



Arterial hypertension is still a public health problem. Knowledge about the disease allows adequate management from prevention to treatment, and a better knowledge has also been associated with better adherence to the treatment.
ObjectiveTo determine factors associated with the level of knowledge about arterial hypertension in primary care patients.
Materials and methodsA non-experimental, cross-sectional, and analytical study was performed with a convenience sample using a structured survey to measure the level of knowledge about arterial hypertension. Frequency calculations and multivariate analysis were performed to determine the association between several factors with the level of knowledge, is considered statistically significant at p<0.05.
ResultsOf 188 participants, 68.09% were females, the average age was 45.37 years old, 35.11% had a diagnosis of arterial hypertension, and 68.09% had a family history of arterial hypertension. The level of knowledge was medium and was associated with age (p=0.01), previous diagnosis of hypertension (p=0.01) and a family history of hypertension (p=0.001). No association was found with genders, educational level or body mass index.
ConclusionsSome factors are associated with a greater knowledge about arterial hypertension, knowing them allows us to adapt public policies and educational interventions for patients who require it most.
According to the World Health Organization (WHO) arterial hypertension (HTN), is a public health problem that currently affects 40% of the worldwide population. The incidence of hypertension varies among different countries, the most affected ones are developing countries.1 In Venezuela, it is estimated that for every 100 people, 34 suffer from hypertension and more than 80% of those cases are not controlled.2,3 Its frequency increases with age, also observing that before 55 years, men are more likely to have high blood pressure, but after 55, women are more likely to have it than men. The most affected people are African descent, obese, those with a high consumption of sodium, people with low levels of physical activity, smokers and those with excessive alcohol intake.4,5
Hypertension usually does not present symptoms, which is why it often goes unnoticed, although occasionally headache, respiratory distress, dizziness, chest pain, palpitations or nosebleeds may be evident.1 Uncontrolled hypertension can lead to ventricular hypertrophy, myocardial infarctions, heart failure, hypertensive retinopathy, strokes and chronic renal failure.6 Among these complications, the highest percentage of deaths is due to coronary heart disease or heart failure.7
Although there are risk factors for HTN that cannot be modified, such as family history, gender, age and race, there are others that can, such as weight, physical activity level, alcohol intake, tobacco consumption, and diet.8 Knowledge of these factors is essential in the prevention, management, and control of HTN. Also, the patient must inform the health staff about complications and consequences arising from HTN, and in those who suffer from the disease, always remind them that it is a chronic disorder and the treatment is for life.3
Studies worldwide have reported deficiencies in the knowledge of hypertension in patients who suffer from it.9,10 However, no previous studies comparing knowledge between hypertensive and non-hypertensive patients were found. In addition, it is estimated that between 30 and 50% of hypertensive patients are unaware that they have the disease.11,12 People at risk of suffering HTN must be educated early and periodically assess their health status so that at the time of their diagnosis, they have a higher knowledge level and adhere better to therapeutic guidelines.
The present study aims to determine the factors associated with the level of knowledge about hypertension in primary care patients, both hypertensive and non-hypertensive, which is unknown in our population, and may be useful to guide educational campaigns to specific groups. In addition, to knowing the population's knowledge about the disease according to different parameters.
Materials and methodsA non-experimental, analytical, cross-sectional investigation was carried out through the application of an anonymous survey to patients who attended HTN screening in the “Simon Bolivar” and “Petra Emilia Moreno” Urban Outpatient Clinics of Bolivar City-Venezuela during December 2016.
The sample was non-probabilistic, including all the patients who attended the consultation in said health centers and wished to participate voluntarily in HTN screening. Of 225 patients who were attended, 188 (83.56%) were included in the study. Those who refused to participate in the study and who came for an emergency or with a clinical condition that prevented them from answering for themselves were excluded.
The survey was designed and validated (ad-hoc) by experts in public health. It consisted of 15 multiple choice questions, with a single correct answer, about general aspects of hypertension: normal blood pressure numbers, symptomatology, prevention, treatment, and complications. Prior to the application of the survey, sociodemographic information on the patients was collected: gender, age, education level, previous diagnosis of HTN and family history. A blood pressure measurement was carried out following the recommendations of the Venezuelan Society of Cardiology13 and was classified according to the Seventh Report of the Joint National Committee for the Prevention, Detection, Evaluation, and Treatment of Arterial Hypertension. Also, height and weight measurements were taken to calculate body mass index (BMI).
To measure the level of knowledge, a score from 0 to 10 was awarded based on the 15 questions. A score lower than five was considered a low level of knowledge, a score between 5 and 7was considered an average level of knowledge, and a score higher than 7 was considered a high level of knowledge.
The information was tabulated in Microsoft Excel 2013, and statistical analysis was performed with SPSS version 15 for Windows. To determine the association between gender, age, educational level, previous diagnosis of HTN, family history of HTN and BMI with the level of knowledge, a multivariate regression analysis was performed, considering a value of p<0.05 statistically significant.
