


Introduction
Recognition of the distinctive challenges in providing care to adolescents and young adults (AYA) with cancer has grown over the past 30 years in numerous countries, stimulated in particular by groups of advocates who have in turn raised awareness and philanthropic funding while harnessing sup¿ port from the cancer care community and agencies of fed¿ eral governments. Several examples stand out.
CanTeen (http://www.canteen.org.au) was founded in Australia in 1985 and has grown into a national organization providing support to young people with cancer through more than 250 programs across the country. In recent years it has received substantial funding support from the federal gov¿ ernment. This registered charity provides money for spe¿ cialist hospital care, counselling and individual assistance as well as information and peer support programs.
The Teenage Cancer Trust (TCT) (http://teenagecancer¿ trust.org/) began in the United Kingdom (UK) in 1990 and has built 25 facilities devoted to the care of those in this age group. It hosts biennial international workshops, most recently in July 2014, attracting participants from many countries. Prompted in part by this success, the National Institute for Health and Clinical Excellence in the UK has taken a position on “Improving Outcomes for Children and Young People with Cancer.”1
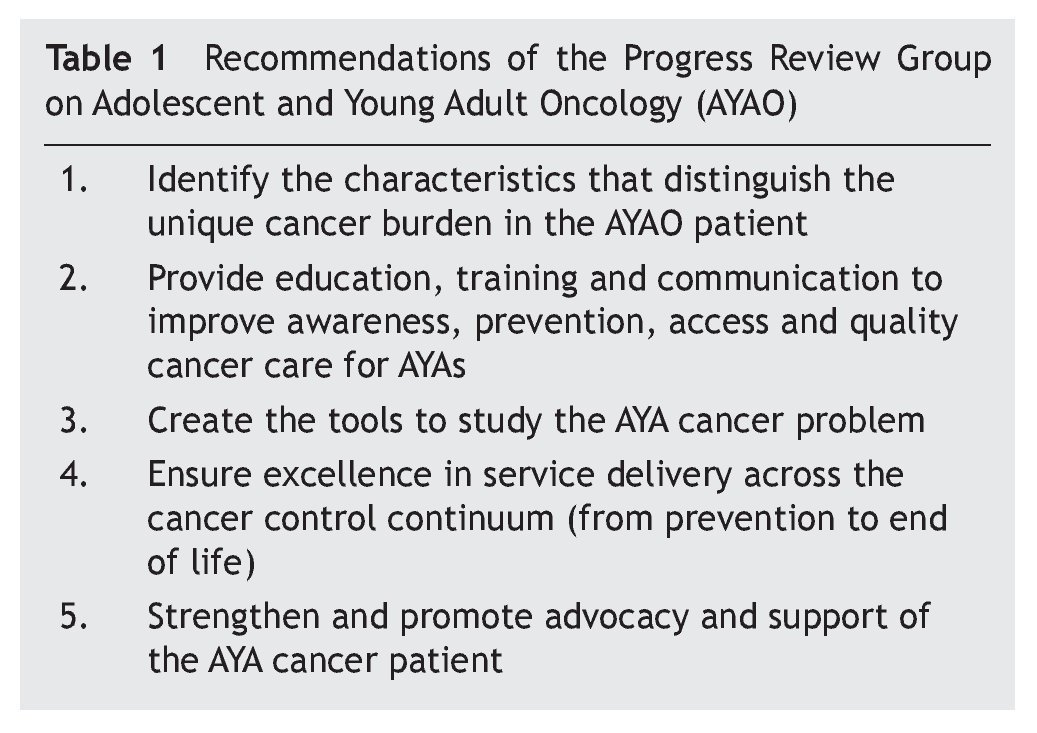
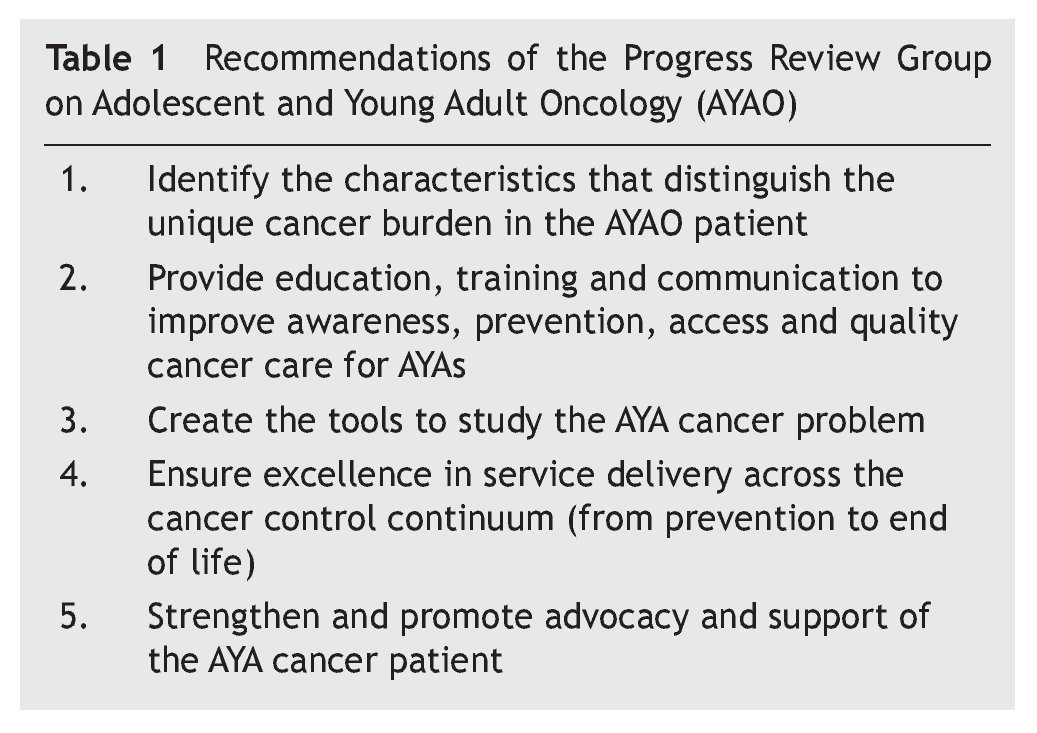
In the United States of America (USA), LiveStrong (then the Lance Armstrong Foundation that began in 1997) part¿ nered with the National Cancer Institute (NCI) to form a Progress Review Group (PRG) in 2005 that focused uniquely not on a disease but on a population, those in the age range of 15¿39 years.2 The PRG produced five recommendations (table 1) on which work continues to be undertaken. LiveStrong formed the Young Adult Cancer Alliance, a con¿ sortium of some 150 organizations that has gone on to inde¿ pendence as a new entity called Critical Mass.
