was of 14.5m2. Not all medical consumables used in the units were within the kanban system. Of a total of 8583 logistic locations (there is only one logistic location per stock-keeping unit (SKU) in each store unit), 6353 (74.02% of the total) corresponded to products on the kanban (double-bin) shelves, and 2230 (25.98%) on conventional shelving that was managed using a traditional replenishment system.
The annual item consumption of these 36 units in 2013 was of € 5,365,644 and the proportion found within the kanban system was of € 2,531,511 (47.18%). This is an ostensibly low average considering the overall consumption as a whole due to the high economic value of certain surgical products that are neither in the kanban system nor have a location in the central or unit store. These products are expensive and are therefore only ordered on demand. Accordingly, there was little interest in incorporating items with low turnover rates into the kanban system as this would only have increased the inventory and the number of expired goods.
The investment made by FEDER, Funds of the European Union, following these 36 implementations of modular double-bin shelving units was of € 186,408.2, representing an average cost of € 5178 per store.
2.2SurveyThe survey was developed to explore and measure the various aspects that define satisfaction levels in the kanban system. The aspects, selected to be valued, were based on a satisfaction survey in healthcare logistic services (Aguilar-Escobar et al., 2013) and adapted to the kanban system with the addition of four new questions. The data collection took place between February 2013 and April 2013 in all units that had completed their kanban implementation (26 different departments distributed between the San Lazaro and Macarena Hospitals). It comprised general information on the respondent, including the name of the unit in which they worked, their job category, seniority range, age range, whether they had received training on kanban systems, and whether they had worked in the hospital prior to the implementation of the kanban system. The survey requested their responses to a list of 12 statements (see the survey in Appendix) using a 10-point Likert scale (ranging from “completely disagrees” to “totally agrees”).
The target population using the kanban system in this hospital was of 1123 people (nursing staff). By using simple random sampling from a finite population, we obtained a total of 208 surveys, giving us a response rate of 18.52%. The sampling error was of ±6.1% for a confidence level of 95%.
With the data obtained from these surveys, a descriptive and exploratory factor analysis was conducted including multiple means comparisons (ANOVA and Student's t-test) using SPSS 22. Prior to the completion of the contrasts, we performed Levene's test for the equality of variances before carrying out the Student's t-test for the equality of means and ANOVA analysis. Due to the test outcome, the Brown–Forsythe test was chosen instead of the classic ANOVA analysis, since it presents robustness to unequal variances. Following the results, it was decided that the Tukey or Games–Howell tests were appropriate to carry out the contrasts (or comparisons) a posteriori. In order to group the variables into representative factors, we conducted a Factorial Analysis. Subsequently, a Categorical Principal Components Analysis (CAPTCA) was carried out to confirm the previous results.
3FindingsWe now present the results and analysis starting with the characteristics of our sample, the satisfaction levels of hospital staff with the kanban system, a descriptive analysis of satisfaction levels, satisfaction level comparisons between different groups, an exploratory factor analysis, and a CAPTCA analysis.
3.1Sample characterizationAs previously stated, the characteristics of the sample of the study were based on the 208 surveys gathered at AHVM. We obtained 16 surveys (7.7%) from the San Lazaro Hospital and 192 (92.3%) were obtained in the Macarena Hospital. When analysing the various units that had responded, 59.1% of the respondents worked in a clinical unit and 40.9% in surgical services or intensive care. The job categories represented within the 205 respondents were: 12 head nurses (5.9%), 98 nurses (47.8%), 94 auxiliary nurses (45.9%), and 1 (0.5%) in another category. The seniority analysis showed that 114 of the respondents had been working in the hospital for more than 20 years (57.3%), 38 people had between 15 and 19 years of service (19.1%), 29 people had between 10 and 14 years (14.6%), 16 people between 5 and 9 years (8%), and 2 people had less than 5 years of seniority (1%). Nine of the 208 respondents did not answer the seniority question. Moreover, when asked whether they had worked in the hospital prior to the implementation of the kanban system, the results indicated that 164 respondents had (82%) and 36 had not (18%) worked in the hospital prior to the implementation.
