





The aim of this study was to assess the diagnostic value of several markers for tuberculosis pleural effusion (TPE) using the combined analysis of Lactate dehydrogenase (LDH), Carbohydrate antigen 125 (CA125), Cytokeratin-19 fragment (CYFRA21-1).
MethodsFrom January to December in 2018, a total of 37 patients with pleural effusion (22 cases of transudative pleural effusion, 15 cases of tuberculosis pleural effusion and 22 cases of Transudative pleural effusion who were hospitalized in our hospital were reviewed. Receiver operating characteristic (ROC) curves and logistic regression equations was used to evaluate the diagnostic efficiency of each marker.
ResultsThe levels of LDH and CYFRA21-1 of tuberculosis pleural effusions were obviously higher than those of transudative pleural effusion with statistically significant difference (<0.05). The areas under the ROC curve of LDH, CA125 and CYFRA21-1 were 0.92, 0.344 and 0.656, respectively. The diagnostic sensitivity of LDH, CA125 and CYFRA21-1 were 100%, 13.3%, 73.3%, respectively. The combined detection of LDH, CA125 and CYFRA21-1 were higher than those of any other combinations of the indexes.
ConclusionsThe study showed a high diagnostic sensitivity and specificity of combined speculation of LDH, ADA and CYFRA21-1 in Tuberculosis pleural effusion.
El objetivo de este estudio fue evaluar el valor diagnóstico de diversos marcadores de derrame pleural tuberculoso (DPTB) utilizando el análisis combinado de lactato deshidrogenasa (LDH), antígeno carbohidrato 125 (CA-125) y fragmento de citoqueratina-19 (CYFRA 21-1).
MétodosDe enero a diciembre de 2018, revisamos un total de 37 pacientes hospitalizados en nuestro hospital con derrame pleural (22 casos de derrame pleural trasudativo y 15 casos de derrame pleural tuberculoso). Se utilizaron las curvas ROC y ecuaciones de regresión logística para evaluar la eficacia diagnóstica de cada marcador.
ResultadosLos niveles de LDH y CYFRA 21-1 de los pacientes con derrame pleural tuberculoso fueron obviamente superiores a los pacientes con derrame pleural trasudativo, con diferencia estadísticamente significativa (p<0,05). Las áreas bajo la curva ROC de LDH, CA-125 y CYFRA 21-1 fueron 0,92, 0,344 y 0,656, respectivamente. La sensibilidad diagnóstica de LDH, CA-125 y CYFRA 21-1 fueron del 100, 13,3 y 73,3%, respectivamente. La detección combinada de LDH, CA-125 y CYFRA 21-1 fue superior a cualesquiera otras combinaciones de los índices.
ConclusionesEl estudio reflejó una alta sensibilidad diagnóstica y especificidad del análisis combinado de LDH, ADA y CYFRA 21-1 en el derrame pleural tuberculoso.
Pleural effusion, which is characterized by pathological and physiologic fluid accumulation in the pleural space, is a common clinical symptom. Exudative pleural effusion is usually pathological originate such as inflammation, tuberculosis and cancer.1 In clinical practice, Benign and malignant pleural effusions often develop secondary to tuberculous and lung cancer, respectively.2 The parameters that are usually available and commonly measured in pleural effusion are useful for the separation of transudates from exudates but often they do not contribute to the diagnosis of the underlying disease.3 Therefore, the different judgement and management for the disease could influence the development t of the disease and its clinical outcome. This review has an overview of transudative pleural effusion and tuberculosis pleural effusion, for the sake of evaluating the application of the LDH, CA125 and CYFRA21-1 in pleural fluid as a novel parametric biomarker to differentiate transudative pleural effusion from tuberculosis pleural effusion.
Materials and methodsPatients studyThis study retrospectively analyzed the clinical information of 22 patients diagnosed as transudative pleural effusion and 15 patients diagnosed as tuberculosis pleural effusion in Ruijin Hospital of Affiliated Hospital of Shanghai Jiao Tong University School between January and December in 2018.
Through clinical manifestations, analysis and a chest radiograph (posteroanterior and lateral, showing pleural-based opacity obscuring the diaphragm), patients with suspected diagnosis of pleural effusion was made in all cases. The diagnosis was made sure through thoracocentesis, along with biochemical and/or microbiological examination analysis of the pleural fluid.4
Statistical analysesThe SPSS 22.0 software package was performed to complete the analyses. Data are demonstrated as X±S for normal distribution data and the Median value (P25-P75) for abnormal distribution of these data. The Mann-Whitney was employed to assess differences in LDH, ADA and CYFRA21-1 concentration in transudative pleural effusion and tuberculosis pleural effusion (TPE). The ROC curve was used to evaluate the diagnostic accuracy of LDH, CA125 and CYFRA21-1 for differentiating tuberculosis pleural effusion (TPE) and Transudative pleural effusion. The AUC values close to 1 refer to great diagnostic accuracy, but AUC values as low as 0.5 presents poor diagnostic accuracy. The comparison among AUCs was assessed employing logistic regression analysis and the ROC curve was produced using SPSS 22.0 package. When a P-value is only less than 0.05, the data was statistically significant.
