

Non-suicidal self-injure behavior, depression and anxiety can be reduced by some variables as coping skills; for the treatment based on these skills is proposed the use of a software based on HyperText Markup Language, version 5 for different platforms as mobile systems and personal computers. The software is developed in the form of social interaction, in order to support the assimilation of these cognitive constructs in the adolescent population. Furthermore this program can be used as a teaching instrument for students of psychology which can facilitate understanding of skills and symptoms that the software takes into account. This article describes the development of coping skills enhancement software (SAHA Spanish acronym) based on traditional cognitive behavioral techniques for the reduction of negative thoughts and feelings, increased use of coping strategies focused on the problem, and reduction of thoughts related to Self-harm. The development takes into account review of cognitive behavioral therapy techniques, script, art design, programming, 3d modeling, edition, among other actions. As a result we obtained an application for the increase of coping skills that can be used in different operating systems.
Las habilidades de afrontamiento son una variable que puede limitar la conducta de autolesión no suicida, la depresión y la ansiedad; para el tratamiento basado en esas aptitudes, se propone el uso de un programa informático desarrollado en lenguaje HTML5 para acceder a múltiples plataformas como móviles y computadoras personales. El diseño usa un enfoque de interacción social para que apoye la asimilación de estos constructos cognitivos en la población adolescente, además de su uso como instrumento de enseñanza a estudiantes de Psicología, con el cual se comprenderán las habilidades y síntomas que toma en cuenta el programa informático. Este artículo describe la elaboración del software para el aumento de habilidades de afrontamiento (SAHA) basado en técnicas cognitivo-conductuales tradicionales para la disminución de pensamientos y sentimientos negativos, aumento en el uso de estrategias de afrontamiento centradas en el problema y disminución de pensamientos relacionados con la autolesión. El desarrollo toma en cuenta la revisión de técnicas de terapia cognitivo-conductual, guion, diseño de arte, programación, modelaje 3D y edición, entre otras acciones. Como resultado se obtuvo una aplicación para el aumento de habilidades de afrontamiento que puede ser usada en diferentes sistemas operativos.
The self-guided treatment supplied by computers have 40 years since its first apparition, among the oldest are the “chatterbots” designed by Kenneth Colby in the 60s, on that basis, Joseph Weizenbaum developed in 1966 “ELIZA” that mimicked a psychologist's questions instead of give advices; these software used natural language and capture patient's information via text (Cartreine, Ahern, & Locke, 2010).
Self-guided treatments, manage by computer, by definition, have its primary development with computer technology, those can be used depending on their characteristics in health institutions or home, also, if the software is developed with multi-language it can support people who otherwise would not have access to this intervention. This type of treatment, are designed to treat clinical problems or to help patients to change their behavior and improve their health; usually these programs are highly interactive and can use multiple techniques such as video, audio, text and animation and can be distributed over the internet or hardware like CDs, DVDs, etc. (Cartreine et al., 2010).
The cognitive behavior therapy (CBT) supported by software, varies according to its application and provides certain advantages such as: remote application, lower costs, communication through dynamics and support for people with phobias, limiting anxiety or physical disability, when these make difficult the traditional therapy (Cartreine et al., 2010).
Most of the contemporary self-guided software are CBT based and they are focused to depression treatment, however, treatments for aliment related problems, tobacco and drug abuse are also been developed (Cartreine et al., 2010).
During the development of life, a person experiences different events, based on these events the subject develops cognitive schemata about life, these constructs can be positive or negative for the individual; when they are negative, they can predispose or cause that an individual experiences easier feelings and negative experiences such as stress, anguish, anxiety, poor self-image, depression, among others (Shapiro, 2008), for example if John began to play soccer and fails to score and then played basketball and neither did it well, John could think that simply is not good for sports in general, developing a negative self-image of him about sports.
Some patients may have deficiencies in coping skills, this can lead to depressive thoughts and feelings; whereby one of the coping methods is the learning and use of skills to solve and address problems, which are intended to support the patient in everyday problems that cause distress, the patient is encouraged to seek solutions by being asked about how they have solved such problems in previous situations, or how they recommend to a friend to solve that problem. Then the therapist offers potential solutions, if necessary (Beck, 2011).
