




We previously reported an increase in respiratory mortality in 2020 in Spain after COVID-19. It is unclear if this rise is sustained in the longer-term. We aimed to determine whether respiratory mortality in 2021 in Spain returned to pre-pandemic levels.
Material and methodsIn an observational, large study using official National Institute of Statistics data, we explored deaths due to respiratory diseases, that is, all causes of death by the standard WHO list of diseases of the respiratory system plus COVID-19, tuberculosis and lung cancer. Using the latest available official data of Spain, we analyzed changes in the mortality pattern in Spain from January 2019 to December 2021. We endorsed STROBE guidance for observational research.
ResultsThere were 98,714 deaths due to respiratory diseases in 2021 in Spain, corresponding to 21.9% of all deaths, becoming second in the ranking of causes of death. Respiratory diseases mortality in Spain has not returned to pre-pandemic levels in 2021, still with an increase of 30.3% (95% CI 30.2–30.4) compared to rates in 2019. All respiratory-specific causes of death decreased in 2021, except for lung cancer, that increased in women and decreased in men compared to 2019 (both p<0.05). In a multivariate analysis some established risk factors for respiratory diseases mortality were confirmed, such as male gender and older age; further, an association with reduced mortality in rural Spain was observed, still with a large geographical variability.
ConclusionsThe COVID-19 pandemic has had a lasting impact on deaths due to respiratory diseases and certain specific causes of death in 2021, and it has disproportionately affected certain regions.
Previamente informamos de un aumento de la mortalidad respiratoria en 2020 en España tras la COVID-19. No está claro si este aumento se mantiene a largo plazo. Nuestro objetivo fue determinar si la mortalidad respiratoria en 2021 en España volvió a los niveles previos a la pandemia.
MétodosEn un gran estudio observacional con datos oficiales del Instituto Nacional de Estadística exploramos las muertes por enfermedades respiratorias, es decir, todas las causas de muerte según la lista estándar de enfermedades del sistema respiratorio de la Organización Mundial de la Salud más COVID-19, tuberculosis y cáncer de pulmón. Utilizando los últimos datos oficiales disponibles de España analizamos los cambios en el patrón de mortalidad en España desde enero de 2019 hasta diciembre de 2021. Seguimos la guía STROBE para investigación observacional.
ResultadosSe produjeron 98.714 muertes por enfermedades respiratorias en 2021 en España, lo que corresponde a 21,9% del total de muertes, situándose en el segundo lugar del ranking de causas de muerte. La mortalidad por enfermedades respiratorias en España no ha vuelto a los niveles previos a la pandemia en 2021, aun con un aumento de 30,3% (IC 95% 30,2-30,4) respecto a las tasas de 2019. Todas las causas de muerte específicas de las vías respiratorias disminuyeron en 2021, excepto el cáncer de pulmón, que aumentó en mujeres y disminuyó en hombres en comparación con 2019 (ambos p < 0,05). En un análisis multivariado se confirmaron algunos factores de riesgo establecidos para la mortalidad por enfermedades respiratorias, como el género masculino y la edad avanzada; además, se observó una asociación con la reducción de la mortalidad en la España rural, aun con una gran variabilidad geográfica.
ConclusionesLa pandemia de COVID-19 ha tenido un impacto duradero en las muertes por enfermedades respiratorias y ciertas causas específicas de muerte en 2021, y ha afectado de manera desproporcionada a ciertas regiones.
The COVID-19 pandemic has had a significant impact on mortality around the world, with many countries experiencing a surge in deaths during the initial months of the pandemic. We previously reported an increase in respiratory mortality in 2020 in Spain, with a corresponding decrease in other due to substitution of causes of death.1
Others have reported increases in cancer and chronic conditions mortality, such as diabetes, cardiovascular diseases, and some oncological diseases, related with the interruption of population-based early detection programmes and diagnostic and therapeutic delays associated with the collapse in primary care and associated hospital services, adding significant stress to already overstretched health systems.2 Many of these general, global aspects need to be implemented and carefully assessed in Spain.3 Three years and counting from the onset of the COVID-19 pandemic,4 with the perspective of seven pandemic waves, and with a population vaccination coverage above 80% in most age strata in Spain, it is unclear if this mortality rise will sustain in the longer-term.
The diseases of the respiratory “system” in the current classification of the WHO (and any competent national bodies) do not fully reflect the reality of all diseases certainly affecting the respiratory system, and do not include conditions that are part of the day-to-day care of patients by pulmonologists, such as tuberculosis, lung cancer or COVID-19 itself, among others. A dialogue to try to correct and interpret well future statistics remains necessary.
In this research, we aimed to determine whether proportionate mortality by respiratory diseases, including tuberculosis, lung cancer and COVID-19 in Spain returned to pre-pandemic levels before COVID-19 in 2021.
MethodsWe endorsed STROBE guidance for observational research.5 We had a particular interest in deaths due to respiratory diseases, that is all causes of death by the standard WHO list of diseases of the respiratory system plus COVID-19, tuberculosis and lung cancer. Using the latest available data from the Instituto Nacional de Estadística (INE) of Spain,6,7 we analyzed proportionate mortality trends in Spain from January 2019 to December 2021. In particular, we used 2019 as the reference year, free from COVID-19, and report proportionate mortality in 2020 and in 2021.