Ethical considerations: Participation in the study was voluntary, with prior informed consent and information about the research that was carried out. The survey was delivered and collected by the authors, maintaining the anonymity of the participants at all times. Participation in the study did not represent any risk to the patient at any time.
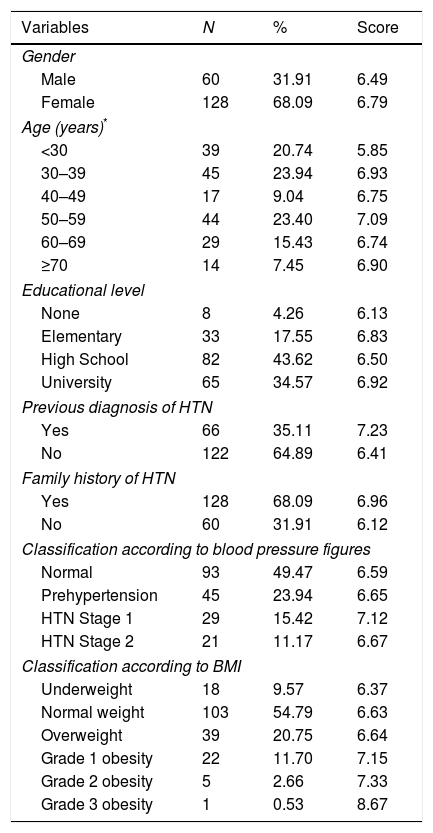
ResultsThe sample consisted of 188 individuals, of which 68.09% corresponded to the female sex. The average age was 45.37 years, and the most frequent age group was 30 to 39 years old (23.94%), followed by the group from 50 to 59 years old (23.40%). Of the participants, 78.19% had at least secondary education completed. 35.11%had already been diagnosed as hypertensive person, and 68.09% had a family history of hypertension (see Table 1). Of patients who had not been diagnosed as hypertensive, 13.93% had blood pressure numbers corresponding to stage 1 or 2 of hypertension. Of the sample, 86.17% recognized the normal blood pressure numbers correctly; 75.53% believed that HTN was preventable, and 53.13% said it was curable. The lowest percentages of correct answers corresponded to the questions about the symptoms; 87.77% erroneously indicated that the majority of people have headaches and 89.89% said they get dizziness. Regarding medication, 25% believed that treatment could be stopped if blood pressure was controlled and 19.15% believed that treatment could be discontinued if they felt better.
General characteristics of the studied population and level of knowledge about HTN.
| Variables | N | % | Score |
|---|---|---|---|
| Gender | |||
| Male | 60 | 31.91 | 6.49 |
| Female | 128 | 68.09 | 6.79 |
| Age (years)* | |||
| <30 | 39 | 20.74 | 5.85 |
| 30–39 | 45 | 23.94 | 6.93 |
| 40–49 | 17 | 9.04 | 6.75 |
| 50–59 | 44 | 23.40 | 7.09 |
| 60–69 | 29 | 15.43 | 6.74 |
| ≥70 | 14 | 7.45 | 6.90 |
| Educational level | |||
| None | 8 | 4.26 | 6.13 |
| Elementary | 33 | 17.55 | 6.83 |
| High School | 82 | 43.62 | 6.50 |
| University | 65 | 34.57 | 6.92 |
| Previous diagnosis of HTN | |||
| Yes | 66 | 35.11 | 7.23 |
| No | 122 | 64.89 | 6.41 |
| Family history of HTN | |||
| Yes | 128 | 68.09 | 6.96 |
| No | 60 | 31.91 | 6.12 |
| Classification according to blood pressure figures | |||
| Normal | 93 | 49.47 | 6.59 |
| Prehypertension | 45 | 23.94 | 6.65 |
| HTN Stage 1 | 29 | 15.42 | 7.12 |
| HTN Stage 2 | 21 | 11.17 | 6.67 |
| Classification according to BMI | |||
| Underweight | 18 | 9.57 | 6.37 |
| Normal weight | 103 | 54.79 | 6.63 |
| Overweight | 39 | 20.75 | 6.64 |
| Grade 1 obesity | 22 | 11.70 | 7.15 |
| Grade 2 obesity | 5 | 2.66 | 7.33 |
| Grade 3 obesity | 1 | 0.53 | 8.67 |
Source: author's own study.
HTN: arterial hypertension; BMI: body mass index.
Level of knowledge: low (score: <5), medium (score: 5–7), high (score: >7).
Prevention measures were correct for the majority; reduced salt intake (83.30%), weight loss (80.32%), physical activity (87.77%) and vegetable and fruit consumption (80.32%). When asked about the consequences of HTN, 96.28% guessed that high blood pressure increases the risk of heart attacks; this was the question with the highest percentage of correct answers. 89.89%correctlyresponded that HTN increases the risk of a stroke, but only 62.23% were able to answer that it increases the risk of blindness (see Fig. 1).