In relation to the respondent's age, 12 workers were 60 years old or over (5.9%), 78 were between 50 and 59 years old (38.2%), 81 were between 40 and 49 years old (38.9%), 31 were between 30 and 39 years old (14.9%), 2 were under 30 years old (1%), and finally 4 workers did not respond to the question. These results combined with seniority demonstrate a worrying sign of ageing and non-renewal of nursing in the Spanish public system. Lastly, we asked about kanban training, an aspect of importance for the proper use of this system. In this regard, 140 respondents reported having received training (69.3%) compared to 62 that indicated otherwise (30.7%), while 6 did not respond to the question.
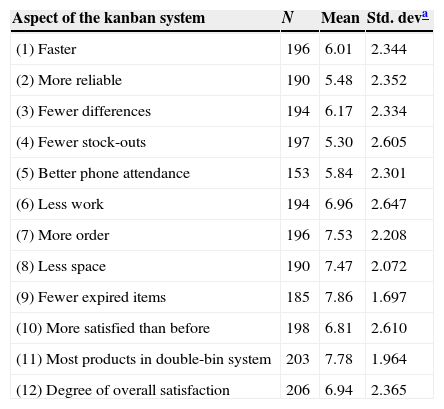
3.2Descriptive analysis of the hospital staff satisfaction with the kanban systemAs stated in Section 2.2, the respondent's satisfaction level with the kanban system was analysed through 12 valuation questions. The first 10 questions were formulated as a comparison between the kanban system and the initial replenishment system. Thus, these questions could only be answered by those who worked in the hospital prior to the kanban implementation. Question 11 enquired whether the majority of the products were found in the double-bin system and question 12 made a general satisfaction assessment. Table 2 shows the number of responses (N), means and standard deviations (Std. dev.) corresponding to each of the 12 valuation questions.
Main descriptive statistics for the valuation question.
| Aspect of the kanban system | N | Mean | Std. deva |
|---|---|---|---|
| (1) Faster | 196 | 6.01 | 2.344 |
| (2) More reliable | 190 | 5.48 | 2.352 |
| (3) Fewer differences | 194 | 6.17 | 2.334 |
| (4) Fewer stock-outs | 197 | 5.30 | 2.605 |
| (5) Better phone attendance | 153 | 5.84 | 2.301 |
| (6) Less work | 194 | 6.96 | 2.647 |
| (7) More order | 196 | 7.53 | 2.208 |
| (8) Less space | 190 | 7.47 | 2.072 |
| (9) Fewer expired items | 185 | 7.86 | 1.697 |
| (10) More satisfied than before | 198 | 6.81 | 2.610 |
| (11) Most products in double-bin system | 203 | 7.78 | 1.964 |
| (12) Degree of overall satisfaction | 206 | 6.94 | 2.365 |
Table 2 also presents the high average (6.94) of the overall satisfaction assessment linked to the kanban system implementation. Interestingly, another survey on logistics system satisfaction in the same hospital gave a global satisfaction assessment value of 6.7 which was already considered a high score by the authors (Aguilar-Escobar et al., 2013). Moreover, in a similar work by Newell, Steinmetz-Malato, and Van Dyke (2011), an average satisfaction of 3.1 on a scale of 0–5 was obtained.
Likewise, the remaining survey questions presented considerably high response means. The aspect most valued by respondents was that kanban systems generated fewer expired items compared to conventional systems (with an average value of 7.9). In addition, the survey questions that gathered an average of over 6.9 were those that stated that kanban systems made stores more orderly (7.53), required less store space (7.47), and resulted in less work for nursing personnel (6.96). Thus, question 10 comparing kanban with the previous system reached a high average value of 6.81. Three questions presented an average below 6.2, which were being the questions concerning reduced stock-outs (with a mean value of 5.3), increased reliability (5.48) and improved phone attendance (5.84).
Moreover, it was observed that the standard deviations were always less than half of the corresponding average, and hence it can be concluded that dispersions were relatively small.