Mortality microdata were obtained from the INE website.8 As previously indicated,1 the so-called Short List of 101 causes of death ICD-10, and its correspondence with ICD-9, was reviewed and regrouped for Group VIII – Diseases of the respiratory system: Flu; Pneumonia; Chronic diseases of the lower respiratory tract (except asthma); Asthma; Respiratory insufficiency; and Other diseases of the respiratory system; and also other diseases of the respiratory system such as tuberculosis, or of daily practice in the field of Pulmonology such as malignant tumours of the trachea, bronchi and lung, were added as respiratory causes of death (what we have labelled as Group VIII-bis). The causes “COVID-19 Virus identified” and “COVID-19 Virus not identified (suspected)” were also included (Table 1). A descriptive analysis of the absolute frequencies of deaths and proportionate mortality by gender, age, and Autonomous Communities (regions) was performed. The percentages of change in proportionate mortality between pre-pandemic (2019) and post-pandemic (2020 and 2021) years were calculated. A crude and multivariable logistic regression analysis was performed with the microdata to obtain the odds ratios (ORs) and their 95% confidence interval (CI), as estimators of the association of the independent variables with mortality. We had a new, particular interest in an analysis by size of the location and location of birth of those deceased. In any comparison, a value of p<0.05 was considered statistically significant.9–11
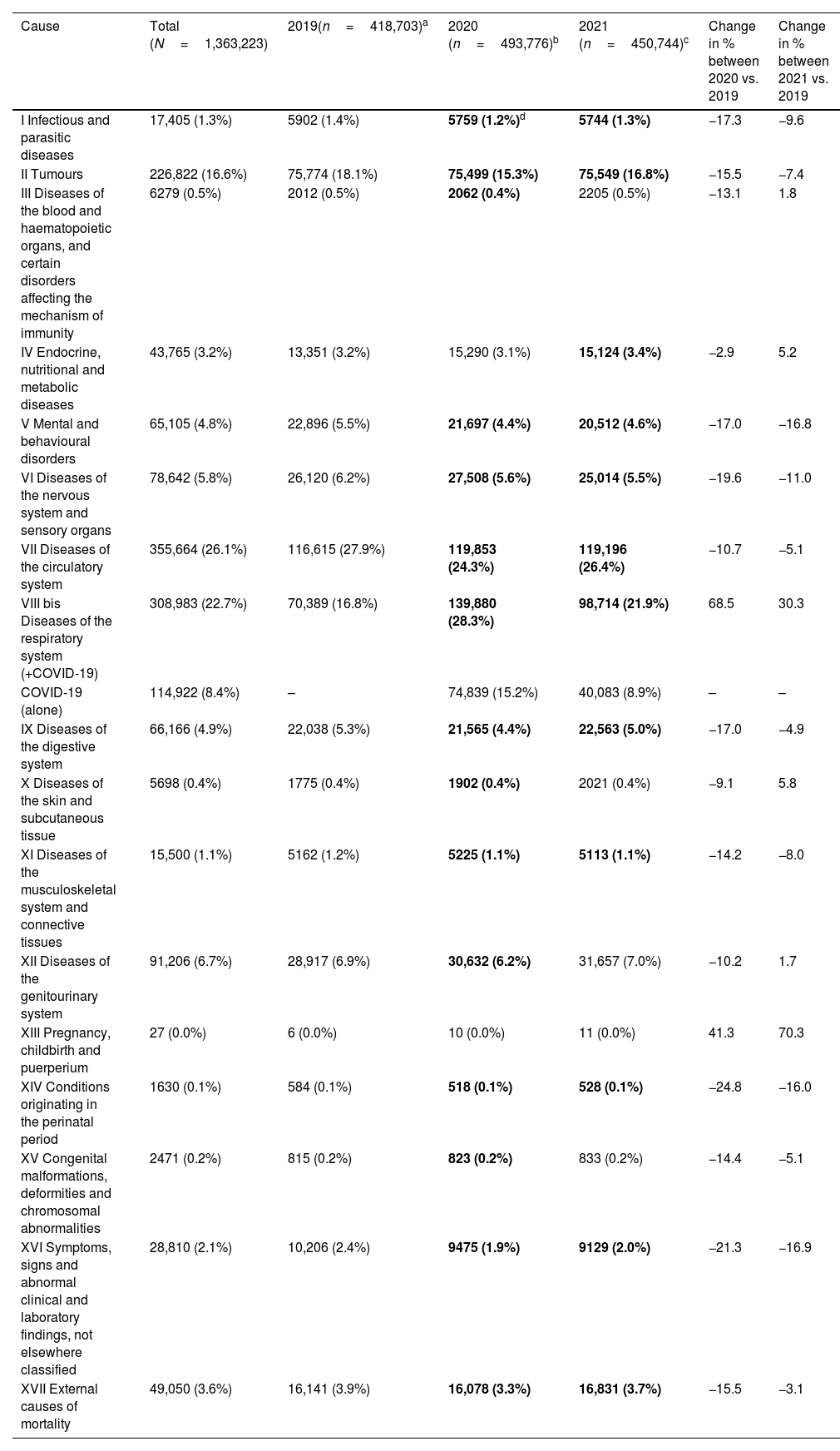
Number of deaths, proportionate mortality (%) and percent change by causes of death in Spain in 2019, 2020 and 2021.
| Cause | Total (N=1,363,223) | 2019(n=418,703)a | 2020 (n=493,776)b | 2021 (n=450,744)c | Change in % between 2020 vs. 2019 | Change in % between 2021 vs. 2019 |