A National Task Force on AYA with cancer was born in Can¿ ada in 2008 with support from C17, the network of all pediatric cancer programs, and funding provided by the Canadian Partnership Against Cancer, an agency of the fed¿ eral government. The Task Force has hosted biennial inter¿ national workshops3,4 and produced six recommendations to advance the discipline of AYA oncology.5 Among its other ac¿ complishments is the design of a national training program for oncologists as an Area of Focused Competence under the auspices of the Royal College of Physicians and Surgeons of Canada.
The clinical needs
A primary challenge is to define the age group that spans the conventional pediatric and adult health care systems, but does not fit well into either with respect to meeting the clinical needs of this population. Although the PRG in the USA adopted the age range of 15¿39, it is clear that the needs of teenagers are substantially different from those who are approaching middle age. Moreover, in industrialized countries the incidence of cancer rises substantially across the PRG-defined age span, from 200 per million in the 15-19 year age group to more than 1200 per million in the 35¿39 group. Accordingly a narrow age range has been used com¿ monly, e.g. 15¿25 for the evolution of specialized clinical services.6
Among the self-identified needs of this population is psy¿ cho¿social support as these young people wrestle with such challenges as changes in body image, sexuality, relation¿ ships with family and friends (including partners), return to education and employment, and financial stressors. A spe¿ cific requirement to be met is in fertility preservation7 that, in the cancer population, has become an emerging disci¿ pline (oncofertility)8 also.