Regarding the level of knowledge, the average score was 6.69/10. The factors that were associated with the level of knowledge were age (p=0.01), a previous diagnosis of HTN (p=0.01) and a family history of hypertension (p=0.001). Gender, educational level, and BMI were not associated with the participants’ level of knowledge (p>0.05). Among individuals with a known diagnosis of hypertension, the time that had elapsed since their diagnosis was not associated with a higher level of knowledge about the disease (p>0.05).
DiscussionThe majority of the participants correctly identified blood pressure numbers that are considered as normal (86.17%), which is higher than results found in studies in Colombia and the United States (73% and 76%, respectively) in hypertensive patients.9,10 However, only half were correct in that HTN is not a curable disease, similar to that found by Barraza et al.9 All the same, a quarter of the respondents believed that they could stop treatment if blood pressure figures were controlled, and 19.15% believed that treatment could be discontinued if they felt better. Ignoring that HTN has no cure, could contribute to the progress of the disease if the patient assumes that after a while of following treatment, he could stop taking the medication. Thus, leading to a deterioration of their health; as highlighted by Granados and Gil,14 the lack of adherence to treatment for HTN results in failure to control and cope with the disease.
More than 80% of participants believe that hypertension shows symptoms in most people; in contrast, in most cases hypertension occurs asymptomatically, making diagnosis difficult.1 However, the presence of nonspecific symptoms could help detect it when the patient goes to a health center to assess their health status, which also represents a point of confusion for many patients, who could assume that these symptoms are a specific indicator of HTN.15
Headaches, dizziness, and nervousness are the main clinical manifestations that patients tend to associate erroneously with elevations in their blood pressure.
It is important to emphasize to patients that HTN does not have specific symptoms that allow it to be easily detected. When unnoticed, as Marin et al.,16 point out, it prevents many from complying with the prescribed therapeutic guidelines by mistakenly believing that not having symptoms means that they enjoy an optimal state of health.
About prevention measures, the majority agreed that reducing salt intake, losing weight, exercising regularly and increasing the consumption of fruits and vegetables helps reduce blood pressure figures, similar numbers as those found in the literature.9 The majority answered correctly about the consequences of maintaining high blood pressure levels, with myocardial infarction being the most successful among participants. Almost two-thirds were correct in that high blood pressure can cause blindness, and 30% in that hypertension does not increase the risk of lung cancer, a percentage similar to that of a study in Columbia and lower than that found in the United States (41.9%).10 According to studies carried out in Colombia, Spain, Brazil and the United States,9,10,17–19 most patients have some knowledge of HTN, but there is still considerable ignorance about it.
That is why the doctor must provide the relevant information and educate the patient about the disease so that the patient is aware of all the negative consequences that HTN can trigger in their bodies, and so that they understand the magnitude and severity of the problem, since the likelihood of an acute myocardial infarction is greater in those with uncontrolled hypertension.20
In a study in Turkey, it was found that knowledge about the duration of treatment, the reason for the use of medication, the cause of hypertension and knowing the blood pressure numbers were associated with a greater adherence to treatment,21 so patients should understand it as much as possible.
About the age range, the group under 30 years showed a lower level of knowledge than the rest. The higher the age, the higher the knowledge about the disease, a result similar to that reported in the literature,20 which may be due to the fact that older people go to health centers more often, and that the highest prevalence of hypertension is in older adults. Other studies have found a lower level of knowledge in patients over 60 years old.21
No relationship was found between sex or educational level and the knowledge about hypertension. However, in different studies, the female sex and a higher level of education have been associated with better knowledge about hypertension.11,18 BMI was also not associated with a higher level of knowledge; no previous studies were found that considered this relationship.
Patients with a prior diagnosis of hypertension showed a higher level of knowledge about the disease compared to those who had not been diagnosed or did not have it, although unlike other studies,12,18 the time since diagnosis in hypertensive patients was not associated with a higher level of knowledge about HTN (p>0.05). This may mean that health professionals are not giving the patient adequate information about their illness when they go for a consultation. Patients with a family history of hypertension showed a higher level of knowledge compared to the group with no history, similar to a study in Spain.12
It is noteworthy that in previous studies only the level of knowledge in people with a known diagnosis of HTN was measured. However, a large number of hypertensive patients do not know that they suffer from the disease1–3; proper knowledge about it before the diagnosis could improve efforts in prevention and adherence to treatment among this group of people, so it is suggested that we continue this line of research.
Although the sample does not allow inference about the rest of the population, the results are similar to those of other studies carried out in several countries, showing the need for continuingeducation of the patient and the establishment of follow-up programs in different primary care centers, which are the first gateway to the health system.
In conclusion, the level of knowledge about hypertension is medium in hypertensive and non-hypertensive individuals. There are factors associated with a higher levelofknowledge about arterial hypertension, knowing them allows for the adaption of public policies and educational interventions for the population that most requires it.
FundingNo financial support was provided.
Conflict of interestThe authors have no conflicts of interest to declare.
Previous presentationsNone.
To Christian Villanera, Claireth Rodríguez, Dhesiree Valor, Ara José, Yoselin Salas, Orlando Martínez, Cecilia Carvajal and Daniela Alcocer for their collaboration during the screening and data collection sessions for the present investigation.