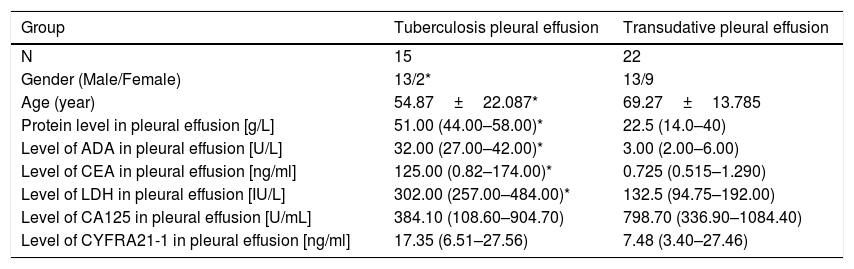
ResultsStudy peopleThere were 22 patients diagnosed as transudative pleural effusion and 15 patients diagnosed as tuberculosis pleural effusion. Characteristics of the two groups are presented in Table 1. Mean (±standard deviation (SD) age was 54.87±22.087 years for the Tuberculosis pleural effusion group and 69.27±13.785 years for Transudative pleural effusion. The protein, ADA and CEA in pleural effusion level are significantly difference (P<0.05) (Table 1).
General characteristics of patients in various groups.
| Group | Tuberculosis pleural effusion | Transudative pleural effusion |
|---|---|---|
| N | 15 | 22 |
| Gender (Male/Female) | 13/2* | 13/9 |
| Age (year) | 54.87±22.087* | 69.27±13.785 |
| Protein level in pleural effusion [g/L] | 51.00 (44.00–58.00)* | 22.5 (14.0–40) |
| Level of ADA in pleural effusion [U/L] | 32.00 (27.00–42.00)* | 3.00 (2.00–6.00) |
| Level of CEA in pleural effusion [ng/ml] | 125.00 (0.82–174.00)* | 0.725 (0.515–1.290) |
| Level of LDH in pleural effusion [IU/L] | 302.00 (257.00–484.00)* | 132.5 (94.75–192.00) |
| Level of CA125 in pleural effusion [U/mL] | 384.10 (108.60–904.70) | 798.70 (336.90–1084.40) |
| Level of CYFRA21-1 in pleural effusion [ng/ml] | 17.35 (6.51–27.56) | 7.48 (3.40–27.46) |
The levels of LDH and CYFRA21-1 of Tuberculosis pleural effusion were obviously higher than those of Transudative pleural effusion, The levels of LDH of Tuberculosis pleural effusion were statistically significant (P<0.05) (Table 1).
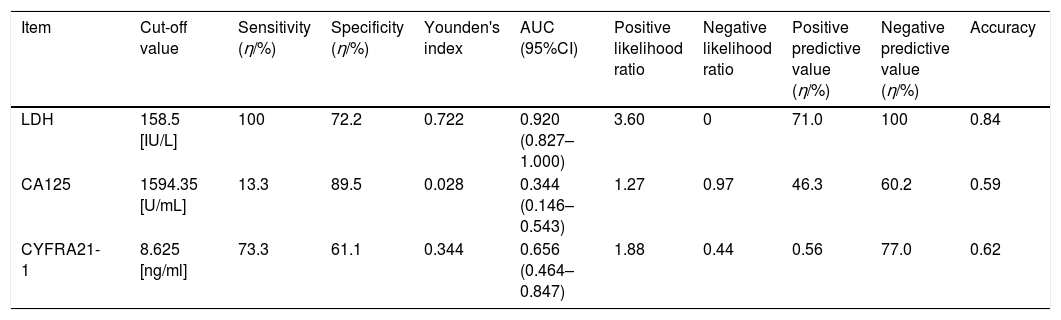
Diagnostic values of LDH, CA125, CYFRA21-1 in diagnosing Transudative pleural effusion and Tuberculosis pleural effusionThe areas under the ROC curve of LDH, CA125 and CYFRA21-1 were 0.920, 0.344 and 0.656, respectively; The diagnostic sensitivity of LDH, CA125 and CYFRA21-1 were 100%, 13.3% and 73.3%, respectively; Negative predictive value of three indexes were 100%, 60.2%, 77.0%, respectively; Accuracy of three indexes were 0.84, 0.59, 0.62, respectively (Table 2).
The ROC analysis of LDH, 125, FRA21-1 in diagnostic value of tuberculous pleural effusion.
| Item | Cut-off value | Sensitivity (η/%) | Specificity (η/%) | Younden's index | AUC (95%CI) | Positive likelihood ratio | Negative likelihood ratio | Positive predictive value (η/%) | Negative predictive value (η/%) | Accuracy |
|---|---|---|---|---|---|---|---|---|---|---|
| LDH | 158.5 [IU/L] | 100 | 72.2 | 0.722 | 0.920 (0.827–1.000) | 3.60 | 0 | 71.0 | 100 | 0.84 |
| CA125 | 1594.35 [U/mL] | 13.3 | 89.5 | 0.028 | 0.344 (0.146–0.543) | 1.27 | 0.97 | 46.3 | 60.2 | 0.59 |
| CYFRA21-1 | 8.625 [ng/ml] | 73.3 | 61.1 | 0.344 | 0.656 (0.464–0.847) | 1.88 | 0.44 | 0.56 | 77.0 | 0.62 |
Comparing the AUCs of single index in Transudative pleural effusion groups VS. Tuberculosis pleural effusion.
The diagnostic sensitivity and specificity of combined speculation of LDH, CA125 and CYFRA21-1 were higher than those of any other combinations of the indexes. The diagnostic sensitivity and specificity of combined speculation of LDH, ADA and CYFRA21-1 were 100% and 84.2%, respectively. The areas under the ROC curve was 0.944(95%CI: 0.865–1.000). The Younden's index of combined detection of three indexes was 0.842 (Table 3).
Diagnostic values of combined detection of LDH, 125, FRA21-1 in differentiating Transudative pleural effusion from Tuberculosis pleural effusion.
| combined detection | AUC(95%CI) | Sensitivity(η/%) | Specificity(η/%) | Younden's index |
|---|---|---|---|---|
| LDH+CA125 | 0.930 (0.845–1.000) | 93.3 | 84.2 | 0.775 |
| LDH+CYFRA21-1 | 0.916 (0.823–1.000) | 100 | 73.7 | 0.737 |
| CA125+CYFRA21-1 | 0.764 (0.598–0.925) | 80 | 68.4 | 0.484 |
| LDH+CA125+CYFRA21-1 | 0.944 (0.865–1.000) | 100 | 84.2 | 0.842 |
Comparing the area under ROC curve of combined indexes in Transudative pleural effusion group vs. Tuberculosis pleural effusion group.
LDH is a cytoplasmatic enzyme prevailing in almost all major organs and systems, usually rises in serums as a respond to a non-specific manner that leads to cellular injury or cellular death.8 An increasing LDH level in pleural fluid with exudative pleural effusion patients usually indicate pulmonary or pleural tissue injury and endothelial damage.5,6 CA-125 antigen is a glycoprotein which is expressed in the amnion and embryonic coelomic epithelium, Some studies have showed that stimulation of some inflammatory factors such as IL-6 and TNF-a could increase the secretion of CA125.6,7 CYFRA21-1 is an kind of acidic (type I) intermediate filament protein and also a part of the cellular cytoskeleton,8 its concentration is very little in healthy people,9 Studies have suggested that there is a lightly increase in CYFRA21-1 in inflammation and tumor.6,10 Thus, CYFRA21-1 could be separated from the cytoskeleton of epithelial cells as a consequence of cell damage9 and CYFRA21-1 could be used for a new biomarker for tuberculosis pleural effusion and malignant pleural effusion.
In our study, according to tuberculosis pleural effusions, The levels of LDH and CYFRA21-1 of tuberculosis pleural effusions were obviously higher than those of transudative pleural effusion with statistically significant difference (P<0.05).The areas under the ROC curve of LDH, CA125 and CYFRA21-1 were 0.92, 0.344 and 0.656, respectively. Although the detection of CA125 and cytokeratin 19 alone is of little significance in the diagnosis of tuberculous pleural effusion, the combined detection of LDH, CA125 and CYFRA21-1 were higher than those of any other combinations of the indexes The diagnostic sensitivity and specificity of combined speculation of LDH, ADA and CYFRA21-1 were 100% and 84.2%, respectively; The areas under the ROC curve was 0.944. The combined detection of LDH, CA125 and CYFRA21-1 could contribute to the diagnosis of tuberculosis pleural effusions.
ConclusionDiagnostic methods currently focus on diagnosing tuberculous pleural effusion. The judgement will contribute to form the basis of treatment strategies and ultimately gain great clinical prognosis. The combined detection of three indexes has important clinical reference in differential diagnosis of the tuberculous pleural effusion.
Authors’ contributionsThe data were collected, progressed and analyzed data by Hongxia Lin, then, she completed this manuscript. Lei Ni reviewed and edited the manuscript. All authors read and approved the manuscript. Acknowledgements: I would like to extend my sincere gratitude to the foundation of the Shanghai Natural Science Foundation (15ZR1426200) in the completion of this thesis.
FundingThis study was financially supported by a grant from the Shanghai Natural Science Foundation (15ZR1426200).
Conflict of interestsThe authors declare that they have no conflict of interest.
