


Lithuania is repeatedly rated among road safety outsiders having some of the worst statistical indicators. Traffic collisions are the leading cause of injuries and mortality of youth (5–25 years old) in Lithuania, age group 15–24 contributing the most. Based on literature review we concluded that theoretically rationalized educational road safety intervention could raise Lithuanian road safety standards in the future. Theory of Planned Behaviour (TPB) was employed to design and assess the effectiveness of pre-driver road safety education programme on changing behaviour components predicting risk taking behaviour of late teenage students. 11 graduate students (N=302) from 10 schools took part in a Quasi-experimental study, 6 schools were assigned to experimental group, 4 to control. Experimental group have received an educational 4h intervention, after a baseline questionnaire assignment. 5 components of road risk taking behaviour, based on Health Belief Model and Theory of Planned Behaviour constructs were measured in 2 week's time interval as indicators of effectiveness of the programme. Students from the experimental group had more negative attitude towards road risk taking behaviour, they were less willing to engage in such behaviour and they perceived their peers as less tolerant to this behaviour after the intervention. No significant changes in these components, but negative change in perceived threat, have occurred in the control group. Results showed that the programme was effective in changing behaviour components that predict students’ risk taking on the road.
Lituania ha sido clasificada reiteradamente por los extranjeros como poseedora de algunos de los peores indicadores estadísticos en seguridad vial. Ahí, las colisiones de tráfico son causa principal de lesiones y mortalidad en jóvenes (5-25 años), especialmente en el rango de edad de entre los 15 a 24 años. La revisión de la literatura indica que los estándares Lituanos en seguridad vial podrían incrementarse con intervenciones educativas teóricamente racionalizadas. La teoría de la conducta planificada (TCP) se empleó para diseñar y evaluar la eficacia de un programa de educación en seguridad vial para preconductores, en el cambio de componentes conductuales que predicen conductas de toma de riesgos al volante (CTRV) en estudiantes adolescentes. Participaron en un estudio cuasi-experimental estudiantes del grado 11 (N=302) pertenecientes a 10 escuelas, 6 de ellas asignadas al grupo experimental y 4 al grupo control. El grupo experimental recibió una intervención educativa de 4h, después de la aplicación del cuestionario de línea base. Como indicadores de efectividad del programa, 5 componentes de CTRV basados en constructos del modelo de creencias de salud y la TCP fueron medidos en un intervalo de 2 semanas. Los estudiantes del grupo experimental tuvieron actitudes más negativas hacia la CTRV, estaban menos dispuestos a participar en este tipo de comportamiento y percibieron a sus compañeros como menos tolerantes a este comportamiento después de la intervención. No hubo cambios significativos en los componentes, pero en el grupo control hubo un cambio negativo en percepción de amenaza. Los resultados mostraron que el programa logró cambiar componentes conductuales que predicen CTRV de los estudiantes.
Lithuania is repeatedly rated among road safety outsiders having road fatality rate of 85 people killed per million inhabitants, compared to 52 which is EU average, or 30 and 28 in United Kingdom and Sweden, in 2013 (European Commission, 2014). Traffic collisions are the leading cause of injuries and mortality of youth (5–25 years old) in Lithuania, age group 15–24 contributing the most (Gurevičius & Drūtytė, 2009; Laukaitienė, Ciesiūnienė, & Bagdanavičiūtė, 2007).
Over representative youth involvement in road traffic collisions is well documented all around the globe (Bates, Davey, Watson, King, & Armstrong, 2014; Scott-Parker, Watson, King, & Hyde, 2012b; World Health Organization, 2013), there is a body of evidence rationalizing it (World Health Organization, 2007), which led to the development of effective countermeasures and reduction of youth road injuries and mortality in some Western countries (Chen et al., 2010; European Association for Injury Prevention and Safety Promotion (EuroSafe), 2013; Hosking, Ameratunga, Exeter, Stewart, & Bell, 2013; Sleet, Ballesteros, & Nagesh, 2010). Despite all this, Lithuania has failed to achieve significant improvements (Lunevicius, Herbert, & Hyder, 2010). It is suggested that Lithuania's low traffic safety standards appear to be structural deficiencies in responsibility sharing, cooperation between different governmental bodies and lack of awareness among decision makers (Government of Republic of Lithuania, 2014). All this result in poor road network condition and slow implementation of modern prevention measures (World Health Organization, 2009).
Often contemporary traffic safety strategies incorporate educational interventions (The World Bank Global Road Safety Facility, 2009). Nevertheless, effectiveness of these interventions is still debated. There are opposing opinions from different researchers stating that educational interventions have no effect on the risk of traffic collision involvement and that they can increase this risk by increasing exposure i.e. encourage adolescents to obtain driving license earlier. Others suggest that these measures can account to approximately 9% in collision involvement rates reduction (Lonero & Mayhew, 2010; Phillipsa, Ullebergb, & Vaa, 2010).
It should be acknowledged that there is no single definition and classification of educational road safety interventions, they are of different duration, employ variety of didactic measures as well as are targeted to different population groups and cover range of topics (Buckley, Sheehan, Shochet, & Chapman, 2013). Naturally all of these determinants can influence intervention's effectiveness and cause contradictions in research findings presented hereby.
Selection of appropriate outcome measure matters as well. Scholars supporting educational interventions, suggest that the number of traffic collisions is not always appropriate outcome measure at first, since educational interventions primarily aim to influence persons behaviour (Tronsmoen, 2010). Collision involvement is related to other factors rather than purely on ones’ behaviour; factors that are attributable to the level of exposure and environment i.e. annual mileage, road, weather, automobile conditions etc. The more appropriate outcome measure in this case is to assess ones behaviour or, as that is not always possible, other properties that predict it (Poulter & McKenna, 2010).
Behaviour researchers have proposed a range of theories aiming to predict and explain person's behaviour. According to Cognitive Dissonance theory, change in believes that drive certain behaviour can lead to change in the actual behaviour (Festinger, 1957). This assumption has been incorporated in Social Cognition models such as Theory of Planed Behaviour (TPB) and Health Beliefs Model (Ajzen, 1985; Rosenstock, 1974). TPB is widely accepted behaviour model which according to review of 185 studies is accountable to 39% of variance in intentions and 27% variance in behaviour (Armitage & Conner, 2001).