|---|---|---|---|---|---|---|
| I Infectious and parasitic diseases | 17,405 (1.3%) | 5902 (1.4%) | 5759 (1.2%)d | 5744 (1.3%) | −17.3 | −9.6 |
| II Tumours | 226,822 (16.6%) | 75,774 (18.1%) | 75,499 (15.3%) | 75,549 (16.8%) | −15.5 | −7.4 |
| III Diseases of the blood and haematopoietic organs, and certain disorders affecting the mechanism of immunity | 6279 (0.5%) | 2012 (0.5%) | 2062 (0.4%) | 2205 (0.5%) | −13.1 | 1.8 |
| IV Endocrine, nutritional and metabolic diseases | 43,765 (3.2%) | 13,351 (3.2%) | 15,290 (3.1%) | 15,124 (3.4%) | −2.9 | 5.2 |
| V Mental and behavioural disorders | 65,105 (4.8%) | 22,896 (5.5%) | 21,697 (4.4%) | 20,512 (4.6%) | −17.0 | −16.8 |
| VI Diseases of the nervous system and sensory organs | 78,642 (5.8%) | 26,120 (6.2%) | 27,508 (5.6%) | 25,014 (5.5%) | −19.6 | −11.0 |
| VII Diseases of the circulatory system | 355,664 (26.1%) | 116,615 (27.9%) | 119,853 (24.3%) | 119,196 (26.4%) | −10.7 | −5.1 |
| VIII bis Diseases of the respiratory system (+COVID-19) | 308,983 (22.7%) | 70,389 (16.8%) | 139,880 (28.3%) | 98,714 (21.9%) | 68.5 | 30.3 |
| COVID-19 (alone) | 114,922 (8.4%) | – | 74,839 (15.2%) | 40,083 (8.9%) | – | – |
| IX Diseases of the digestive system | 66,166 (4.9%) | 22,038 (5.3%) | 21,565 (4.4%) | 22,563 (5.0%) | −17.0 | −4.9 |
| X Diseases of the skin and subcutaneous tissue | 5698 (0.4%) | 1775 (0.4%) | 1902 (0.4%) | 2021 (0.4%) | −9.1 | 5.8 |
| XI Diseases of the musculoskeletal system and connective tissues | 15,500 (1.1%) | 5162 (1.2%) | 5225 (1.1%) | 5113 (1.1%) | −14.2 | −8.0 |
| XII Diseases of the genitourinary system | 91,206 (6.7%) | 28,917 (6.9%) | 30,632 (6.2%) | 31,657 (7.0%) | −10.2 | 1.7 |
| XIII Pregnancy, childbirth and puerperium | 27 (0.0%) | 6 (0.0%) | 10 (0.0%) | 11 (0.0%) | 41.3 | 70.3 |