Next some software packages that are developed for depression treatment are reviewed, every one uses different approaches: The program Coping Cat Cat CD-ROM (Khanna & Kendall, 2008) is based on coping skills, and uses animations, audio and pictures; The software Treasure Island (Brezinka, 2012) develop CBT basic concepts specifically the triad: thought, behavior and feelings; The informatics program gNats (Coyle, McGlade, Doherty, & O’Reilly, 2011) use avatar based navigation in 3d environments to introduce mental health concepts, depressive thoughts identification, consequences and how to address them. Finally another approach for the use of software in behavioral therapy is the assessment via Stroop for different health problems like smoking (Calleja & Hernandez-Pozo, 2009).
MethodIn order to explain the software's development, it has been decided to expose it from two angles, the first one is to address technical aspects and general production, and the second is to review the software's goals and the therapeutic techniques that the informatic programs use.
The software development process in general, was carried out in the following stages:
Research of techniques: During this stage, appropriate techniques of CBT were reviewed to address a specific cognitive problem, but also these techniques should be feasible to use as a software.
Script writing based on the techniques already selected: a script is developed taking into consideration the techniques for story mode, which, should be consistent.
Art design (characters and environments) taking as a guideline the needs of the script: In this part the visual elements are developed to convey with the elements of the narrative.
Voice recording: For the square breathing technique an animation was developed to leads the subject for relaxation, this multimedia element needed the voice of the avatar to guide the subject while having closed eyes.
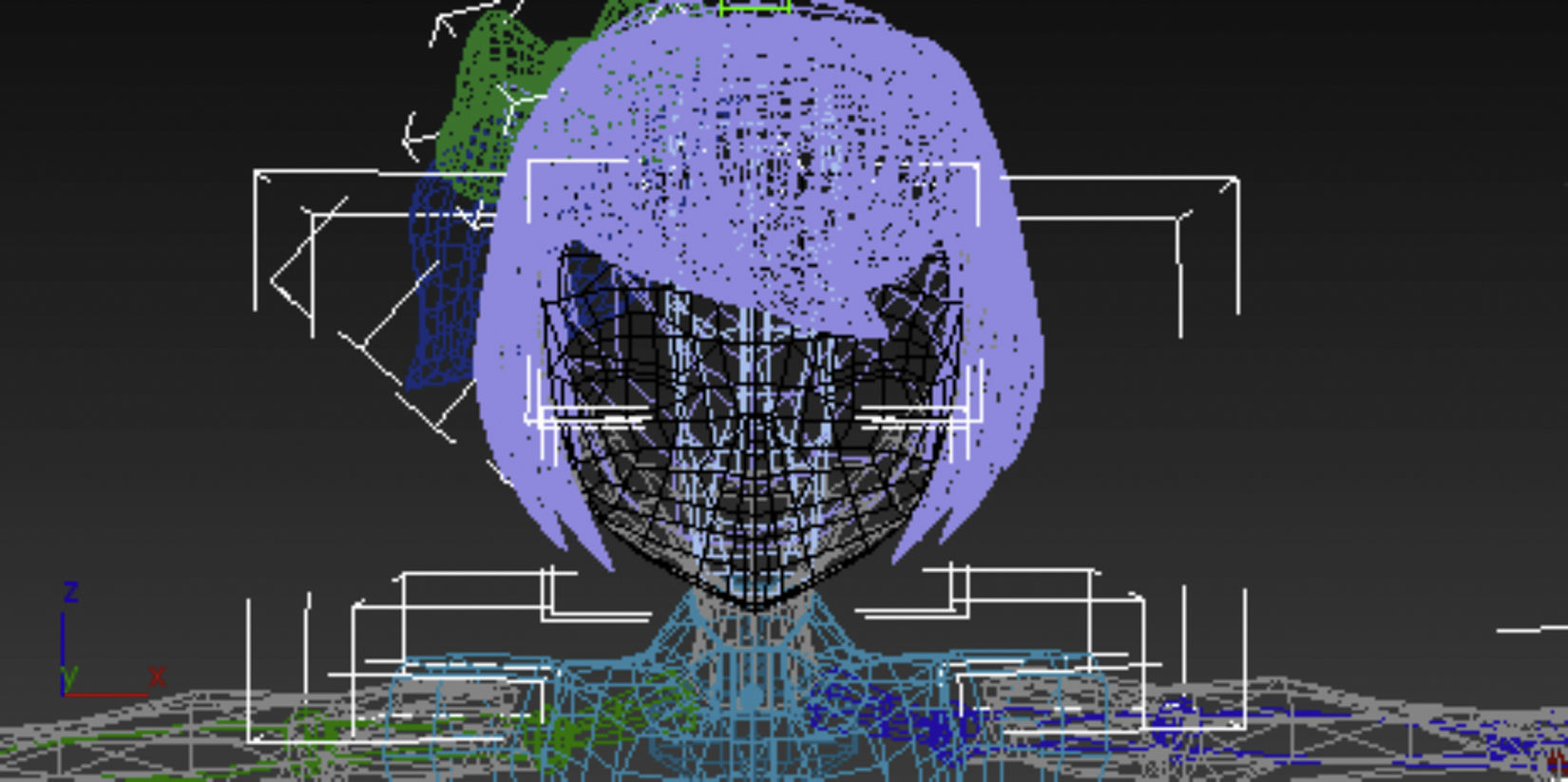
Development of graphic elements and animations: Based on the art design, the final elements that were required for the software where produced, including 3D modeling (Fig. 1), animation and 2d pictures.

Programming: This step corresponds to software development with the use of a programming language, in this case was chosen one with a wide range of compatibility, which is described in a later section.