According to the TPB, intentions and behaviour are a function of one's attitudes (behavioural beliefs), subjective norms (normative beliefs) and perceived behaviour control (control beliefs). Attitudes refer to general beliefs about intended behaviour and its outcomes; subjective norm is a set of beliefs about social pressure related to engagement into behaviour under consideration; perceived behaviour control refers to beliefs about one's ability to successfully execute behaviour under consideration (Ajzen, 2014). According to TPB, changes in some of these beliefs can produce change in behaviour. These claims lay theoretical backgrounds for design and evaluation of health education programmes, and have been employed in a number of them, in and outside the field of road safety (Hackman, & Knowlden, 2014; Mann, 2010; Poulter & McKenna, 2010; Webb, Joseph, Yardley, & Michie, 2010).
According to presented considerations, beliefs favourable to dangerous behaviour are predicting execution of it, on the contrary, beliefs favourable to safe behaviour can be compared to salutogenic factor that predicts avoidance of unsafe behaviour. Transition of one's beliefs from one end of the scale towards another is usually difficult and sometimes even impossible, hence educational health promotion programmes are most effective when delivered before undesirable beliefs are embedded (Chapman, Buckley, & Sheehan, 2012). This makes timing a vitally important property in educational youth road safety programmes. As adolescent mature and acquire more independence and experience, their beliefs about behaviour on the road start to formulate and can be impossible to change latter (Buckley et al., 2013; Mann, 2010; Waylen & McKenna, 2008). Based on this, educational road safety programme can be expected to be most beneficial if delivered at the time when adolescent starts to consider certain behaviour on the road.
Based on observations presented hereby we conclude that theoretically rationalized educational road safety intervention could raise Lithuanian road safety standards in the future. We aimed to develop best practices based programme and assess its effectiveness in the sample of late teenagers. We predicted that programme activities will have a positive effect on the components of risk taking behaviour and, as it is suggested by the theory of TPB, behaviour of our target population.
Material and MethodsProgrammeThe goal, we were aiming to achieve, was to induce change in behaviour components described in the TPB of high school students aged 16–18 years old, who participate in road traffic as passengers and future drivers. Programme which was used to achieve these goals was based on the TPB and addressed students beliefs about most common risk factors i.e. speeding, impaired driving, wear of safety belts, use of mobile devices as well as peer influence towards occurrence of these risk factors (Bates et al., 2014; Scott-Parker, Watson, King, & Hyde, 2012a; Scott-Parker et al., 2012b; Šeibokaitė, Endriulaitienė, & Markšaitytė, 2011). Didactic methods (interactive games, case analysis, role play, etc.) that we used in the programme have come from publicly available publications that identified them as the most appropriate tools to achieve our goals (Buckley, 2008; Buckley, & Watson, 2013; Mayhew, Simpson, Williams, & Ferguson, 1998). An example of hypothetical situation and rationale based on TPB of how the programme was trying to prevent intended behaviour: “A teenage driver believes that after having a low to moderate amount of alcohol she is still able to safely drive her friends back home, without being pulled over by police or getting in to a road collision (unrealistic control beliefs). She heard about her friends doing this previously and is pressured by her friends in that particular situation (perceived social norm). She thinks that by doing this she will be able to get back home on time and avoid unnecessary conflict with her parents as well as to avoid being bullied by her friends (positive attitude)”.
Based on TPB we aimed to diminish one's perceived ability of driving under the influence of alcohol by explaining about likely outcomes of such behaviour and chances of their occurrence (addressed behavioural beliefs). Secondly we aimed to improve her perceived ability to resist peer pressure by providing necessary communication techniques (addressed control beliefs). Thirdly, the actual social norm was presented by allowing peer group discussion led by trained facilitator (addressed normative beliefs).
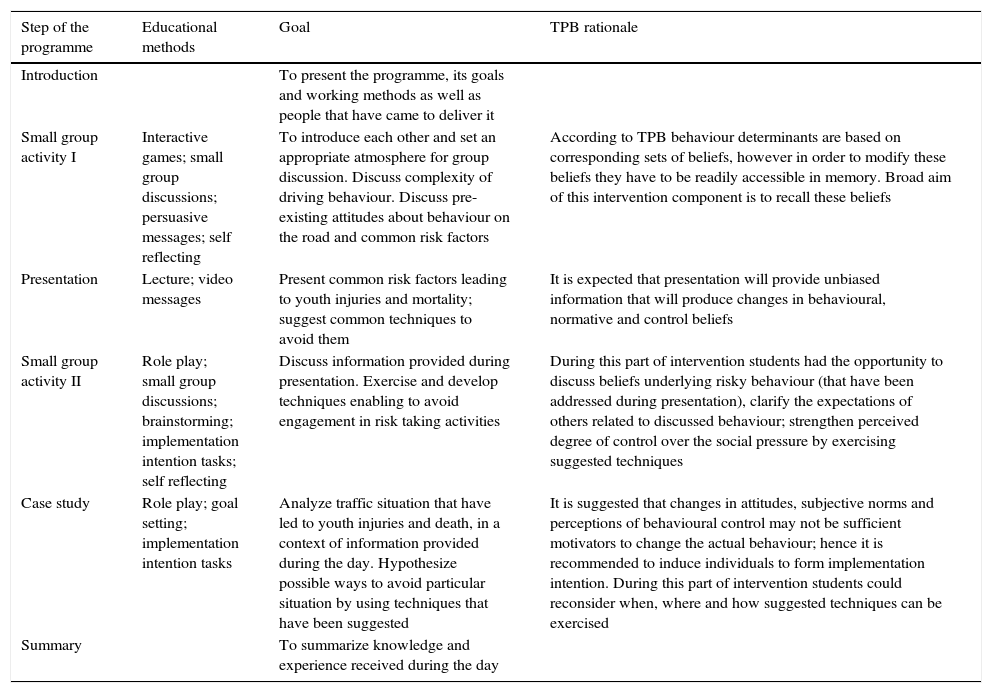
Detailed structure the programme is provided in Table 1.