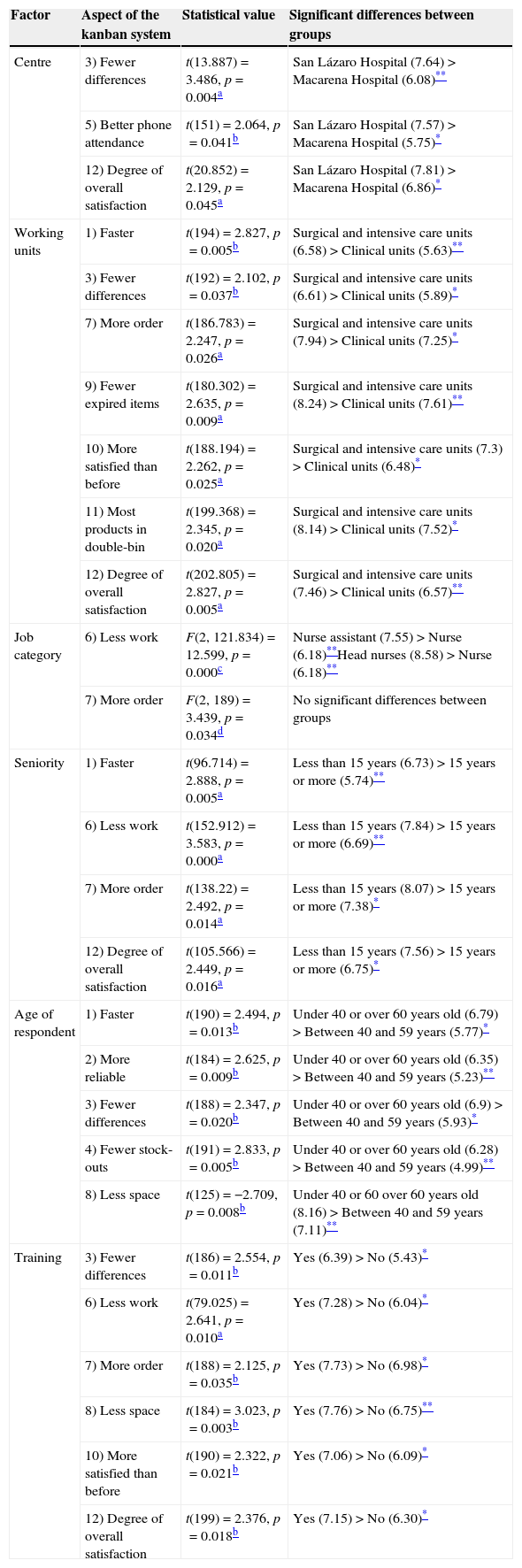
3.3Satisfaction-level comparisons between different groupsIn order to determine whether demographic variables, considered in the study, had an impact on the level of satisfaction, we carried out various contrasts to test the differences between groups. Table 3 summarizes the satisfaction analysis including the comparison between groups for each aspect. The last column shows the significant differences between groups, the mean value (shown in parentheses, on a scale of 0–10), the difference direction (> higher, < smaller) and the statistical significance level (*, **).
Comparisons between groups.