A case has been made that accrual of AYA with cancer to therapeutic clinical trials has been especially deficient.9
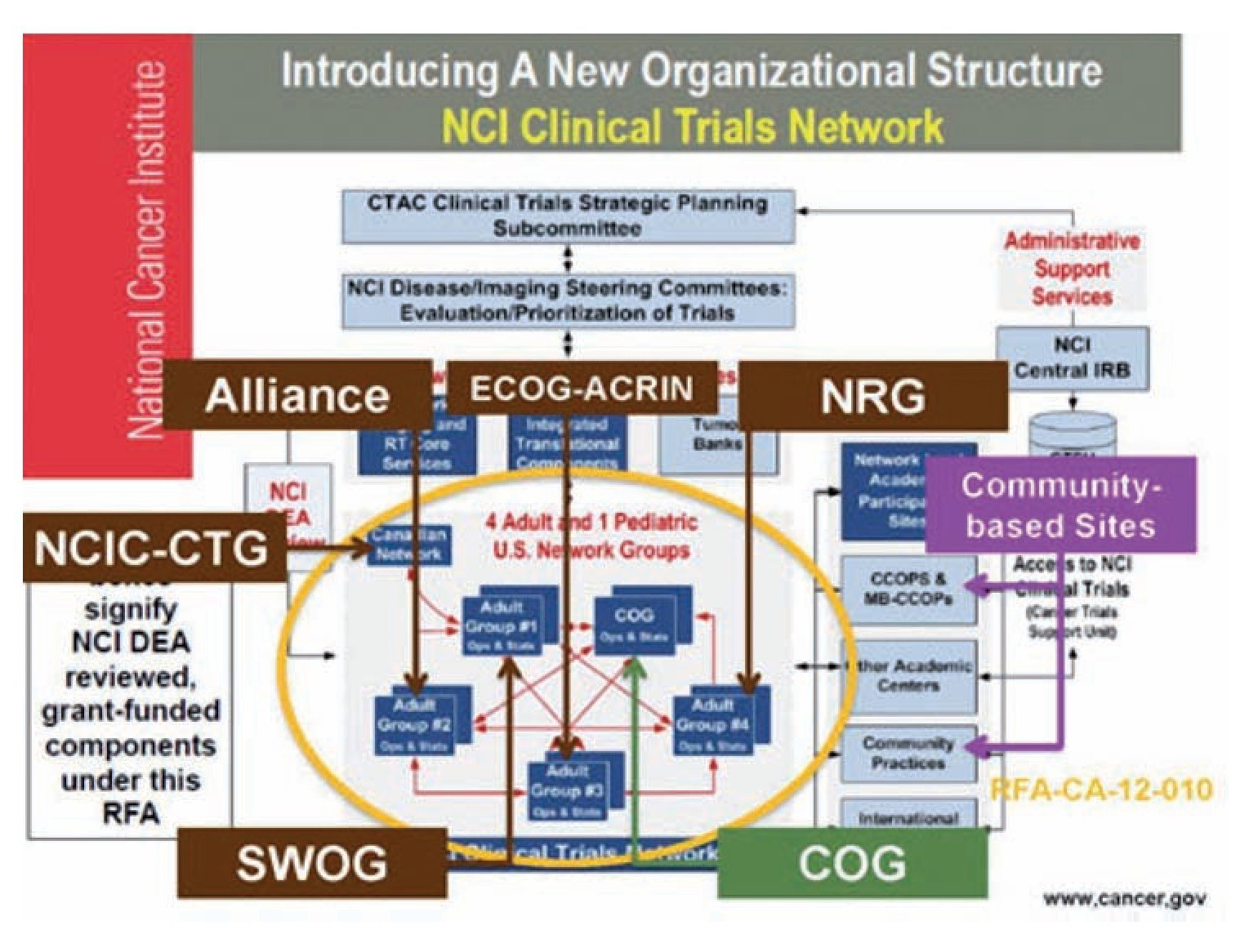
However, with the establishment of an AYA committee with¿ in the Children’s Oncology Group in 2000 there has been recent improvement in this regard and the formation of an intergroup focused on AYA in the re¿structured National Clin¿ ical Trials Network in North America (figure 1) should