| XIV Conditions originating in the perinatal period | 1630 (0.1%) | 584 (0.1%) | 518 (0.1%) | 528 (0.1%) | −24.8 | −16.0 |
| XV Congenital malformations, deformities and chromosomal abnormalities | 2471 (0.2%) | 815 (0.2%) | 823 (0.2%) | 833 (0.2%) | −14.4 | −5.1 |
| XVI Symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified | 28,810 (2.1%) | 10,206 (2.4%) | 9475 (1.9%) | 9129 (2.0%) | −21.3 | −16.9 |
| XVII External causes of mortality | 49,050 (3.6%) | 16,141 (3.9%) | 16,078 (3.3%) | 16,831 (3.7%) | −15.5 | −3.1 |
There were 98,714 deaths due to respiratory diseases in 2021 in Spain (VIII-bis in our classification), corresponding to 21.9% of all deaths, becoming second in the ranking of causes of death, right after diseases of the circulatory system with 119,196 (26.4%), and ahead of cancer with 75,549 (16.8%) (Table 1). Our results show that respiratory mortality in Spain has not returned to pre-pandemic levels in 2021, still with an increase of 30.3% (95% CI 30.2–30.4) compared to background rates in 2019 (it was a 68.5% (95% CI 68.4–68.6) increase in 2020).
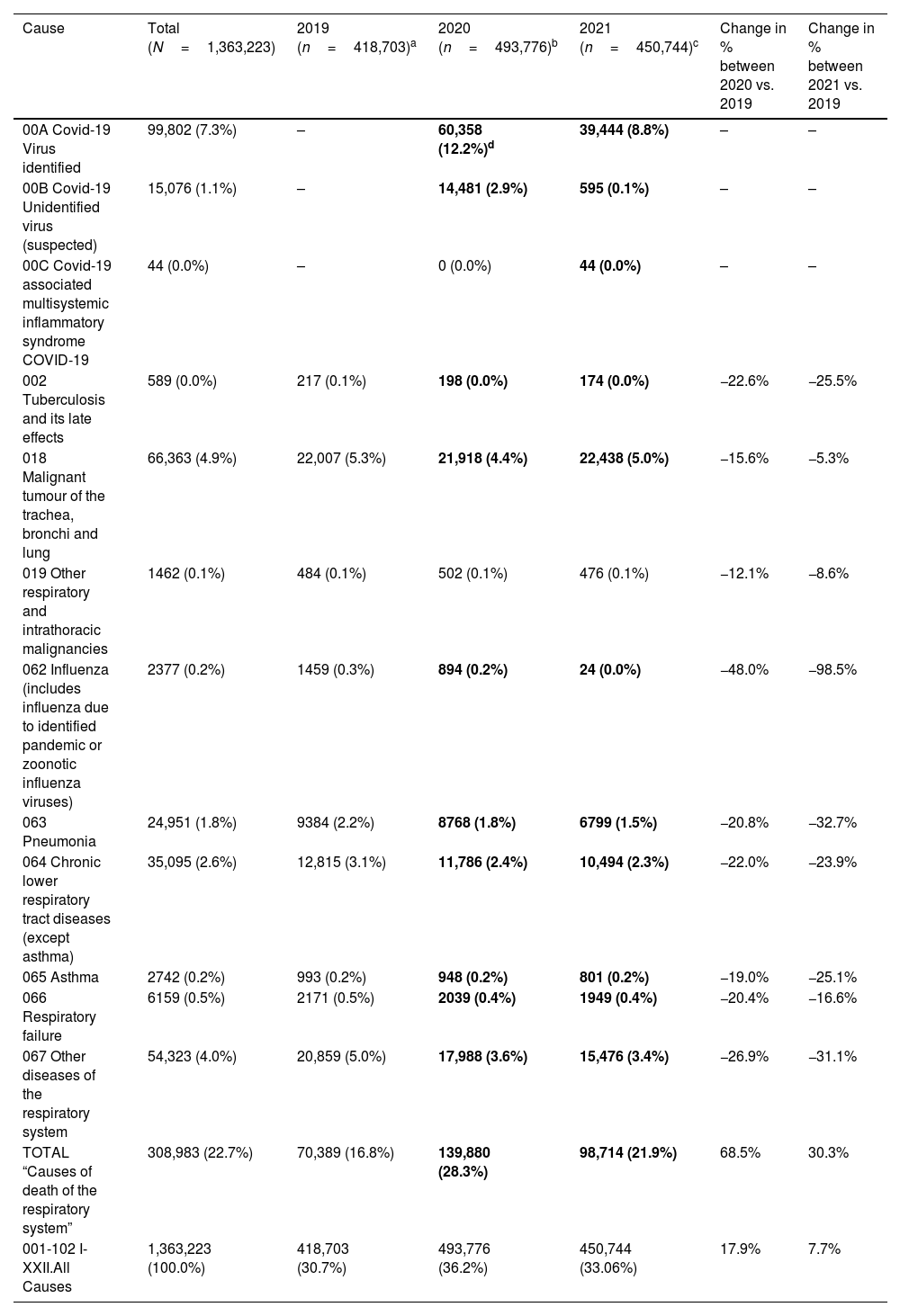
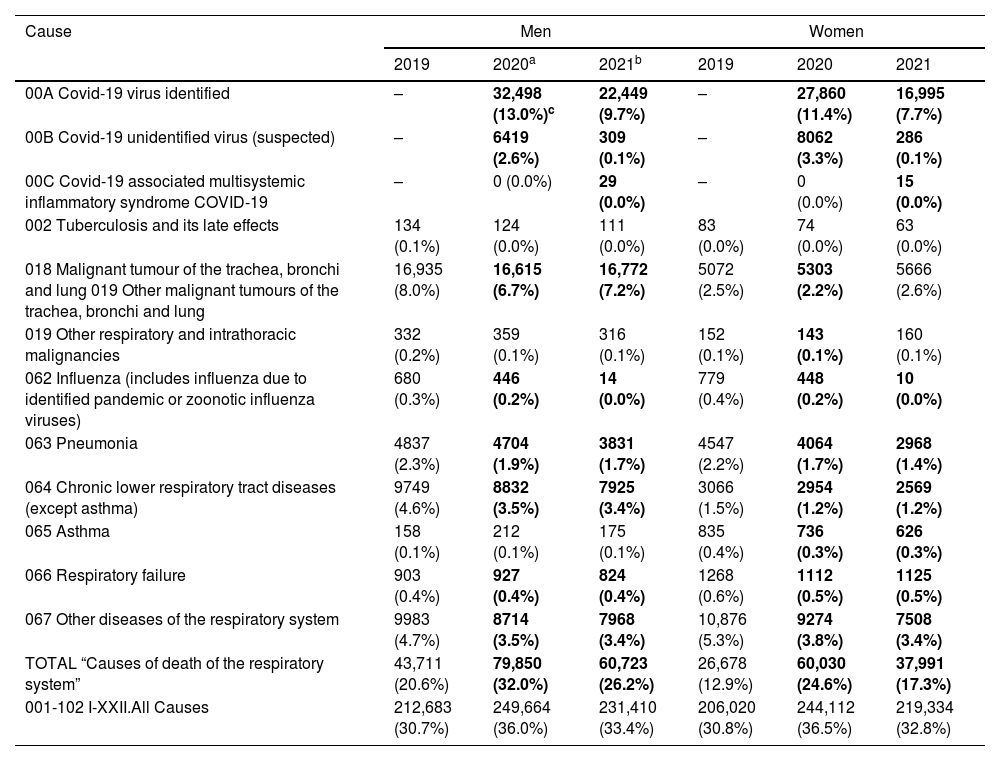
When we analyzed mortality by respiratory-specific causes of death versus 2019, we found that all significantly or nominally decreased in 2021 (Table 2), except for lung cancer, that increased in women and decreased in men compared to 2019 (both p<0.05) (Table 3 and Fig. 1). Additionally, we observed large regional differences by Autonomous Communities, with some regions experiencing a greater impact on overall, respiratory-related and specific respiratory diseases mortality compared to others.
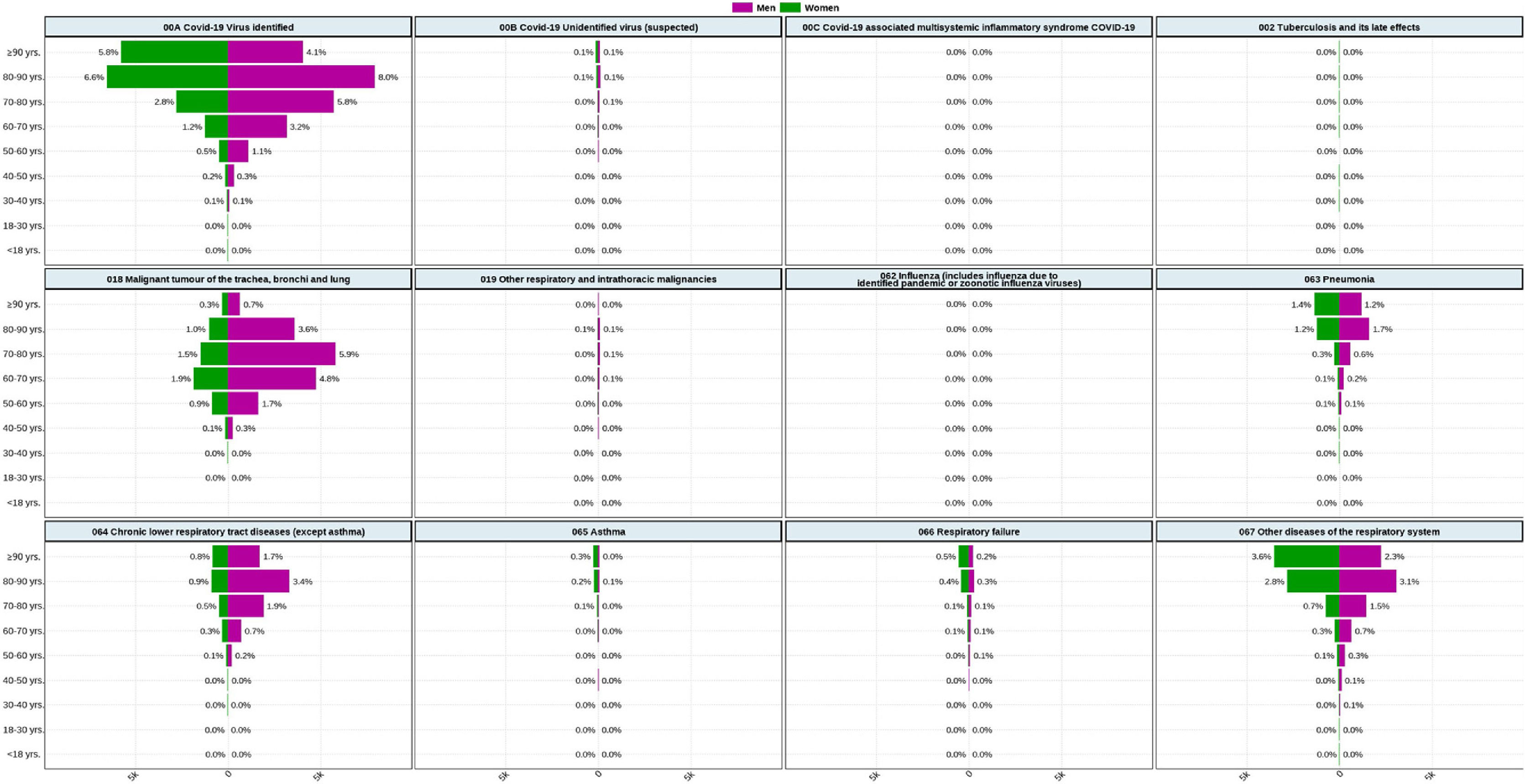
Number of deaths, proportionate mortality (%) and percent change by diseases of the respiratory system in Spain in 2019 to 2021.