Evaluation and correction: After the programming phase, software function tests were performed to detect errors in programming and texts; errors detected were corrected during this stage.
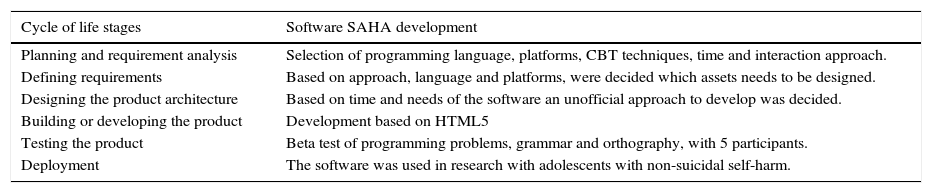
The realization of the program did not follow the traditional life cycle for software (Tabares, Alferez, & Alferez, 2009) development or SDLC (Software Development Life Cycle) however in Table 1, a relation is made.
Cycle of life relation.
| Cycle of life stages | Software SAHA development |
|---|---|
| Planning and requirement analysis | Selection of programming language, platforms, CBT techniques, time and interaction approach. |
| Defining requirements | Based on approach, language and platforms, were decided which assets needs to be designed. |
| Designing the product architecture | Based on time and needs of the software an unofficial approach to develop was decided. |
| Building or developing the product | Development based on HTML5 |
| Testing the product | Beta test of programming problems, grammar and orthography, with 5 participants. |
| Deployment | The software was used in research with adolescents with non-suicidal self-harm. |
This application's development was made with HTML5, this provide low cost and compatibility with a range of operative systems (OS) and platforms; HTML5 is a web based language that almost every internet navigator can use. When the SAHA application was developed the language do not provide the best support for audio and video, so different techniques were used according to the OS of the software.
The software version for Windows used HTML5 except for audio and video reproduction, in this case were used Flash. Android version was developed with HTML5 only, since there is no compatibility of Flash Player with the operating system, the animation was limited to a single scene and there was no audio playback. By the time this article was written, the problems with audio and video is solved in HTML5.
It was decided not to make the iOS and/or Mac OS X version, the cost involved is high because it is required to buy additional hardware for the publication; however, if is necessary operating systems like Linux, iOS and/or Mac OS X could access the application through a Web browser, with minimal compatibility issues.