Programme structure.
| Step of the programme | Educational methods | Goal | TPB rationale |
|---|---|---|---|
| Introduction | To present the programme, its goals and working methods as well as people that have came to deliver it | ||
| Small group activity I | Interactive games; small group discussions; persuasive messages; self reflecting | To introduce each other and set an appropriate atmosphere for group discussion. Discuss complexity of driving behaviour. Discuss pre-existing attitudes about behaviour on the road and common risk factors | According to TPB behaviour determinants are based on corresponding sets of beliefs, however in order to modify these beliefs they have to be readily accessible in memory. Broad aim of this intervention component is to recall these beliefs |
| Presentation | Lecture; video messages | Present common risk factors leading to youth injuries and mortality; suggest common techniques to avoid them | It is expected that presentation will provide unbiased information that will produce changes in behavioural, normative and control beliefs |
| Small group activity II | Role play; small group discussions; brainstorming; implementation intention tasks; self reflecting | Discuss information provided during presentation. Exercise and develop techniques enabling to avoid engagement in risk taking activities | During this part of intervention students had the opportunity to discuss beliefs underlying risky behaviour (that have been addressed during presentation), clarify the expectations of others related to discussed behaviour; strengthen perceived degree of control over the social pressure by exercising suggested techniques |
| Case study | Role play; goal setting; implementation intention tasks | Analyze traffic situation that have led to youth injuries and death, in a context of information provided during the day. Hypothesize possible ways to avoid particular situation by using techniques that have been suggested | It is suggested that changes in attitudes, subjective norms and perceptions of behavioural control may not be sufficient motivators to change the actual behaviour; hence it is recommended to induce individuals to form implementation intention. During this part of intervention students could reconsider when, where and how suggested techniques can be exercised |
| Summary | To summarize knowledge and experience received during the day |
Active student participation was encouraged by attractive activities and reflective discussions in peer groups, led by facilitators – undergraduate psychology students. Activities in peer groups were standardized and explicitly described in the manuals, peer group facilitators had to pass a training programme before they could take part in the scheduled activities. Overall programme duration was 4h. Programme consisted of a lecture, two small group sessions; and a case study. Programme did not include driving lessons nor did it teach any theoretical car control skills i.e. it excluded methods and topics that are traditionally identified as possibly encouraging to obtain driving license (Chapman et al., 2012).
Programme was implemented in partnership of a local NGO having a public health background and primarily specializing in youth health promotion activities and Psychology scholars interested in traffic psychology. All the practical activities i.e. peer group facilitator training and their support during the workshops, lectures, case studies, managerial tasks were conducted by a representative of this NGO, whilst methodological support was provided by the traffic psychology researchers.
Study design and subjectsIn order to assess effectiveness of the programme quasi-experimental study was conducted. It was organized in Kaunas region (the second largest region in Lithuania) secondary schools. All secondary schools having 11 grade students from Kaunas region were invited to take part in this programme. Those who were interested were assigned to experimental group (6 schools) and interventions were carried out at each school of this group. Other 4 schools were recruited from the same region asking schools ‘administrations to conduct the survey. Participants from both groups completed the questionnaire twice at the same time interval: before implementation of the intervention (T1 measurement) and after a gap of two weeks (T2 measurement).
In total 192 participants from experimental group participated in the T1 measurement, 85 male and 107 female participants. Similarly 110 participants from the control group completed the questionnaire (47 males, 63 females). The age of all participants ranged from 16 till 19 years (the mean age was 16.82 years (SD=0.522). No age differences were found between experimental and control groups (t=−1.464, df=299, p>0.144).
135 students from the experimental group (55 males and 80 females) and 51 students from control group (18 males and 33 females) participated in the T2 measurement. Total enrolment in the study was 70.3 percent in experimental group and 46.4 percent in control group.
Measures5 components of road risk taking behaviour based on Health belief model and Theory of Planned Behaviour constructs were measured in this study. These components were in line with the rationale and content of an educational programme. Components included attitudes, perceived threat, subjective norm, perceived behavioural control and intentions; and were targeted to 6 aspects of road risk taking behaviour that were addressed in a programme. These aspects were: speeding, driving under the influence of alcohol or illegal drugs, driving while talking on the mobile phone, risk taking due to peer influence and driving without safety belt. The scales for the measurement were developed by the authors for the purposes of this study based on the recommendations of the above mentioned theories (CAST (Campaigns and Awareness-raising strategies in traffic safety); Belgian Road Safety Institute, 2009; Fishbein & Ajzen, 2010).
Attitudes towards road risk taking behaviour were measured by 23 item 7-point Likert scale (1-completely disagree; 7-completely agree). Each item was targeted towards one of the 6 before mentioned aspects of the road risk taking behaviour. E.g., “I’m not sure that safety belt can protect me from injuries during an accident”. Higher scores of the attitude scale show stronger acceptance of road risk taking behaviour. Internal consistency of this scale was satisfactory both in the T1 and T2 measurements (Cronbach α – 0.81 and 0.85).
Perceived threat of road risk taking behaviour was also measured by 6 item 7-point Likert scale (1-very unlikely; 7-very likely). Each item was related to each aspect of the road risk taking behaviour addressed in a programme. Sample item: “How likely is it that you will get into car accident which would result in severe consequences if you were driving 10km/h faster than it is allowed?”. Higher scores of the perceived threat scale show higher perceived threat of the road risk taking behaviour. Internal consistency of this scale was satisfactory both in the T1 and T2 measurements (Cronbach α – 0.87 and 0.91).
Perceived norm of the road risk taking behaviour was measured by 6 item 7-point Likert scale (1-completely disagree; 7-completely agree). Each item was targeted towards one of the 6 aspects of the road risk taking behaviour, asking participants to evaluate perceived agreement of their peers in various situations. Sample item: “If I was driving after I had 3 drinks, most of my friends would disagree”. Higher scores of this scale show more negative perceived norm of the road risk taking behaviour. Internal consistency of this scale was satisfactory both in the T1 and T2 measurements (Cronbach α – 0.81 and 0.85).
Perceived behavioural control of road risk taking was measured by 6 item 7-point Likert scale (1-very easy; 7-very difficult). Each item was also targeted towards one of the 6 areas of the road risk taking behaviour, by asking participants to evaluate how difficult it would be for them to restrain from this behaviour. Sample item: “How difficult or easy it would be for you not to speed if you were a car driver”. Higher scores of this scale show lower behavioural control. Internal consistency of this scale was satisfactory both in the T1 and T2 measurements (Cronbach α – 0.80 and 0.86).
Intentions to take risks on the road were measured by 7 item 7-point Likert scale (1-very unlikely; 7-very likely). Each item was targeted towards one of the 6 aspects of the road risk taking behaviour, measuring likelihood of engaging to risky activities on the road. Sample item: “How likely is it that you will drive a car after smoking marihuana?”. Additional question was used to measure intention not to use safety belt as a car passenger. Higher scores of this scale show stronger intentions to take risks. Internal consistency of this scale was satisfactory both in the T1 and T2 measurements (Cronbach α – 0.67 and 0.69).