| Cause | Total (N=1,363,223) | 2019 (n=418,703)a | 2020 (n=493,776)b | 2021 (n=450,744)c | Change in % between 2020 vs. 2019 | Change in % between 2021 vs. 2019 |
|---|---|---|---|---|---|---|
| 00A Covid-19 Virus identified | 99,802 (7.3%) | – | 60,358 (12.2%)d | 39,444 (8.8%) | – | – |
| 00B Covid-19 Unidentified virus (suspected) | 15,076 (1.1%) | – | 14,481 (2.9%) | 595 (0.1%) | – | – |
| 00C Covid-19 associated multisystemic inflammatory syndrome COVID-19 | 44 (0.0%) | – | 0 (0.0%) | 44 (0.0%) | – | – |
| 002 Tuberculosis and its late effects | 589 (0.0%) | 217 (0.1%) | 198 (0.0%) | 174 (0.0%) | −22.6% | −25.5% |
| 018 Malignant tumour of the trachea, bronchi and lung | 66,363 (4.9%) | 22,007 (5.3%) | 21,918 (4.4%) | 22,438 (5.0%) | −15.6% | −5.3% |
| 019 Other respiratory and intrathoracic malignancies | 1462 (0.1%) | 484 (0.1%) | 502 (0.1%) | 476 (0.1%) | −12.1% | −8.6% |
| 062 Influenza (includes influenza due to identified pandemic or zoonotic influenza viruses) | 2377 (0.2%) | 1459 (0.3%) | 894 (0.2%) | 24 (0.0%) | −48.0% | −98.5% |
| 063 Pneumonia | 24,951 (1.8%) | 9384 (2.2%) | 8768 (1.8%) | 6799 (1.5%) | −20.8% | −32.7% |
| 064 Chronic lower respiratory tract diseases (except asthma) | 35,095 (2.6%) | 12,815 (3.1%) | 11,786 (2.4%) | 10,494 (2.3%) | −22.0% | −23.9% |
| 065 Asthma | 2742 (0.2%) | 993 (0.2%) | 948 (0.2%) | 801 (0.2%) | −19.0% | −25.1% |
| 066 Respiratory failure | 6159 (0.5%) | 2171 (0.5%) | 2039 (0.4%) | 1949 (0.4%) | −20.4% | −16.6% |
| 067 Other diseases of the respiratory system | 54,323 (4.0%) | 20,859 (5.0%) | 17,988 (3.6%) | 15,476 (3.4%) | −26.9% | −31.1% |
| TOTAL “Causes of death of the respiratory system” | 308,983 (22.7%) | 70,389 (16.8%) | 139,880 (28.3%) | 98,714 (21.9%) | 68.5% | 30.3% |
| 001-102 I-XXII.All Causes | 1,363,223 (100.0%) | 418,703 (30.7%) | 493,776 (36.2%) | 450,744 (33.06%) | 17.9% | 7.7% |
Number of deaths and percentage of mortality by diseases of the respiratory system in 2019, 2020 and 2021 in Spain, by gender.
| Cause | Men | Women | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020a | 2021b | 2019 | 2020 | 2021 | |
| 00A Covid-19 virus identified | – | 32,498 (13.0%)c | 22,449 (9.7%) | – | 27,860 (11.4%) | 16,995 (7.7%) |
| 00B Covid-19 unidentified virus (suspected) | – | 6419 (2.6%) | 309 (0.1%) | – | 8062 (3.3%) | 286 (0.1%) |
| 00C Covid-19 associated multisystemic inflammatory syndrome COVID-19 | – | 0 (0.0%) | 29 (0.0%) | – | 0 (0.0%) | 15 (0.0%) |
| 002 Tuberculosis and its late effects | 134 (0.1%) | 124 (0.0%) | 111 (0.0%) | 83 (0.0%) | 74 (0.0%) | 63 (0.0%) |
| 018 Malignant tumour of the trachea, bronchi and lung 019 Other malignant tumours of the trachea, bronchi and lung | 16,935 (8.0%) | 16,615 (6.7%) | 16,772 (7.2%) | 5072 (2.5%) | 5303 (2.2%) | 5666 (2.6%) |
| 019 Other respiratory and intrathoracic malignancies | 332 (0.2%) | 359 (0.1%) | 316 (0.1%) | 152 (0.1%) | 143 (0.1%) | 160 (0.1%) |
| 062 Influenza (includes influenza due to identified pandemic or zoonotic influenza viruses) | 680 (0.3%) | 446 (0.2%) | 14 (0.0%) | 779 (0.4%) | 448 (0.2%) | 10 (0.0%) |
| 063 Pneumonia | 4837 (2.3%) | 4704 (1.9%) | 3831 (1.7%) | 4547 (2.2%) | 4064 (1.7%) | 2968 (1.4%) |
| 064 Chronic lower respiratory tract diseases (except asthma) | 9749 (4.6%) | 8832 (3.5%) | 7925 (3.4%) | 3066 (1.5%) | 2954 (1.2%) | 2569 (1.2%) |
| 065 Asthma | 158 (0.1%) | 212 (0.1%) | 175 (0.1%) | 835 (0.4%) | 736 (0.3%) | 626 (0.3%) |
| 066 Respiratory failure | 903 (0.4%) | 927 (0.4%) | 824 (0.4%) | 1268 (0.6%) | 1112 (0.5%) | 1125 (0.5%) |
| 067 Other diseases of the respiratory system | 9983 (4.7%) | 8714 (3.5%) | 7968 (3.4%) | 10,876 (5.3%) | 9274 (3.8%) | 7508 (3.4%) |
| TOTAL “Causes of death of the respiratory system” | 43,711 (20.6%) | 79,850 (32.0%) | 60,723 (26.2%) | 26,678 (12.9%) | 60,030 (24.6%) | 37,991 (17.3%) |
| 001-102 I-XXII.All Causes | 212,683 (30.7%) | 249,664 (36.0%) | 231,410 (33.4%) | 206,020 (30.8%) | 244,112 (36.5%) | 219,334 (32.8%) |
 due to diseases from the respiratory system, Spain, 2021.")