| Factor | Aspect of the kanban system | Statistical value | Significant differences between groups |
|---|---|---|---|
| Centre | 3) Fewer differences | t(13.887)=3.486, p=0.004a | San Lázaro Hospital (7.64)>Macarena Hospital (6.08)** |
| 5) Better phone attendance | t(151)=2.064, p=0.041b | San Lázaro Hospital (7.57)>Macarena Hospital (5.75)* | |
| 12) Degree of overall satisfaction | t(20.852)=2.129, p=0.045a | San Lázaro Hospital (7.81)>Macarena Hospital (6.86)* | |
| Working units | 1) Faster | t(194)=2.827, p=0.005b | Surgical and intensive care units (6.58)>Clinical units (5.63)** |
| 3) Fewer differences | t(192)=2.102, p=0.037b | Surgical and intensive care units (6.61)>Clinical units (5.89)* | |
| 7) More order | t(186.783)=2.247, p=0.026a | Surgical and intensive care units (7.94)>Clinical units (7.25)* | |
| 9) Fewer expired items | t(180.302)=2.635, p=0.009a | Surgical and intensive care units (8.24)>Clinical units (7.61)** | |
| 10) More satisfied than before | t(188.194)=2.262, p=0.025a | Surgical and intensive care units (7.3)>Clinical units (6.48)* | |
| 11) Most products in double-bin | t(199.368)=2.345, p=0.020a | Surgical and intensive care units (8.14)>Clinical units (7.52)* | |
| 12) Degree of overall satisfaction | t(202.805)=2.827, p=0.005a | Surgical and intensive care units (7.46)>Clinical units (6.57)** | |
| Job category | 6) Less work | F(2, 121.834)=12.599, p=0.000c | Nurse assistant (7.55)>Nurse (6.18)**Head nurses (8.58)>Nurse (6.18)** |
| 7) More order | F(2, 189)=3.439, p=0.034d | No significant differences between groups | |
| Seniority | 1) Faster | t(96.714)=2.888, p=0.005a | Less than 15 years (6.73)>15 years or more (5.74)** |
| 6) Less work | t(152.912)=3.583, p=0.000a | Less than 15 years (7.84)>15 years or more (6.69)** | |
| 7) More order | t(138.22)=2.492, p=0.014a | Less than 15 years (8.07)>15 years or more (7.38)* | |
| 12) Degree of overall satisfaction | t(105.566)=2.449, p=0.016a | Less than 15 years (7.56)>15 years or more (6.75)* | |
| Age of respondent | 1) Faster | t(190)=2.494, p=0.013b | Under 40 or over 60 years old (6.79)>Between 40 and 59 years (5.77)* |
| 2) More reliable | t(184)=2.625, p=0.009b | Under 40 or over 60 years old (6.35)>Between 40 and 59 years (5.23)** | |
| 3) Fewer differences | t(188)=2.347, p=0.020b | Under 40 or over 60 years old (6.9)>Between 40 and 59 years (5.93)* | |
| 4) Fewer stock-outs | t(191)=2.833, p=0.005b | Under 40 or over 60 years old (6.28)>Between 40 and 59 years (4.99)** | |
| 8) Less space | t(125)=−2.709, p=0.008b | Under 40 or 60 over 60 years old (8.16)>Between 40 and 59 years (7.11)** | |
| Training | 3) Fewer differences | t(186)=2.554, p=0.011b | Yes (6.39)>No (5.43)* |
| 6) Less work | t(79.025)=2.641, p=0.010a | Yes (7.28)>No (6.04)* | |
| 7) More order | t(188)=2.125, p=0.035b | Yes (7.73)>No (6.98)* | |
| 8) Less space | t(184)=3.023, p=0.003b | Yes (7.76)>No (6.75)** | |
| 10) More satisfied than before | t(190)=2.322, p=0.021b | Yes (7.06)>No (6.09)* | |
| 12) Degree of overall satisfaction | t(199)=2.376, p=0.018b | Yes (7.15)>No (6.30)* |
In relation to the centre (hospital location) where the nurses work, we applied a Student's t-test comparing the means of independent samples. There were significant differences between questions (3) Fewer differences, (5) Better phone attendance, and (12) Degree of overall satisfaction, with a constant higher valuation in the San Lazaro Hospital compared to that of the Macarena Hospital. The reason for this higher valuation may be linked to the fact that the first kanban store was implemented in the newly opened San Lazaro Hospital operating rooms, thereby replacing several small outdated stores.
We then applied a Student's t-test by comparing the means of independent samples for informants from both centres grouped into two working unit categories: surgical/intensive care units and clinical units. As seen in Table 3, 7 of the 12 survey questions showed significant differences. Furthermore, all aspects showed higher values for the surgical and intensive care compared to the clinical respondents. More specifically, there was high overall satisfaction (question 12) of the kanban system in Intensive Care units, General Surgery and Traumatology with scores of 8.6, 8.29 and 7.30. In contrast, for the clinical respondents, the overall satisfaction of nursing staff in Dermatology, Gastroenterology and Endoscopy was of 4.75, 4.75 and 5.33, which greatly decreased the group average.