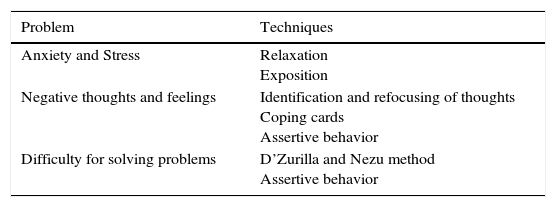
For the development of the program's content with regard to CBT, a relation was made between the needs of the cognitive and the techniques that could cover it (Table 2).
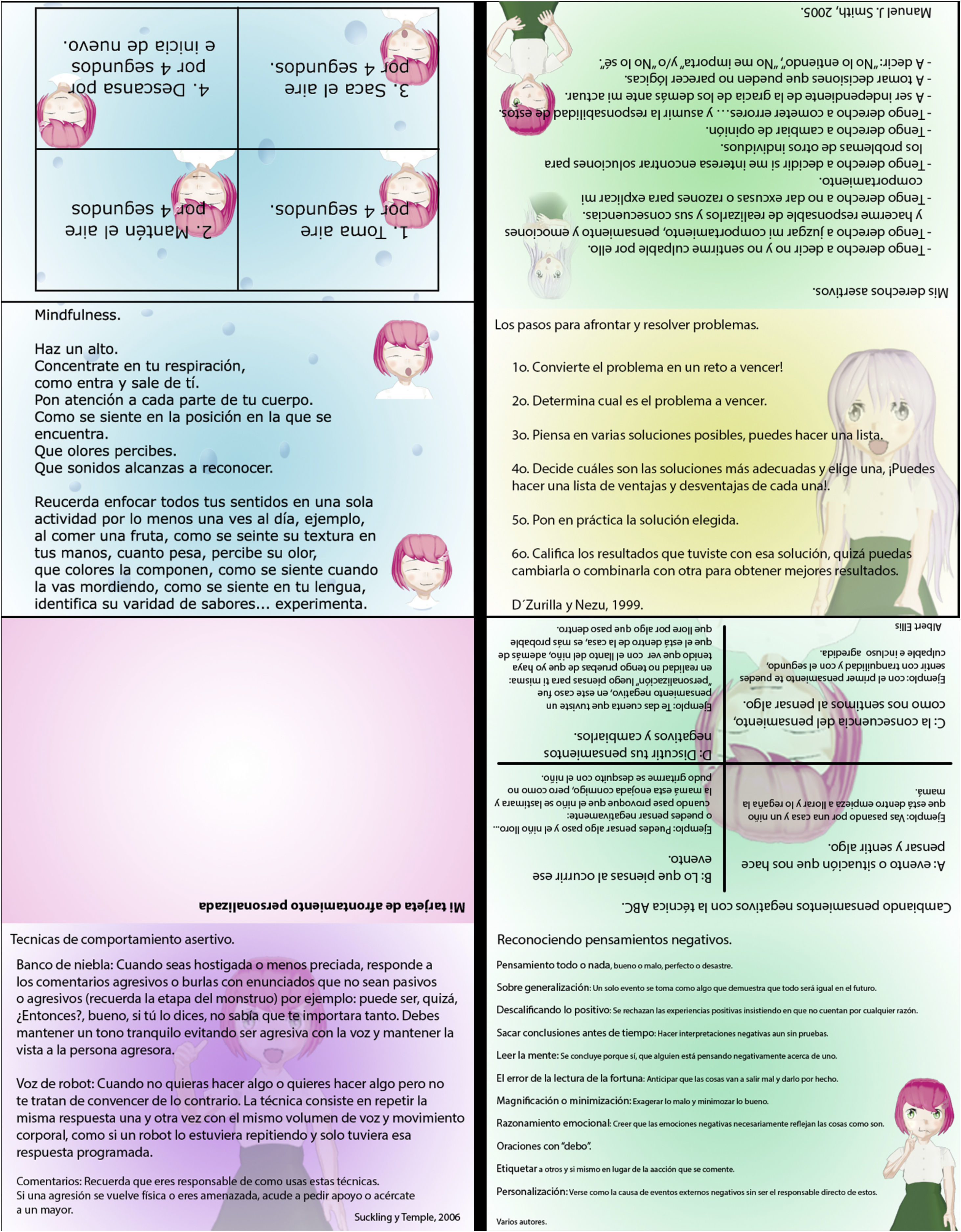
SAHA software is based on six sessions and every session is complemented by the therapist in a later discussion, also the use of coping cards is required which serve to remind the patient the coping techniques at any place and time of a regular day.
The first session of the software corresponds to the guided practice of relaxation technique called mindfulness (Didonna, 2008) and “square breathing” (Drewes, 2009). For the square breathing technique, the avatar performs the technique and instructs (Fig. 2) through audio, for mindfulness technique, another avatar explains how to perform the technique as a conversation.

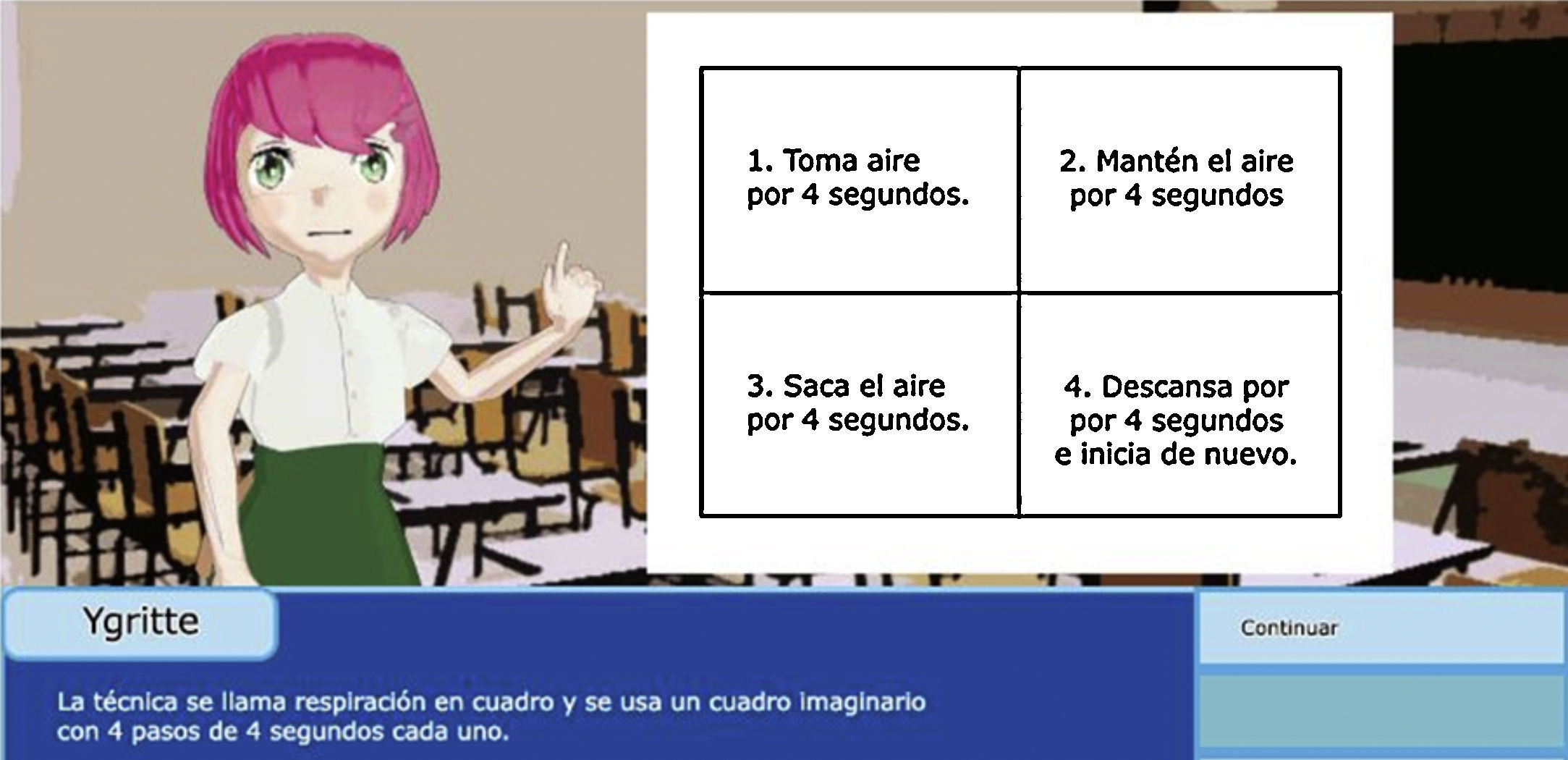
Second session includes the technique for troubleshooting of D’Zurilla and Nezu (1999), in this session the avatar faces a problem and the patient make decisions to help the avatar to solve it, then the subject review the procedure (Fig. 3) to solve problems.

During the third session a didactic approach to assertive behavior was made in software and for assertive rights knowledge, coping cards where used. When the subject interact in the session 3, the avatar will be presented to several problems and situations, then, the subject will be asked to help the avatar to resolve them, every decision will have immediate feedback, informing whether it was an assertive, aggressive or passive decision in the case of the latter two, the subject will be told the reason why the decision was passive or aggressive.
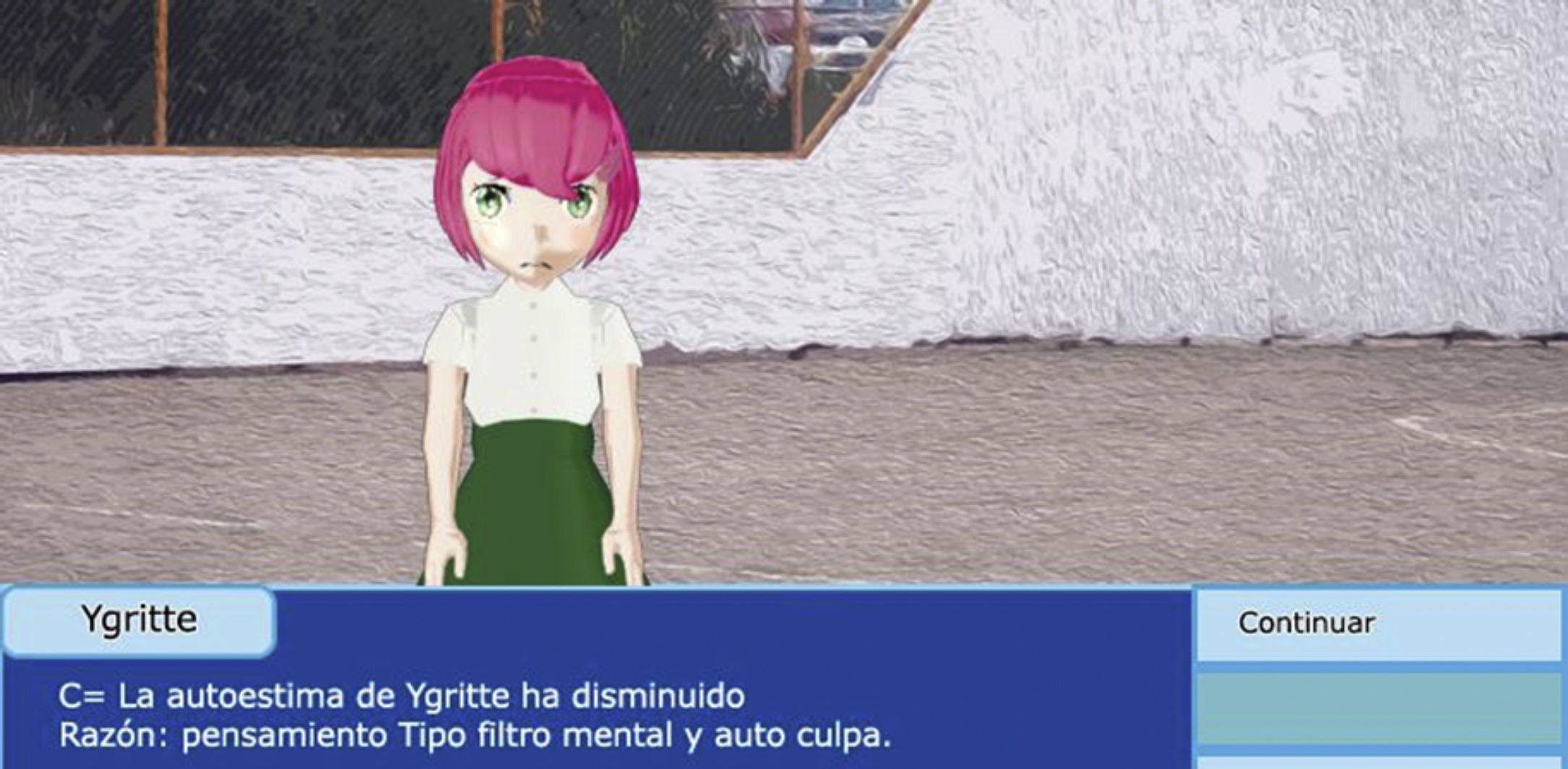
The fourth and fifth sessions include a technique for the identification, detection and refocusing of negative thoughts that the avatar experience during the history of the sessions (Fig. 4), the method of cognitive restructuration is based on the ABC technique Albert Ellis (Caballo, 2008).

The final session emphasizes in coping skills and assertiveness techniques as “fog bank” and “scratched disc” (Smith & Sharp, 1994), the latter is adapted by Amelia Suckling as the technique of “robot voice” to facilitate implementation and greater understanding in younger people (Suckling & Temple, 2006). This being the last session, is developed like a typical videogame boss, and the user is expected to put into practice what he learned in previous sessions.
ResultsThis document describes the development of software to increase coping skills in adolescents, it was revised from a point of view of general and specific production with regard to behavioral problems and techniques to deal with them.
In the general development it was detected the need for programming languages that are compatible on different OS, so the possibilities of use are increased for many platforms as a personal computer, mobile phone and web browsers.
In the particular development, the need to investigate appropriate techniques to facilitate their translation to software with minimal modification from the original therapeutic strategy was discussed.
ConclusionsBased on SDLC in his 5th Stage which is “testing the product” the software pass through a beta testing process to ensure academic quality where PhD in psychology Rocio Hernandez-Pozo and MA in psychology Enrique Berra test the correct use of language, on other hand, to find functionality errors participate as beta testers a psychologist, and teenagers (Annex 2 for full credits).
The software visits different techniques that traditionally have been used to improve coping capacities in adolescents, but is pending to review the operation of the same techniques modified for application via software. In addition, it is considered that can be made more sessions for each technique in the program, this could help to, through constant review of the techniques, can relate when and how to apply, assimilate and generalize such schemes (APA, 2013), so, sooner or later the patient can make part of his daily life the coping techniques.
Authors’ contributionAuthors contributed to the study in the following manner: MAML: design and test of the software, data collection, writing of the paper, translation. MRHP: supervision of the construction of the software, review of the draft and final version of the paper.

| Production, animation, 3d modeling, editing, programming: |
| Miguel Ángel Munóz López |
| Academic direction: |
| Dr. María del Rocío Hernández Pozo |
| Academic Dictamination: |
| Lic. Cristina González Méndez |
| Mtro. Enrique Berra Ruiz |
| Ygritte Voice: |
| Miriam Selene Villalpando Hernández |
| Character design: |
| Eva Lucia Criado Saenz |
| Miguel Ángel Muñoz López |
| Beta testers: |
| Siegfried Uriel Muñoz Romero |
| Miriam Selene Villalpando Hernández |
| María Guadalupe Muñoz López |
| Dr. María del Rocío Hernández |
Peer review under the responsibility of Asociación Mexicana de Comportamiento y Salud.