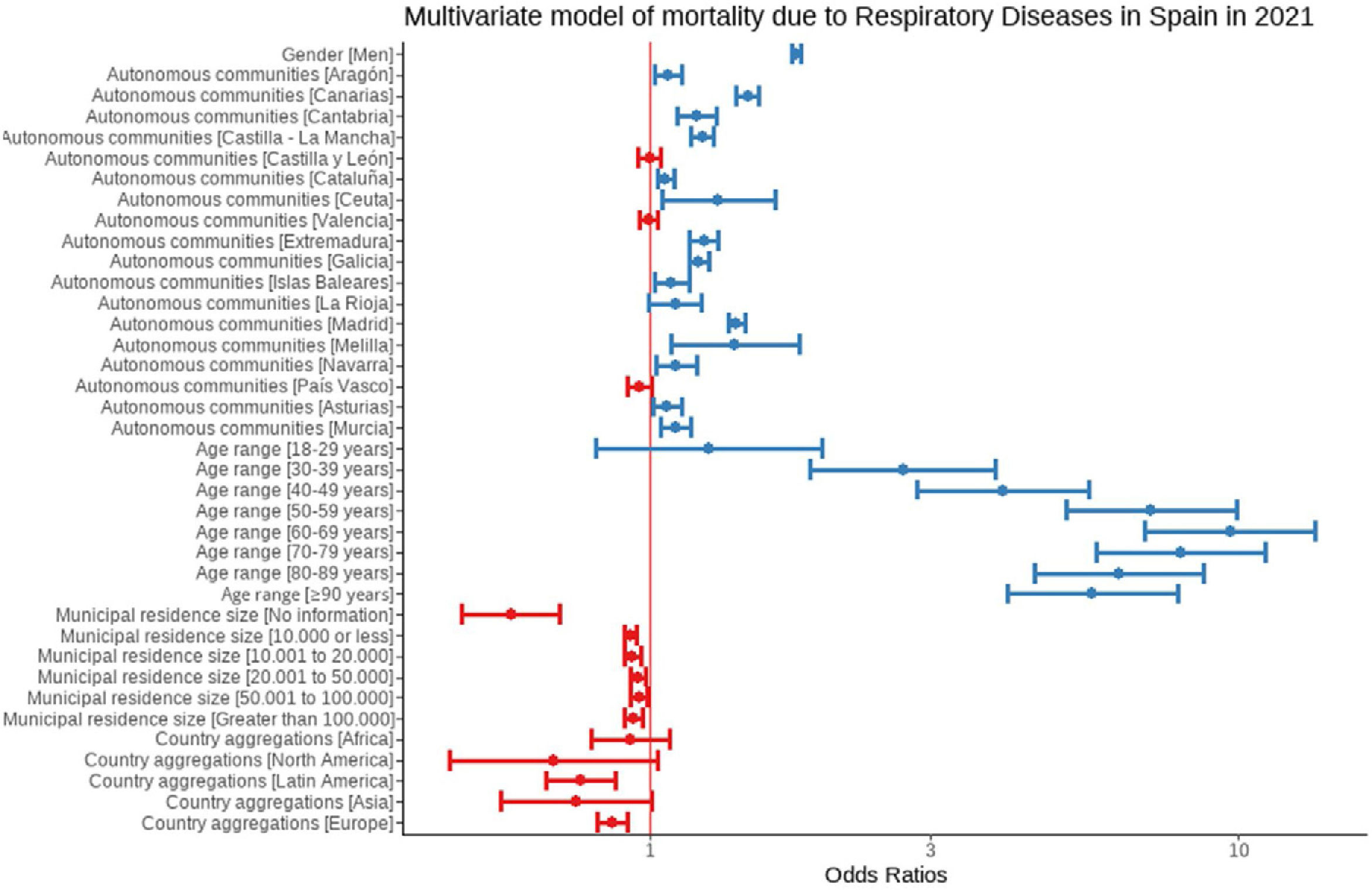
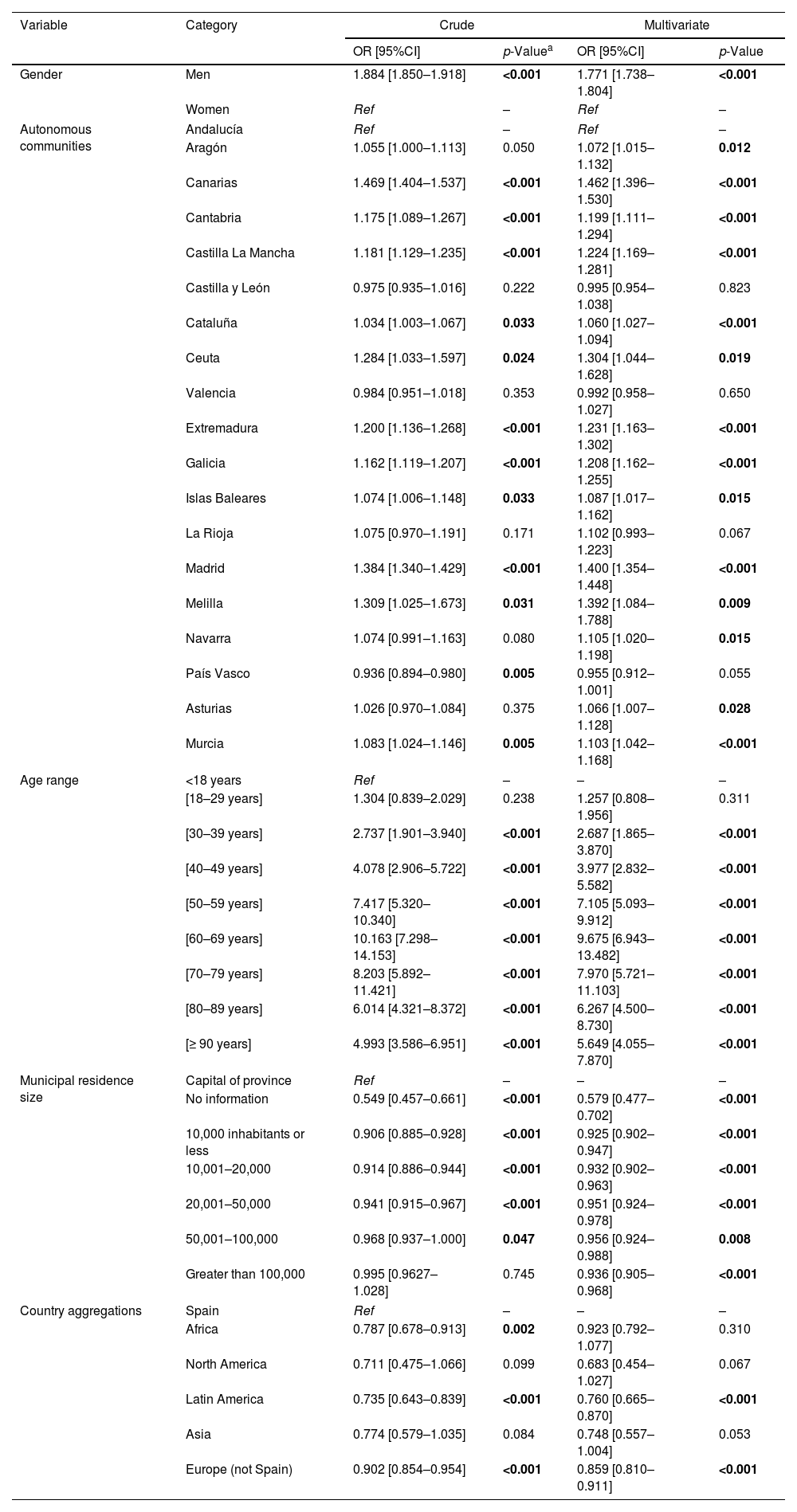
In the multivariate logistic regression analysis some established risk factors for respiratory diseases mortality were confirmed, such as male gender and older age; further, a protection in rural Spain was observed, still with a large geographical variability, and those born from elsewhere in Europe and LatinAmerica had significantly lower respiratory mortality compared to others born in any other continents (Table 4 and Fig. 2).