Statistical methodsThe distribution of variables was assessed by the Kolmogorov–Smirnov test for homogeneity of variance. It was found that all scales were not normally distributed, in particular perceived behavioural control and perceived threat scales. Asymmetry coefficients of data from intentions, attitudes and perceived norms scales did not exceed 1, hence criterions assuming normal distribution were used in analysis only in these particular cases. Non parametric two independent samples Mann–Whitney U test was used for between-group comparisons at T1 and T2 measurements. Within-group changes were analyzed using non parametric related samples Wilcoxon test. Linear regression analysis was used to determine if being in experimental or control group predicts changes in perceived norm as this variable differed initially between these groups. Effect sizes of changes in components of road risk taking behaviour were measured by calculating the values of Cohen's d using the means and standard deviations of two groups (experimental and control). Cohen's d=M1−M2/spooled, where spooled=[(s12+s22)/2]. Differences were considered statistically significant at p<0.05. All statistical analyses were executed using SPSS for Windows, version 15.0 (SPSS Inc., Chicago, IL).
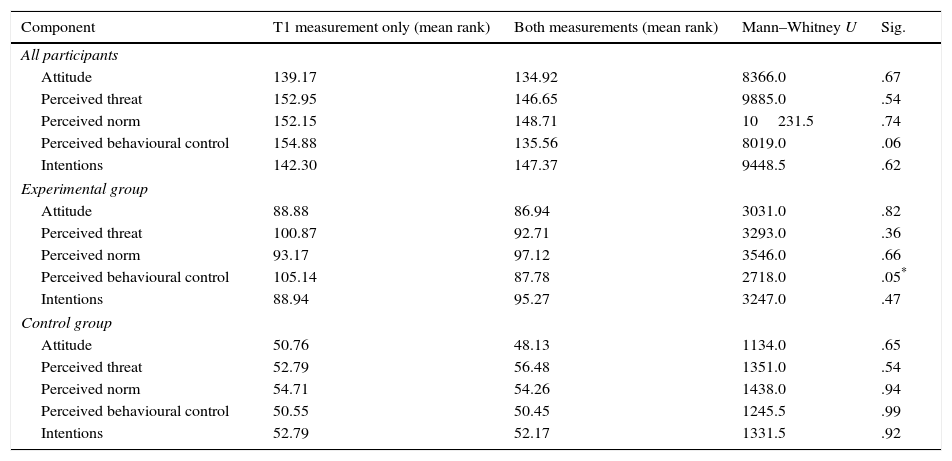
ResultsThe participants’ attrition rate analysisFirstly it was important to assess if study participants, that took place in T1 and T2 measurements, were homogenous to participants that took place in only T1 measurement. Mann–Whitney U test for two independent groups was used for comparison of 5 components of road risk taking behaviour (attitudes, perceived threat, perceived norm, perceived behavioural control and intentions) of two groups of participants in all participants group as well as separately in the experimental and control groups (Table 2).
Comparison of road risk taking behaviour components between students who participated only in T1 measurement and in both measurements.
| Component | T1 measurement only (mean rank) | Both measurements (mean rank) | Mann–Whitney U | Sig. |
|---|---|---|---|---|
| All participants | ||||
| Attitude | 139.17 | 134.92 | 8366.0 | .67 |
| Perceived threat | 152.95 | 146.65 | 9885.0 | .54 |
| Perceived norm | 152.15 | 148.71 | 10231.5 | .74 |
| Perceived behavioural control | 154.88 | 135.56 | 8019.0 | .06 |
| Intentions | 142.30 | 147.37 | 9448.5 | .62 |
| Experimental group | ||||
| Attitude | 88.88 | 86.94 | 3031.0 | .82 |
| Perceived threat | 100.87 | 92.71 | 3293.0 | .36 |
| Perceived norm | 93.17 | 97.12 | 3546.0 | .66 |
| Perceived behavioural control | 105.14 | 87.78 | 2718.0 | .05* |
| Intentions | 88.94 | 95.27 | 3247.0 | .47 |
| Control group | ||||
| Attitude | 50.76 | 48.13 | 1134.0 | .65 |
| Perceived threat | 52.79 | 56.48 | 1351.0 | .54 |
| Perceived norm | 54.71 | 54.26 | 1438.0 | .94 |
| Perceived behavioural control | 50.55 | 50.45 | 1245.5 | .99 |
| Intentions | 52.79 | 52.17 | 1331.5 | .92 |
It was found that two groups of participants did not differ in any measured component of the risk taking behaviour, but some differences were found in separate analysis of experimental and control groups. Students from the experimental group who participated only in the T1 measurement had weaker perceived behavioural control of road risk taking than those who participated in both measurements. No other differences were found.
Baseline comparison of the experimental and control groupsSecondly Mann–Whitney U test was used to assess if experimental and control groups were homogenous during the baseline survey, in all 5 road risk taking behaviour components (Table 3).
Baseline comparison of the experimental and control groups.
| Component | Experimental group (mean rank) | Control group (mean rank) | Mann–Whitney U | Sig. |
|---|---|---|---|---|
| Attitude | 136.25 | 136.94 | 8483.0 | .95 |
| Perceived threat | 144.63 | 156.64 | 9380.5 | .25 |
| Perceived norm | 141.07 | 165.80 | 8607.0 | .02* |
| Perceived behavioural control | 136.47 | 153.59 | 8091.0 | .09 |
| Intentions | 144.72 | 146.89 | 9527.0 | .83 |
The analysis has shown that initially no differences between experimental and control groups were present in their attitudes, perceived threat, intentions and perceived behavioural control. Nevertheless subjects from control group had more negative perceived norm of road risk taking behaviour comparing to the experimental group, i.e. students in the control group thought their peers would be less tolerant to their risk taking behaviour. Based on these findings evaluation of changes of perceived norm in two research groups were made using statistical techniques that allowed us to control these initial differences.
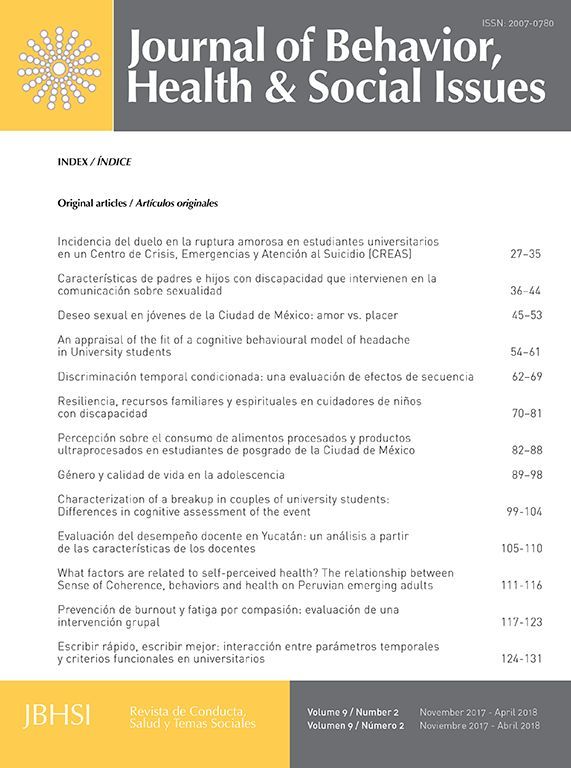
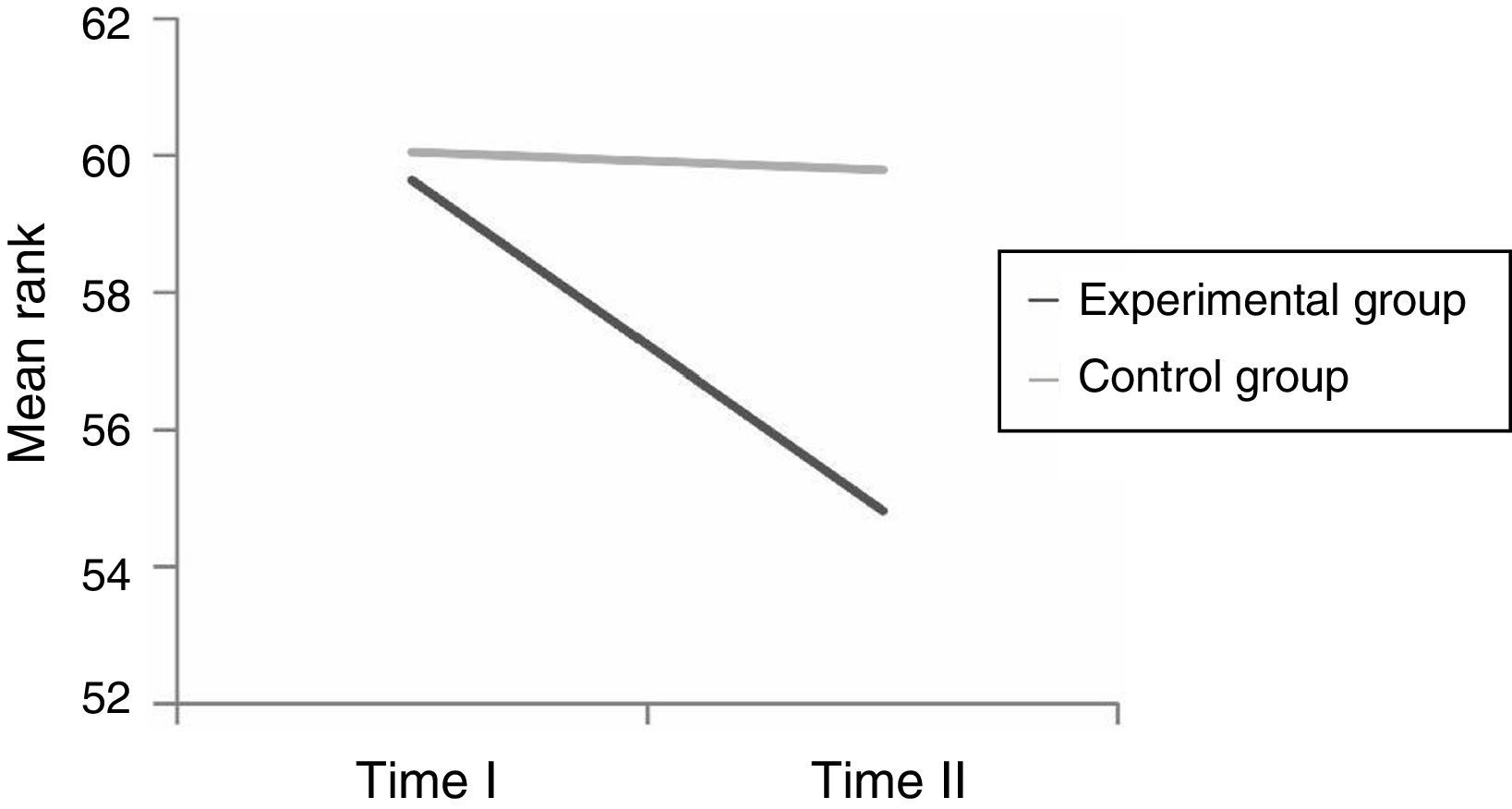
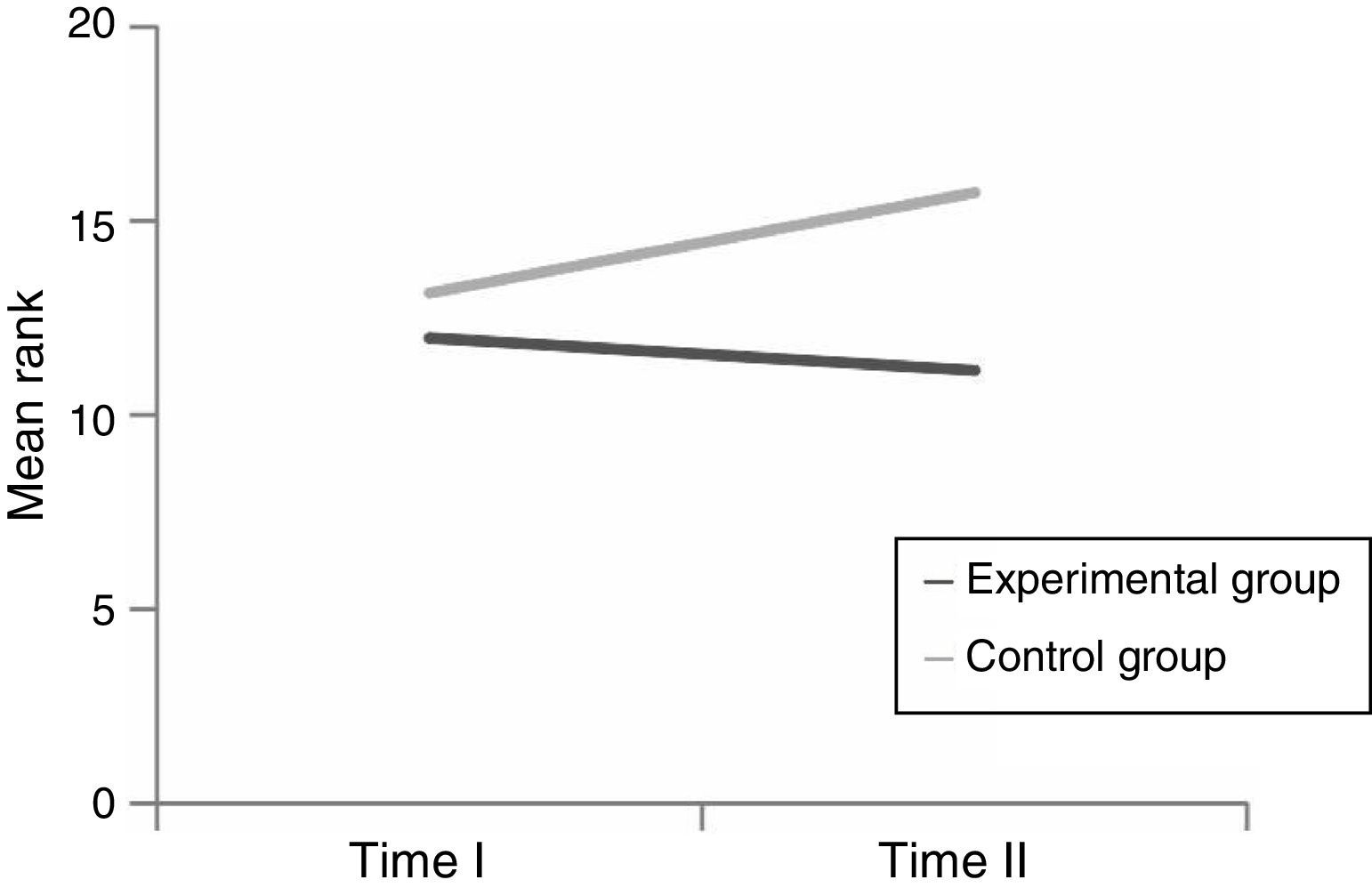
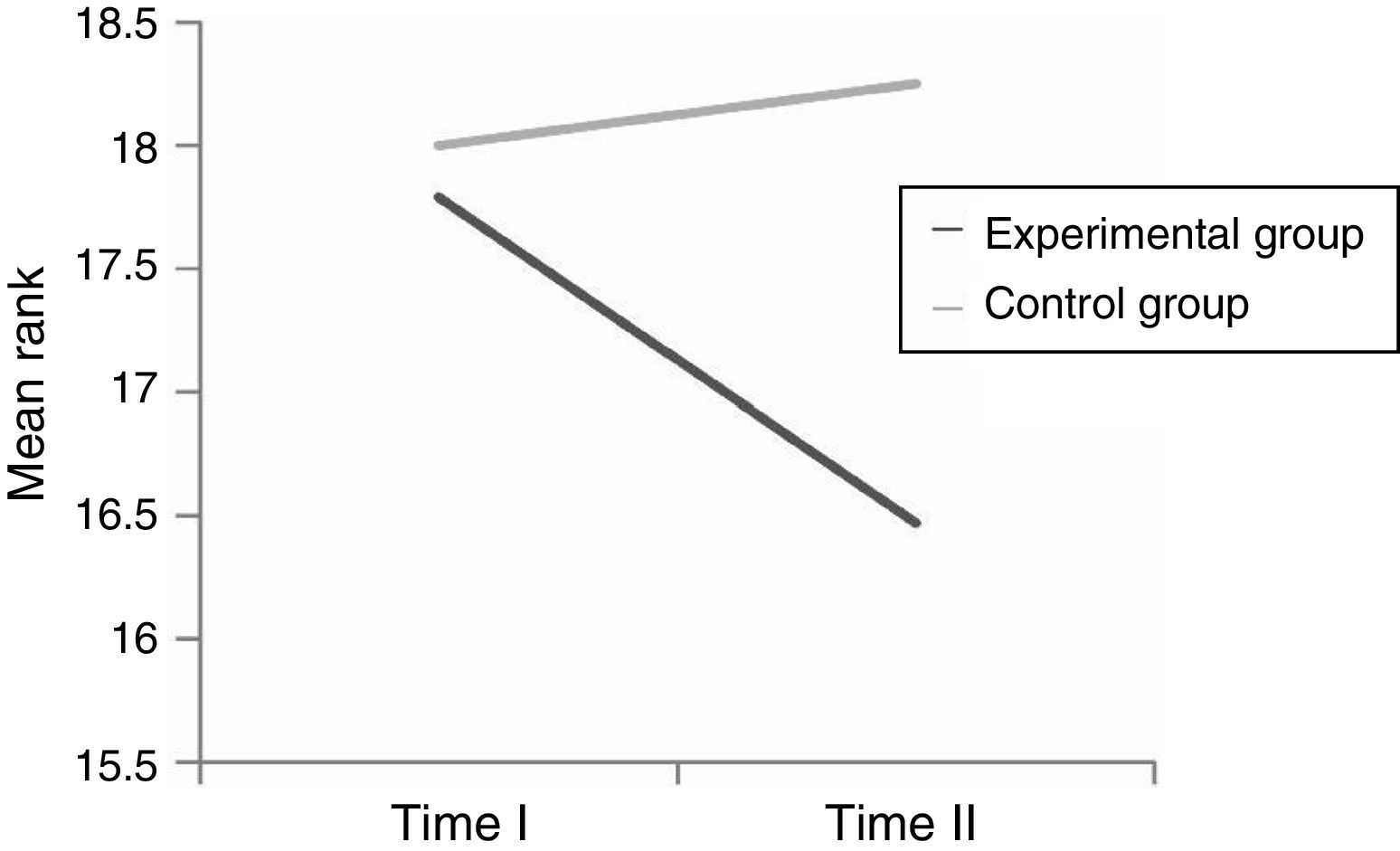
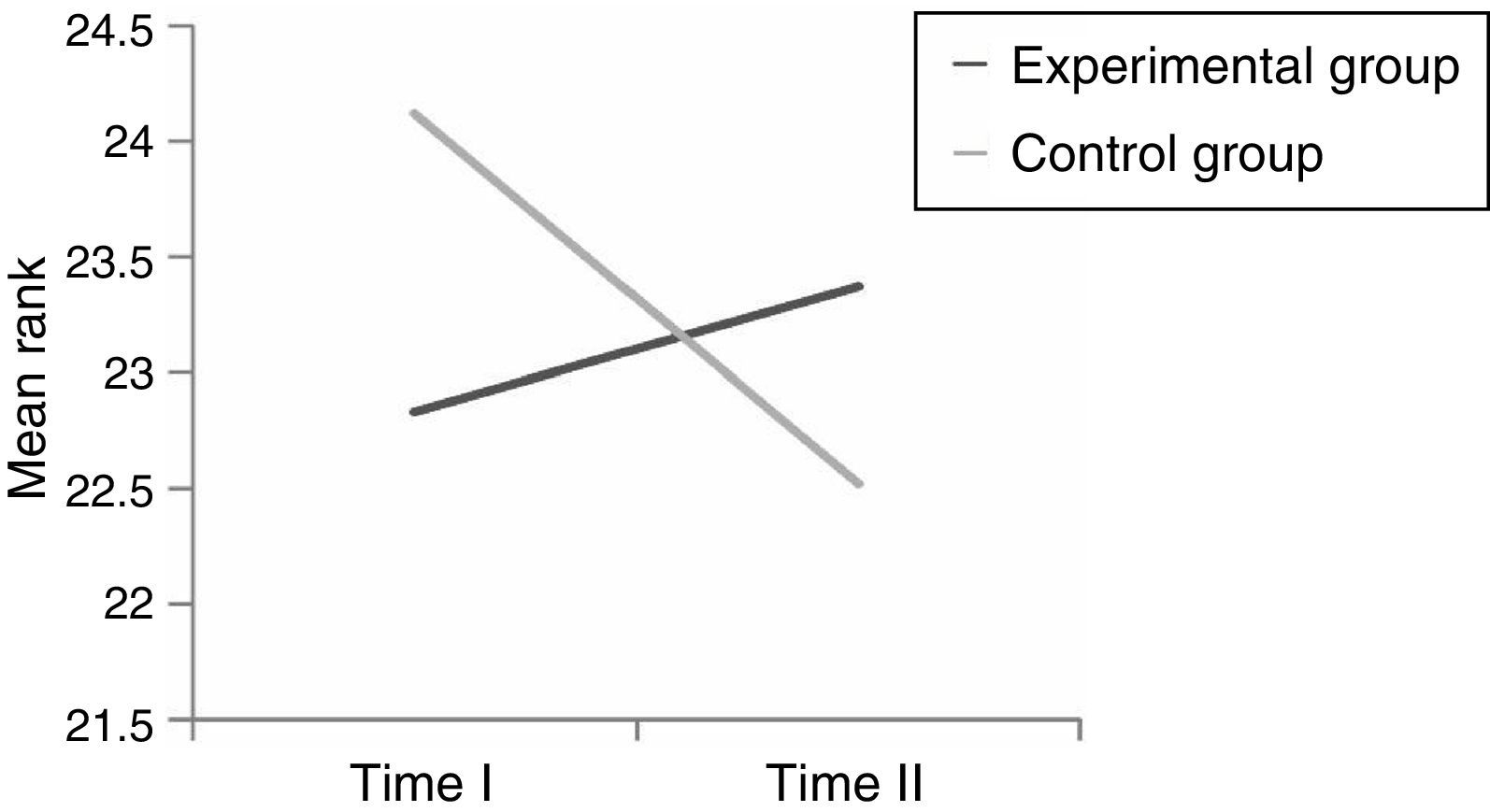
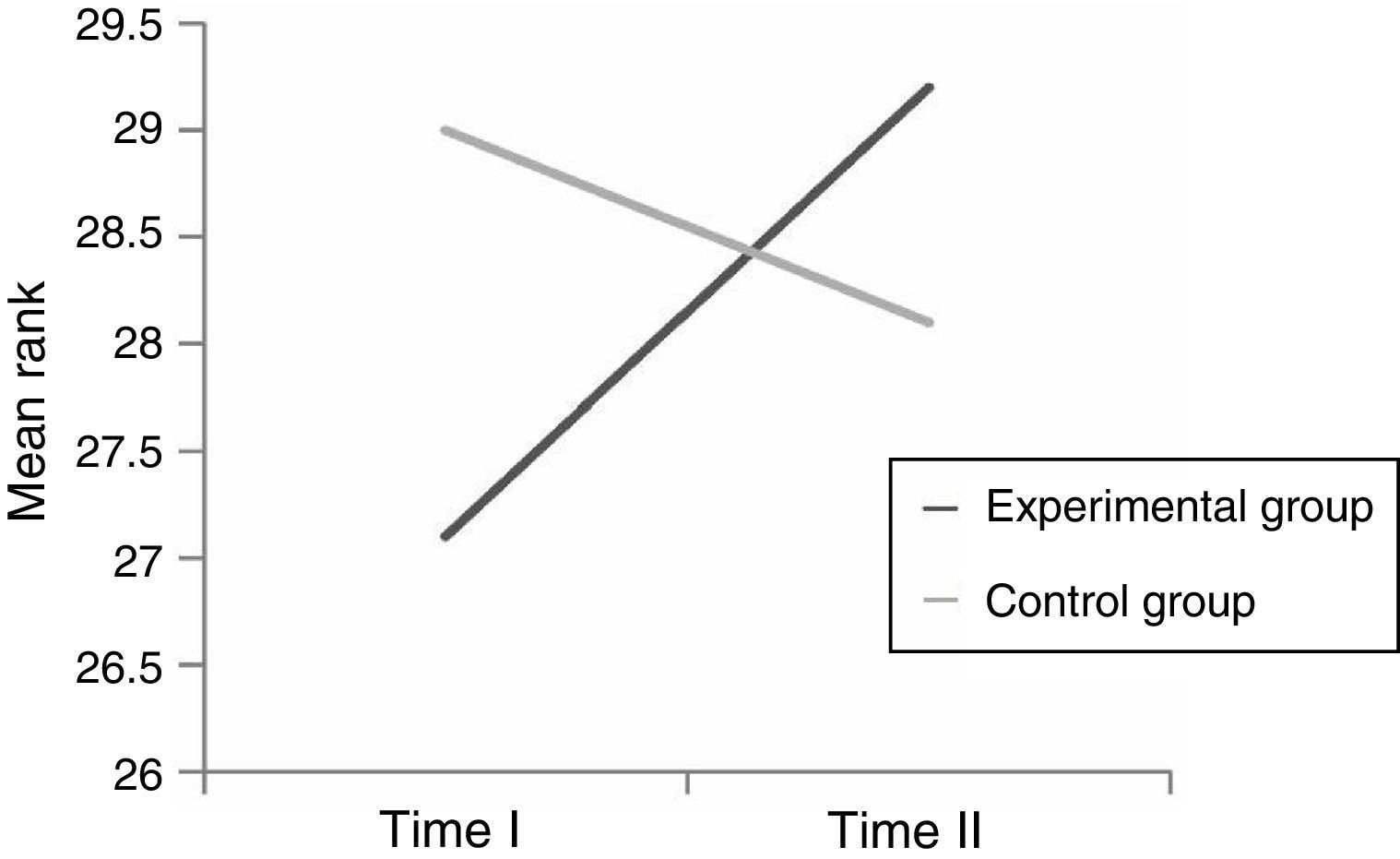
Changes in the components of the road risk taking behaviour in the experimental and control groupsThirdly differences between T1 and T2 measurements’ results were measured by using nonparametric Wilcoxon criteria in all 5 components of the risk taking behaviour, separately in experimental and control groups. It was expected that positive changes of road risk taking behaviour components will be observed in experimental group, while no changes or negative changes of these components were expected in the control group. Changes of all 5 components of road risk taking behaviour are shown in Figs. 1–5.





Statistically significant positive changes in attitudes towards risk taking behaviour, intentions and perceived norm occurred in the experimental group. It means that students from the experimental group had more negative attitude towards road risk taking behaviour, they were less willing to engage in risk taking behaviour and they perceived their peers as less tolerant to their risk taking behaviour after the programme. No significant changes in these components have happened in the control group. Moreover negative change in perceived threat occurred in the control group in the T2 measurement compared to the T1 measurement. Students from control group perceived road risk taking behaviour as less threatening in two weeks after the T1 measurement.
Based on the finding that during the T1 measurement control group had more negative perceived norm of the road risk taking behaviour comparing to experimental group, linear regression analysis was used to assess effect of a programme to the transition of this behaviour construct. Perceived norm from T2 measurement was chosen as dependant variable, while perceived norm from T1 measurement as though as group (1-experimental; 2-control) variables were chosen as explanatory variables. The model was suitable for analysis (F=15.464, p<0.000; R2=0.138).
Analysis showed that even though perceived norm at T1 measurement was significantly predicting dependent variable (β=0.381; p<0.001), but group variable was not a significant predictor (β=−0.099; p<0.158) of perceived norm at T2 measurement. It means that we could not say that prevention programme was effective in changing perceived norm of the road risk taking behaviour of the students.
Prevention programmes effectiveness studies commonly seek not only to measure changes in the attitudes and/or behaviour of the participants, but also its effect size. Following this tradition we measured effect sizes by Cohen d estimates for the components of road risk taking behaviour, which changed significantly between the experimental and control groups. It was found that prevention programme was mostly effective changing the attitudes (Cohen d=0.467; medium effect) and weakly but significantly changed students’ intentions (Cohen d=0.256; small effect) and perceived threat (Cohen d=0.385; small effect) of road risk taking behaviour.
DiscussionThe purpose of our study was to evaluate the effectiveness of the pre-driver education programme based on the Theory of Planned Behaviour (TPB). This programme was designed for high school students and implemented in Lithuania for the first time. It focused on influencing attitudes, perceived threat, perceived norm, perceived behavioural control and intentions related to road risk taking behaviour.
In general the results showed that the programme was effective in changing the components related to road risk taking behaviour. This is in line with previous findings (Rosenstock, 1974) and confirms that despite the critique the TPB is useful for behaviour change interventions for older adolescents with different cultural backgrounds. After the programme implementation students from the experimental group developed more negative attitudes and lower intentions of road risk taking. Meanwhile students from the control group retained these elements stable in a period of two weeks. Moreover their perceived threat of road risk taking decreased showing that even short period of time in adolescence could be critical for the development of risky perceptions as possible antecedents of risky behaviour. On the other hand, this result should be taken with caution as the changes of the perception of threat towards more risky direction might have been influenced by measurement procedure. Some authors state that attitudes and beliefs might be changed just asking respondents to think about them while answering the questionnaires (Maio & Haddock, 2010).
Contrary to expectations no significant changes occurred in perceived behavioural control and perceived norm of risky behaviour on the road after the programme implementation. This result might be explained by the construct of self-efficacy (Ajzen, 2002). It is possible that self-efficacy is more related to stable personality features (Bandura, 2012) therefore more extended in time programme might be needed for significant changes to occur. On the other hand, most activities of this programme were targeted at cognitive and emotional aspects of risky intentions for participants who do not have experience in driving, therefore their self-efficacy related to driving might not be relevant. Similarly perceived norm of road risky behaviour for adolescents might be resistant to rapid change due to extreme importance of peer opinion (Scott-Parker et al., 2012a). If significant peers did not participate in the intervention activities, adolescents’ perceived norm of risky behaviour did not change. When improving the programme, more attention should be paid to strengthen the ability to control own behaviour on the road in the situations relevant to non-drivers adolescents, e.g. wearing a seat belt, refusing to go with a driver under the influence of alcohol or drugs. Despite the efforts in the current programme, specific techniques of resisting to peer influence should be practised extensively.
We could confirm that TPB based pre-driver education programme is useful tool for practical application in Lithuanian context. Still some limitations of the study should be taken into account in order to have stronger rationale for programme effectiveness. First of all, the sample size of the study participants was quite small; therefore the effect sizes were small to medium. Secondly, the investigation was based on self report data, thus social desirability bias might have influenced the results. Finally, only short-term effectiveness of the programme was confirmed; long-term effectiveness has to be evaluated in the future investigations. In addition, other researchers are encouraged to investigate the effectiveness of this programme in other countries. Studies of individual/personality correlates of programme effectiveness would be also of high value.
Peer review under the responsibility of Asociación Mexicana de Comportamiento y Salud.