Concerning the job category, mean comparisons between groups showed significant differences in two aspects (see Table 3): (6) less work and (7) more order. In both aspects, nurses put lower valuation scores compared to the head nurses. Additionally, for question 6, where kanban is said to generate less work, auxiliary nurses gave a higher valuation than nurses. The case study showed that both the head nurses and auxiliary nurses enjoyed the greatest time-saving. Head nurses eliminated inventory counts and order forms from their workload. Moreover, unpacking and placing merchandise were no longer the responsibility of auxiliary nurses.
When analysing the data in relation to seniority in the workplace, we simplified the analysis by separating the respondents into two groups: those with less than 15 years of experience and those with 15 or more. As shown in Table 3, the independent sample Student's t-test that compares the means showed that there were significant differences in four aspects, which were always higher in the group with less seniority.
Similarly to the seniority analysis, we distinguished respondents between two age groups: those under 40, and those 60 years old or more (“youngest and oldest”); and those between 40 and 59 years old. We compared means using an independent sample Student's t-test. As shown in Table 3, there were significant differences in five aspects. In each case the average rating was always higher in the “youngest and oldest” group. It may also be that the middle age group is more critical towards the health system as a whole.
Finally, with regard to those that had received training (Yes) or not (No), we compared the means using a Student's t-test (see Table 3) and found that there were significant differences in six variables. All aspects showed a higher average rating for the group that had received training. This result emphasized the importance of providing training on kanban system procedures to ensure good performance and high nursing satisfaction with the system.
3.4Exploratory factor and CAPTCA analysisIn order to analyse all the items within our “satisfaction level” construct, the 12 aspects were subjected to an exploratory factor analysis. Both the Kaiser–Meyer–Olkin test, which gave a value of 0.907 above the recommended 0.6 (Tabachnick & Fidell, 2007), and the Bartlett test of sphericity, which was statistically significant (p=0.000), indicated that our sample was appropriate for this type of analysis. Moreover, our sample size surpassed the recommended minimum of 10 observations per item for these types of tests (Nunnally, 1978).
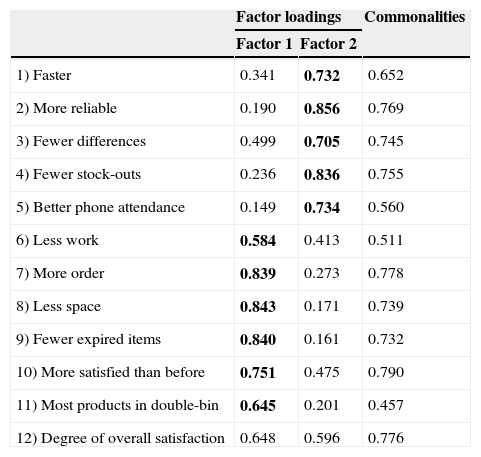
The principal component analysis showed two factors when applying eigenvalues greater than 1. The first factor (which included the aspects contained in questions 6, 7, 8, 9, 10 and 11) accounted for 56.93% of the variance. The second factor (which included questions 1, 2, 3, 4 and 5) accounted for 11.93% of the variance. Therefore, these two components together accounted for 68.86% of the explained variance. As seen, question 12, being the general satisfaction, could be included in either the first or the second factor.
Table 4 presents the factor loadings and communalities for the two-factor solution.
Principal component analysis (two factors).
| Factor loadings | Commonalities | ||
|---|---|---|---|
| Factor 1 | Factor 2 | ||
| 1) Faster | 0.341 | 0.732 | 0.652 |
| 2) More reliable | 0.190 | 0.856 | 0.769 |
| 3) Fewer differences | 0.499 | 0.705 | 0.745 |
| 4) Fewer stock-outs | 0.236 | 0.836 | 0.755 |
| 5) Better phone attendance | 0.149 | 0.734 | 0.560 |
| 6) Less work | 0.584 | 0.413 | 0.511 |
| 7) More order | 0.839 | 0.273 | 0.778 |
| 8) Less space | 0.843 | 0.171 | 0.739 |
| 9) Fewer expired items | 0.840 | 0.161 | 0.732 |
| 10) More satisfied than before | 0.751 | 0.475 | 0.790 |
| 11) Most products in double-bin | 0.645 | 0.201 | 0.457 |
| 12) Degree of overall satisfaction | 0.648 | 0.596 | 0.776 |
Extraction method: Principal Component Analysis.
Rotation method: Varimax with Kaiser Normalization.
Rotation converged in three iterations.
Alpha de Cronbach: Factor 1=0.876, Factor 2=0.893: variance explained=68.862%.
The highest loading for each item (except 12) is indicated by bold characters.
The first factor appears to group aspects related to the kanban system and its inherent advantages such as: less nursing work, more organized storage, less storage space, fewer expired items, increased internal customer satisfaction, and incorporation of a majority of products in the system. In our view, the second factor grouped other variables that were more relevant to the performance of the AHVM hospital logistics system. Indeed, this factor included the following aspects: faster and more reliable deliveries, fewer differences, fewer stock-outs, and better phone attendance.
We measured the survey's internal consistency with these two factors and obtained a Cronbach's alpha of 0.876 for the first factor and 0.893 for the second factor. These values are high (close to 1), thereby demonstrating the high reliability of the measurement scale used in this survey.
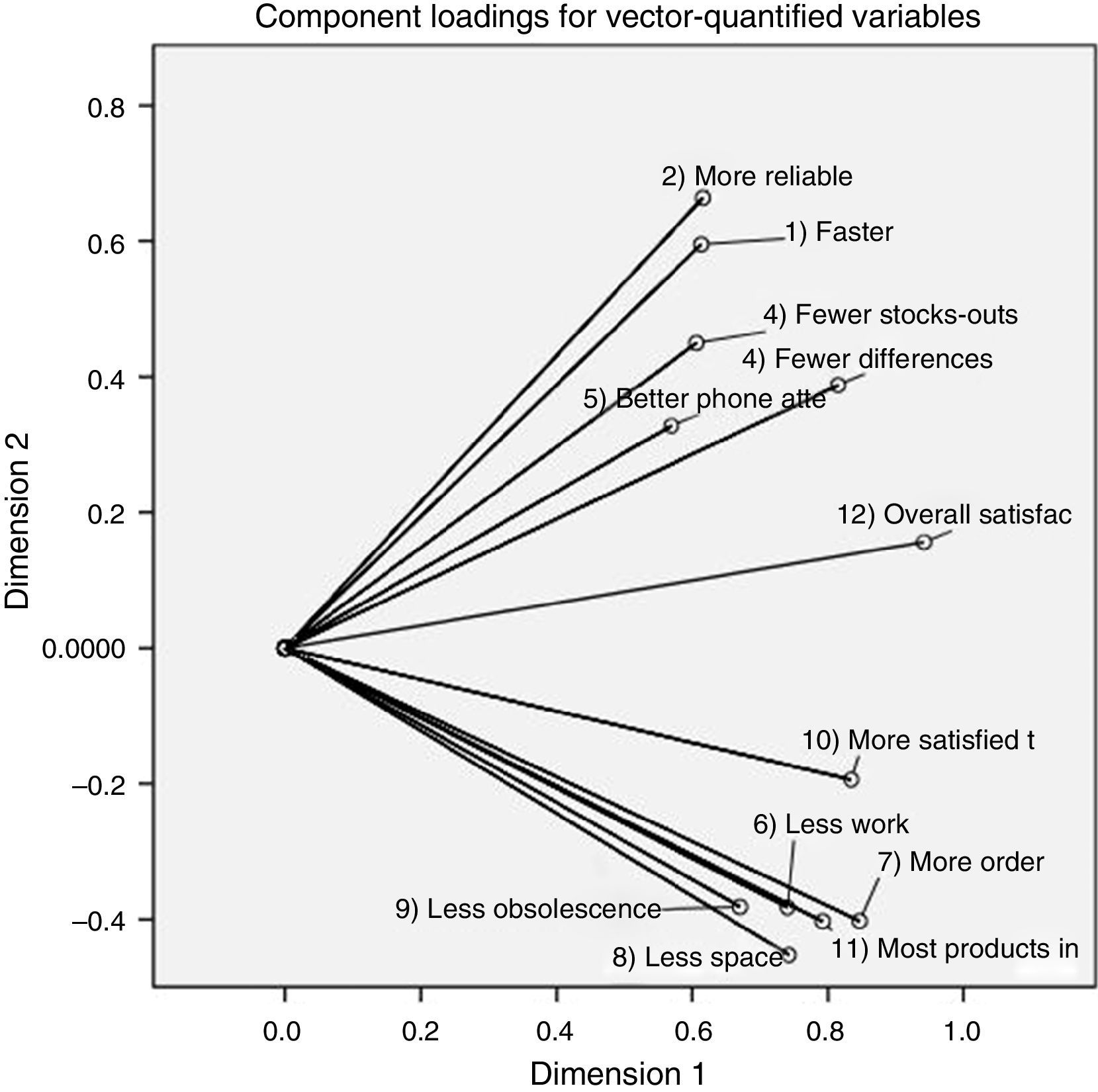
In order to statistically contrast these results, a Categorical Principal Components Analysis (CATPCA) was performed grouping variables in two representative factors. Fig. 1 shows a two-dimensional space and the component loadings for each of the variables. The observed clustering is explained with the angles between vectors showing that the smaller the angle between a pair of vectors, the greater the association between the variables represented. Thus, the first five variables (from 1 to 5) are grouped on one side, and identify the advantages of the kanban system itself, and the other six variables (from 6 to 11) on the other side identify the performance of the logistics system. Question 12 is a result of both, thereby indicating that satisfaction of nursing staff is influenced by both satisfaction with the kanban system and the logistics system performance.
4Discussion
This paper aimed to further investigate nursing personnel satisfaction towards kanban systems in hospital supply chains. Our main objective was to measure nursing personnel satisfaction levels and see whether they positively or negatively valued implementation of kanban systems to solve logistic problems. Our findings showed high overall levels of satisfaction with the kanban system (6.94 out of 10). Moreover, the new kanban system received higher satisfaction levels than the previous replenishment system (6.81). Indeed, the survey showed a positive appreciation in all aspects evaluated, since all valuations remain above 5, on a 0–10 Likert scale. These results confirm that the kanban system received a positive evaluation and this has a positive influence on job satisfaction on the part of nursing staff because it enables them to provide quality services to patients (Murrells et al., 2005; Penz et al., 2008).
Our first complementary objective was to verify whether there were differences in the level of satisfaction between user groups. In this regard, the work centres (specific hospital), work unit, the job category, the seniority, and the age of the respondent and training were found to be determinants of opinion.
Our second complementary objective was to determine which factors, principal components, or dimensions of satisfaction, could reduce the original variables used in the study. According to the principal component analysis, all the questions in the survey were influenced by two factors that could be called inherent advantages of a kanban system (less work, more order, less space, fewer expired items and increased customer satisfaction) and logistics system performance (faster, more reliable, fewer differences, fewer stock-outs, and better phone attendance). The hospital logistics department provided support services for the kanban system. Interestingly, nursing personnel determined that aspects 1, 2, 3, 4 and 5 were less dependent on the kanban system but rather on the logistics system. Moreover, managers that implemented a kanban system could improve nursing staff satisfaction, especially that related to aspects 6, 7, 8, 9 and 10. The kanban system promoted a major increase in satisfaction in comparison with the conventional system, and both factors (kanban implementation and good logistics system) improved nursing staff satisfaction. Therefore, based on the difference in valuation of the items and on the exploratory analysis, we deduce that the main advantages of the kanban system for healthcare logistics are that: nursing work linked to material management is minimized (question 6), stores are more orderly (question 7), less space is required in stores (question 8), and there are fewer expired items (question 9). These results are consistent with those obtained by other authors (Graban, 2008; Khorajia et al., 2009; Landry & Beaulieu, 2010; Landry et al., 2004; Landry & Philippe, 2004; Persona et al., 2008). However, the above authors reached their conclusions by different means to those proposed in this paper. To the best of our knowledge, this is the first study that links nursing opinion with these advantages of the kanban system.
Moreover, we believe that the results would not have been as successful if the implementation of kanban had not been preceded by a series of changes throughout the hospital logistics system. These changes include the creation of a logistics platform, the implementation of a new warehouse management system, and the use of new radiofrequency terminals connected with the main computer system (Aguilar-Escobar & Garrido-Vega, 2013). In fact, as recognized in manufacturing implementations of the kanban system (Domínguez Machuca, García González, Domínguez Machuca, Ruiz Jiménez, & Álvarez Gil, 2003; Womack, Jones, & Ross, 1990), hospital implementation also requires changes in the logistics system that enable an adequate response to issues such as the maintenance of high levels of service quality, elimination of errors in the process, reduction of time, and assurance of reliable deliveries. Such a structured environment is essential in operating a kanban system and can even be considered an extension of the system (Sugimori et al., 1977). In fact, the kanban system entails sending supplies from the central warehouse more often and in smaller amounts (Persona et al., 2008). In the studied case, the kanban system triggers replenishment from the store twice per week while the units in the traditional system were mainly replenished only weekly. This new system represented more than 1500 daily replenishment lines in October 2011. The subsequent increase of workload in the central warehouse resulted in certain difficulties in maintaining service levels (Aguilar-Escobar & Garrido-Vega, 2013). However, the survey results showed that these initial difficulties had been overcome at the time of our survey (in 2013) which is reflected in the results of the satisfaction evaluation of nurses with the kanban system and the entire logistics system.
In conclusion, we found that the kanban system has promoted a series of reforms in the logistics system, and the logistics system has contributed towards the success of the kanban system.
5Practical implicationsThe high levels of satisfaction and the benefits derived from using kanban systems, as outlined in this paper, could encourage health administrators and managers towards their implementation. Additionally, since nursing satisfaction has been linked with higher performance (Leggat, Bartram, Casimir, & Stanton, 2010), health administrators and managers should consider that these results empirically demonstrate nursing satisfaction towards kanban system implementation. Indeed, as kanban systems provide benefits and satisfaction to nursing personnel, implementation risks could potentially be reduced. Furthermore, managers should consider differences in the level of satisfaction between user groups since this level could indicate the need to adapt approaches to better fit their requirements: e.g. the impact of a kanban implementation in a surgical or intensive unit could differ from that in a clinical unit.
We highlight the importance of carrying out a training programme as this significantly increased the valuation of all aspects considered in this study.
Another important implication was that those nurses who perceived their work units as being more patient-centred were significantly more satisfied with their jobs since they had a direct effect on patient care (Rathert & May, 2007). Accordingly, kanban systems contributed towards making nurses more patient-centred by leaving non-care activities to logistics personnel, thereby ensuring they had the material necessary for proper care. Indeed, our work demonstrated that nursing personnel needed less time for logistic activities with a kanban system than with a conventional system. Thus, implementing patient-centred practices, such as kanban systems, could result in improved nurse satisfaction followed by improved patient care, and organizational outcomes. Moreover, in the medium term, this time-saving can reduce personnel costs, thereby offsetting the investment of € 5178 per store.
6Research limitations and suggestions for future researchThis paper has outlined various limits. First, one of the authors acted as an economic-administrative director, responsible for hospital logistics, in this hospital group for much of the period considered (August 2006–September 2010), and a second author acted as head of purchasing and logistics department, which may have introduced a bias into the analysis. However, to partly compensate for this bias, a third investigator was involved in the case study and a rigorous research methodology was applied.
The second limitation is linked to the fact that our research methodology collected data using a single case study. Indeed, we measured employee satisfaction towards kanban systems in a single hospital group (AHVM), which makes us question the transferability of the results to other hospitals employing a kanban system. However, our results are valid, from an analytical point of view, since they present an example that reinforces and develops the existing theory concerning the advantages of using kanban systems in healthcare.
Similar studies on kanban systems in hospitals, including cross-case-type studies, should be conducted to further validate our findings. Additionally, the two factors found in the principal component analysis (advantages of a kanban system and logistics system performance), and the variables represented within each, should be investigated and confirmed through further research into healthcare settings.
Although double-bin is not the only possible way to implement kanban in hospital logistics (Heinbuch, 1995; Persona et al., 2008; Patterson, 2012) it is the most widely used application of kanban. Therefore, in this article we use the terms double-bin, two-bin, and kanban system interchangeably.