Crude and multivariate odds ratios for respiratory mortality (excluding COVID-19) in Spain in 2021.
| Variable | Category | Crude | Multivariate | ||
|---|---|---|---|---|---|
| OR [95%CI] | p-Valuea | OR [95%CI] | p-Value | ||
| Gender | Men | 1.884 [1.850–1.918] | <0.001 | 1.771 [1.738–1.804] | <0.001 |
| Women | Ref | – | Ref | – | |
| Autonomous communities | Andalucía | Ref | – | Ref | – |
| Aragón | 1.055 [1.000–1.113] | 0.050 | 1.072 [1.015–1.132] | 0.012 | |
| Canarias | 1.469 [1.404–1.537] | <0.001 | 1.462 [1.396–1.530] | <0.001 | |
| Cantabria | 1.175 [1.089–1.267] | <0.001 | 1.199 [1.111–1.294] | <0.001 | |
| Castilla La Mancha | 1.181 [1.129–1.235] | <0.001 | 1.224 [1.169–1.281] | <0.001 | |
| Castilla y León | 0.975 [0.935–1.016] | 0.222 | 0.995 [0.954–1.038] | 0.823 | |
| Cataluña | 1.034 [1.003–1.067] | 0.033 | 1.060 [1.027–1.094] | <0.001 | |
| Ceuta | 1.284 [1.033–1.597] | 0.024 | 1.304 [1.044–1.628] | 0.019 | |
| Valencia | 0.984 [0.951–1.018] | 0.353 | 0.992 [0.958–1.027] | 0.650 | |
| Extremadura | 1.200 [1.136–1.268] | <0.001 | 1.231 [1.163–1.302] | <0.001 | |
| Galicia | 1.162 [1.119–1.207] | <0.001 | 1.208 [1.162–1.255] | <0.001 | |
| Islas Baleares | 1.074 [1.006–1.148] | 0.033 | 1.087 [1.017–1.162] | 0.015 | |
| La Rioja | 1.075 [0.970–1.191] | 0.171 | 1.102 [0.993–1.223] | 0.067 | |
| Madrid | 1.384 [1.340–1.429] | <0.001 | 1.400 [1.354–1.448] | <0.001 | |
| Melilla | 1.309 [1.025–1.673] | 0.031 | 1.392 [1.084–1.788] | 0.009 | |
| Navarra | 1.074 [0.991–1.163] | 0.080 | 1.105 [1.020–1.198] | 0.015 | |
| País Vasco | 0.936 [0.894–0.980] | 0.005 | 0.955 [0.912–1.001] | 0.055 | |
| Asturias | 1.026 [0.970–1.084] | 0.375 | 1.066 [1.007–1.128] | 0.028 | |
| Murcia | 1.083 [1.024–1.146] | 0.005 | 1.103 [1.042–1.168] | <0.001 | |
| Age range | <18 years | Ref | – | – | – |
| [18–29 years] | 1.304 [0.839–2.029] | 0.238 | 1.257 [0.808–1.956] | 0.311 | |
| [30–39 years] | 2.737 [1.901–3.940] | <0.001 | 2.687 [1.865–3.870] | <0.001 | |
| [40–49 years] | 4.078 [2.906–5.722] | <0.001 | 3.977 [2.832–5.582] | <0.001 | |
| [50–59 years] | 7.417 [5.320–10.340] | <0.001 | 7.105 [5.093–9.912] | <0.001 | |
| [60–69 years] | 10.163 [7.298–14.153] | <0.001 | 9.675 [6.943–13.482] | <0.001 | |
| [70–79 years] | 8.203 [5.892–11.421] | <0.001 | 7.970 [5.721–11.103] | <0.001 | |
| [80–89 years] | 6.014 [4.321–8.372] | <0.001 | 6.267 [4.500–8.730] | <0.001 | |
| [≥ 90 years] | 4.993 [3.586–6.951] | <0.001 | 5.649 [4.055–7.870] | <0.001 | |
| Municipal residence size | Capital of province | Ref | – | – | – |
| No information | 0.549 [0.457–0.661] | <0.001 | 0.579 [0.477–0.702] | <0.001 | |
| 10,000 inhabitants or less | 0.906 [0.885–0.928] | <0.001 | 0.925 [0.902–0.947] | <0.001 | |
| 10,001–20,000 | 0.914 [0.886–0.944] | <0.001 | 0.932 [0.902–0.963] | <0.001 | |
| 20,001–50,000 | 0.941 [0.915–0.967] | <0.001 | 0.951 [0.924–0.978] | <0.001 | |
| 50,001–100,000 | 0.968 [0.937–1.000] | 0.047 | 0.956 [0.924–0.988] | 0.008 | |
| Greater than 100,000 | 0.995 [0.9627–1.028] | 0.745 | 0.936 [0.905–0.968] | <0.001 | |
| Country aggregations | Spain | Ref | – | – | – |
| Africa | 0.787 [0.678–0.913] | 0.002 | 0.923 [0.792–1.077] | 0.310 | |
| North America | 0.711 [0.475–1.066] | 0.099 | 0.683 [0.454–1.027] | 0.067 | |
| Latin America | 0.735 [0.643–0.839] | <0.001 | 0.760 [0.665–0.870] | <0.001 | |
| Asia | 0.774 [0.579–1.035] | 0.084 | 0.748 [0.557–1.004] | 0.053 | |
| Europe (not Spain) | 0.902 [0.854–0.954] | <0.001 | 0.859 [0.810–0.911] | <0.001 | |
CI: confidence interval.