be a further stimulus to remedying the deficit. This initiative will be able to address the need for AYA specific clinical trials based on the evidence that, for some diseases (well exem¿ plified by acute lymphoblastic leukemia [ALL]) the outcome is better in young adults who are treated according to pedi¿ atric rather than adult protocols.10
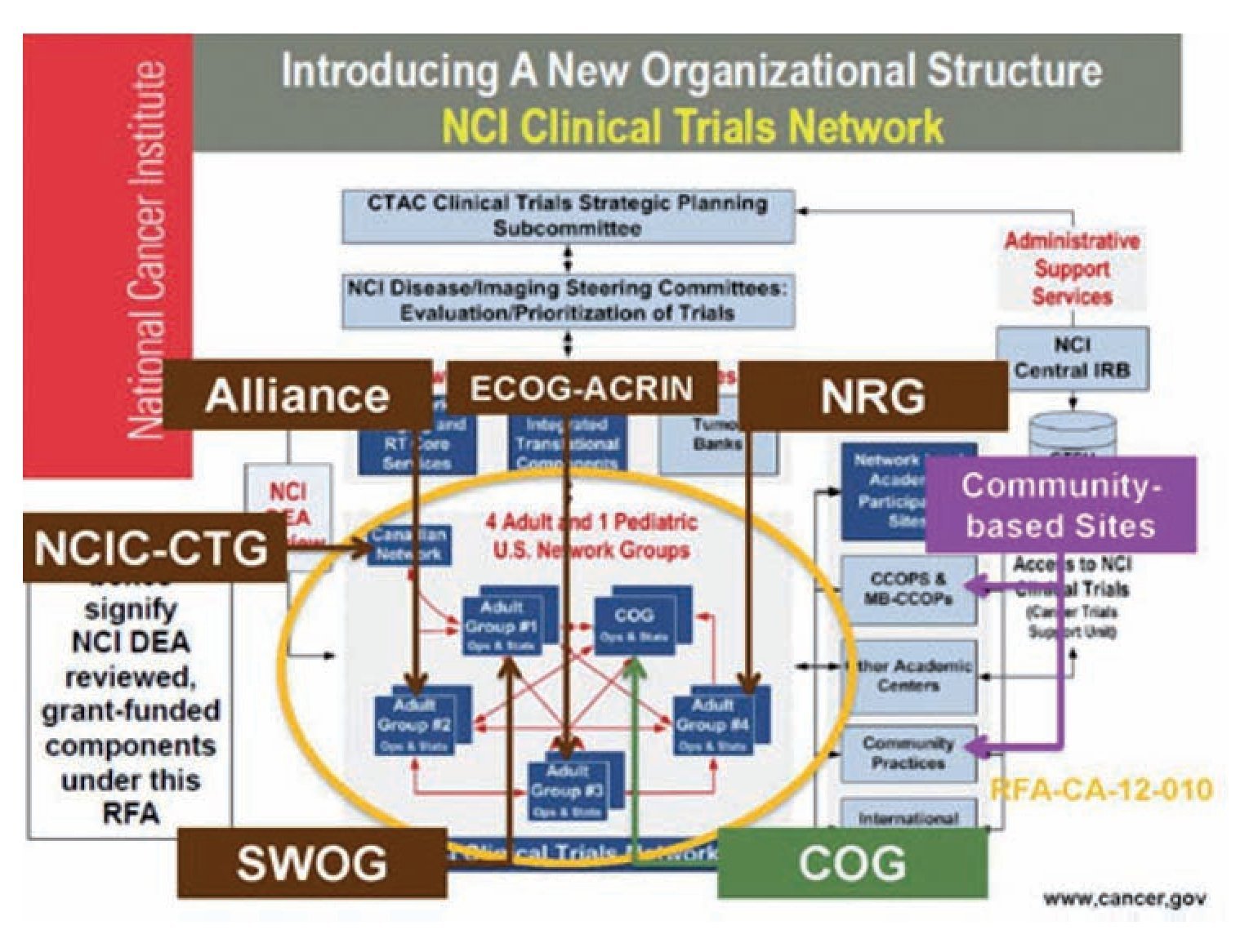
Figure 1 Re-configuration of the NCI Clinical Trials Network.
Disease distinctions
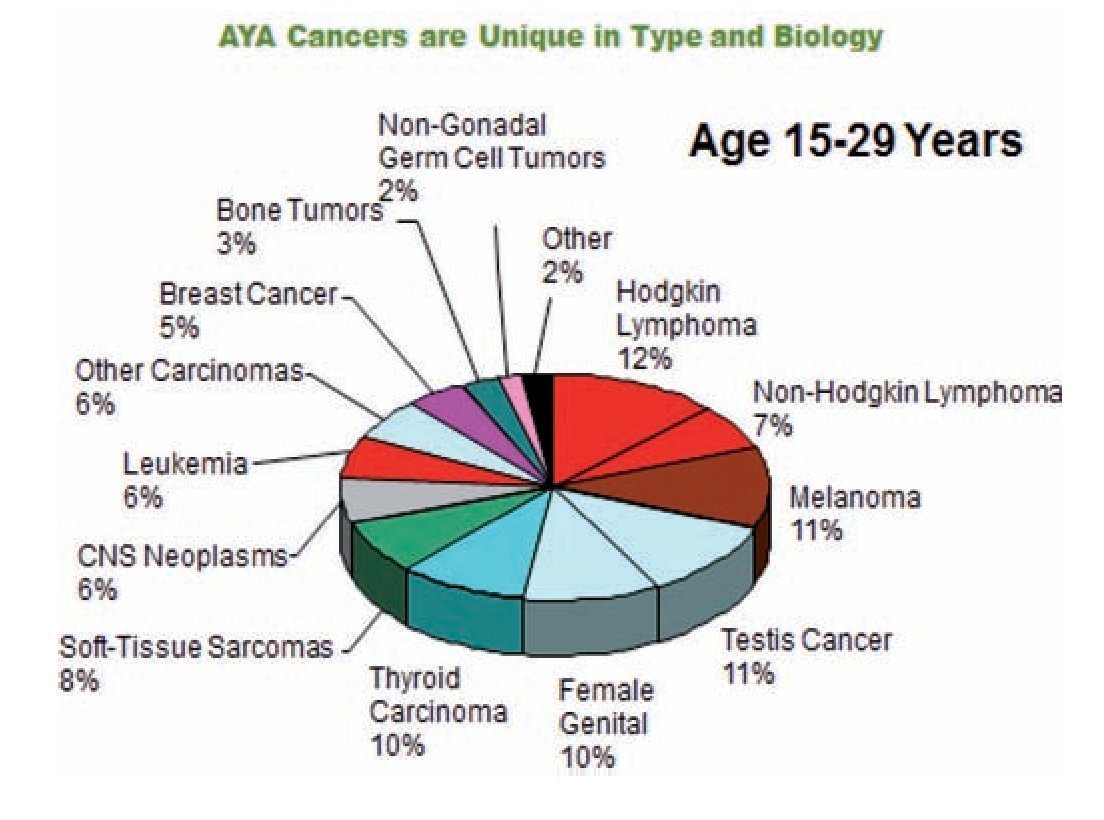
The spectrum of cancers affecting AYA is distinct from that affecting both younger and older people.11 Lymphomas, germ cell tumours, thyroid carcinomas and malignant mela¿ noma account for approximately 60% of the total in the age group of 15-29 years (figure 2). An appreciation of this dis¿ tinctiveness led to a proposed new classification of cancer in AYA12 that has been adopted by the Surveillance, Epidemi¿ ology and End Results Program of the NCI in the USA.
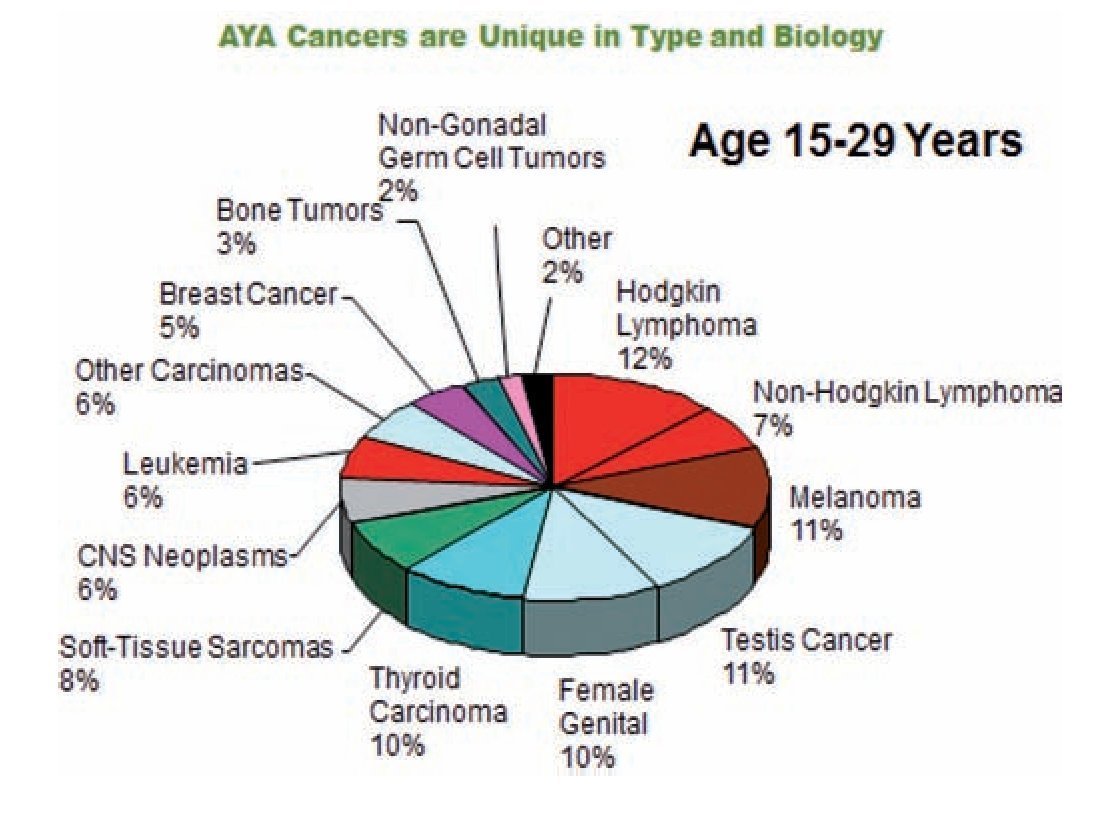
Figure 2 Disease distribution among adolescents and young adults (AYA) with cancer.
There is a growing understanding that the characteristics of individual diseases may also be different in AYA. This is true not only of ALL and solid tumours that are more common in childhood but also of some carcinomas, such as those of breast and colon, that are much more prevalent in older adults but do impact on AYA.13 These differences have impor¿ tant prognostic implications. Moreover, improved knowledge of the differences aid therapeutic decision¿making. For ex¿ ample, more female AYA than older women with breast can¿ cer have familial and “triple negative” disease (devoid of estrogen, progesterone and growth factor receptors). As fur¿ ther evidence of the distinctive phenotypes and genotypes of cancers in AYA become available, this opens avenues for more targeted therapy and better clinical outcomes.
Conclusions
It is hoped that this brief account of selected aspects of AYA oncology will serve, in some measure, to justify the emer¿ gence of this new discipline. More importantly, it may in¿ crease awareness of the special needs of AYA with cancer and attract a wide variety of health care professionals to form the multi¿disciplinary teams that are essential to the provision of optimal care to this population. Likewise, there are important questions to be addressed in both tumour and host biology. The growing interest in AYA oncology has spawned a new journal (Journal of Adolescent and Young Adult Oncology) and the first textbook devoted to the top¿ ic.14 Meanwhile the role of advocacy cannot be over¿esti¿ mated. A strong, well¿informed voice in support of AYA with cancer remains essential in harnessing the resources re¿ quired for the development and sustainability of clinical programs focused on the special needs of this population and for a robust, relevant research agenda.
Received: June 2014;
Accepted: June 2014
*Corresponding author:
E-mail address:rbarr@mcmaster.ca (R.D. Barr).