 for Respiratory Diseases excluding COVID-19 in Spain in 2021.")
Finally, with an intention to be comprehensive in our descriptive analyses, the number of deaths and percentage of mortality by diseases of the respiratory system in 2021 in Spain are presented by Autonomous Community (eTable 1), and also by age (eTable 2).
DiscussionWe report that the COVID-19 pandemic has had a lasting impact on both general and specific causes of death due to respiratory diseases in 2021 in Spain, and it has disproportionately affected certain regions, mainly Madrid and Catalunya. By accounting COVID-19, tuberculosis and lung cancer deaths within the WHO list of diseases of the respiratory system, it can be stated that 21.9% of all deaths in 2021 in Spain were due to respiratory diseases, becoming second in the ranking of causes of death. Respiratory mortality in Spain has not returned to pre-pandemic levels in 2021, still with an increase of 30.3% compared to background rates in 2019.
Respiratory conditions are responsible for a large population burden of disease, morbidity and mortality, both in Spain and in the world. According to the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD), of the 50.5 million deaths that occurred in 1990 in the world, 4.3 million were attributed to pneumonia, 2.2 million to tuberculosis, 2.0 million to chronic obstructive pulmonary disease (COPD) and 0.95 million to lung cancer. In addition, it was estimated that for 2020, of the 68.3 million predictable deaths, 11.9 million would be from respiratory causes as per the standard WHO list, estimating that they became the third cause of death in 2020.12 In Spain, with a relatively aged population and yet with alarming rates of smoking,13 and of smoking-related deaths,14,15 respiratory diseases also have a huge impact on individual and population health.16,17 Its magnitude and diversity mean that the clinical management of respiratory health, beyond Pulmonology, also requires a large part of the daily dedication of health professionals in Primary Care, Internal Medicine and other specialties.18,19
It is well known that respiratory mortality statistics from death certificates are underreported compared to cancer, cardiovascular and metabolic diseases. This bias occurs for various reasons.20,21 Among other, it is a clinical challenge to attribute a death to a respiratory cause, since the symptoms and determinants are non-specific and overlap with those of cardiovascular or other diseases, and many patients with chronic respiratory diseases die with them and not from them.22,23 Current standardized coding manuals for death certificates from the World Health Organization (WHO), as well as from the European Union and its EUROSTAT, or from the National Institute of Statistics (INE) are homogeneous. The INE is governed by the rules established by the WHO as established by Regulation (EU) No. 328/2011 of the Commission of April 5, 2011, which applies Regulation (EC) No. 1338/2008 of the European Parliament and of the Council on Community statistics on public health and on health and safety at work. Regarding statistics on the causes of respiratory death, only those from Group VIII (with ICD10 062-067) are considered as causes of death of the Respiratory System, namely: Influenza; Pneumonia; Chronic diseases of the lower respiratory tract (except asthma); Asthma; Respiratory insufficiency; and Other diseases of the respiratory system.24 However, as above mentioned, other diseases that also directly affect the respiratory system such as tuberculosis, or daily practice in the field of Pulmonology and Thoracic Surgery such as lung cancer (“malignant tumours of the trachea, bronchi and lung”), are considered for statistical purposes as deaths of infectious and oncological causes, respectively, might be reconsidered as respiratory as well in future reclassifications.
This analysis has a number of strengths such as its immediacy, urgency, obvious relevance, and internal consistency. In addition, it contributes to the current debate on classifying by underlying cause vs. all basic death contributions. In particular, all INE Causes of Death Statistics offer data on the basic cause of death and also on all those other diseases that have contributed to death and that the certifying doctor has reported on the medical death certificate (multiple causes). All of them can be considered as advantages. However, we must highlight a series of limitations related with an observational study design, and some of which are inherent to the death certificate. In general, it is considered established that many patients with COPD, asthma or other respiratory diseases die with them as mentioned above.25,23
Explanatory factors are the general population's lack of knowledge about respiratory diseases and the lack of specificity of most respiratory symptoms and signs, compared to other major causes of disease and death, such as cardiovascular or oncological causes. This will require the design of complex long-term strategies, and therefore difficult to implement. However, overestimation should be avoided. Strictly speaking, the COVID-19 clinical care task of the pulmonologist could only be considered directly in deaths occurring in the hospital. For example, during the first wave in Spain, people who died in residences, or at their homes, did not represent a true care burden to pulmonologist. Of course, Pulmonology shares the treatment and management of respiratory patients with Internal Medicine, Primary Care and other specialties. Multisectoral coordination and dialogue should contribute to a better management of these patients.
Our findings suggest that, while proportionate mortality has largely returned to pre-pandemic levels overall, the pandemic has had a lasting impact on deaths due to respiratory diseases and certain specific causes of death, and has disproportionately affected certain regions. We conclude that respiratory mortality in Spain has not returned to pre-pandemic levels in 2021, still with an increase of 30.3% compared to background rates in 2019. Further research is needed to understand the factors contributing to these differences and to inform policies aimed at reducing respiratory diseases mortality in the post-pandemic era.
Ethical considerationsNot applicable as we only use administrative, anonymised official data.
FundingNone.
Conflict of interestThe authors declare there are no conflicts on interest to report related with this research.
EF is partially funded by the Department of Research and Universities of the Generalitat de Catalunya [2021SGR00906]. EF thanks IDIBELL for the institutional support of the CERCA/Generalitat de Catalunya Program.
The following are the supplementary data to this article:
