



Low cerebrospinal fluid (CSF) pressure due to meningeal tear is an infrequent but widely reported condition, often associated with typical neuroimaging findings that are helpful for diagnosis. However, it is relatively infrequent for the site of the CSF leak to be located, especially in cases secondary to mild trauma; the upper thoracic spine and cervico-thoracic junction are the most frequent locations.1 Locating the site of the CSF leak is relevant due to the possible prognostic implications.
We present a case with striking neuroimaging findings, which enabled us to clearly locate the site of the CSF leak at the lumbar level (a rare location); this was essential to establish a definitive treatment.
Our patient was a 30-year old woman with no relevant personal history, who visited our department due to progressive headache of 48hours’ duration. Headache started 2hours after the patient lifted a 47-inch television set. The headache was frontal and drug-resistant, and was accompanied by nausea and vomiting. It improved only with bed rest and intensified when the patient stood. Physical examination revealed nuchal rigidity with positive Kernig and Brudzinski signs.
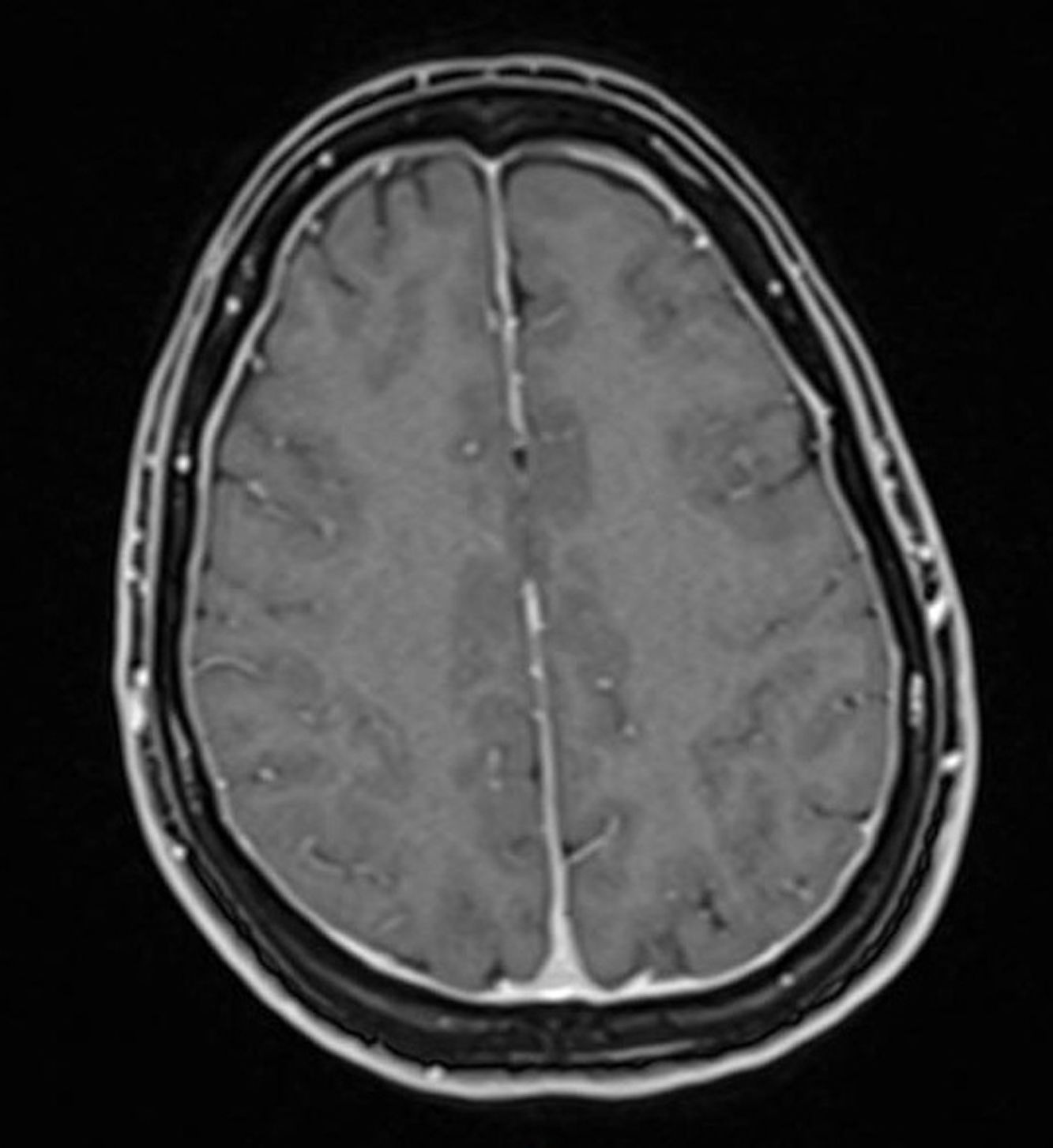
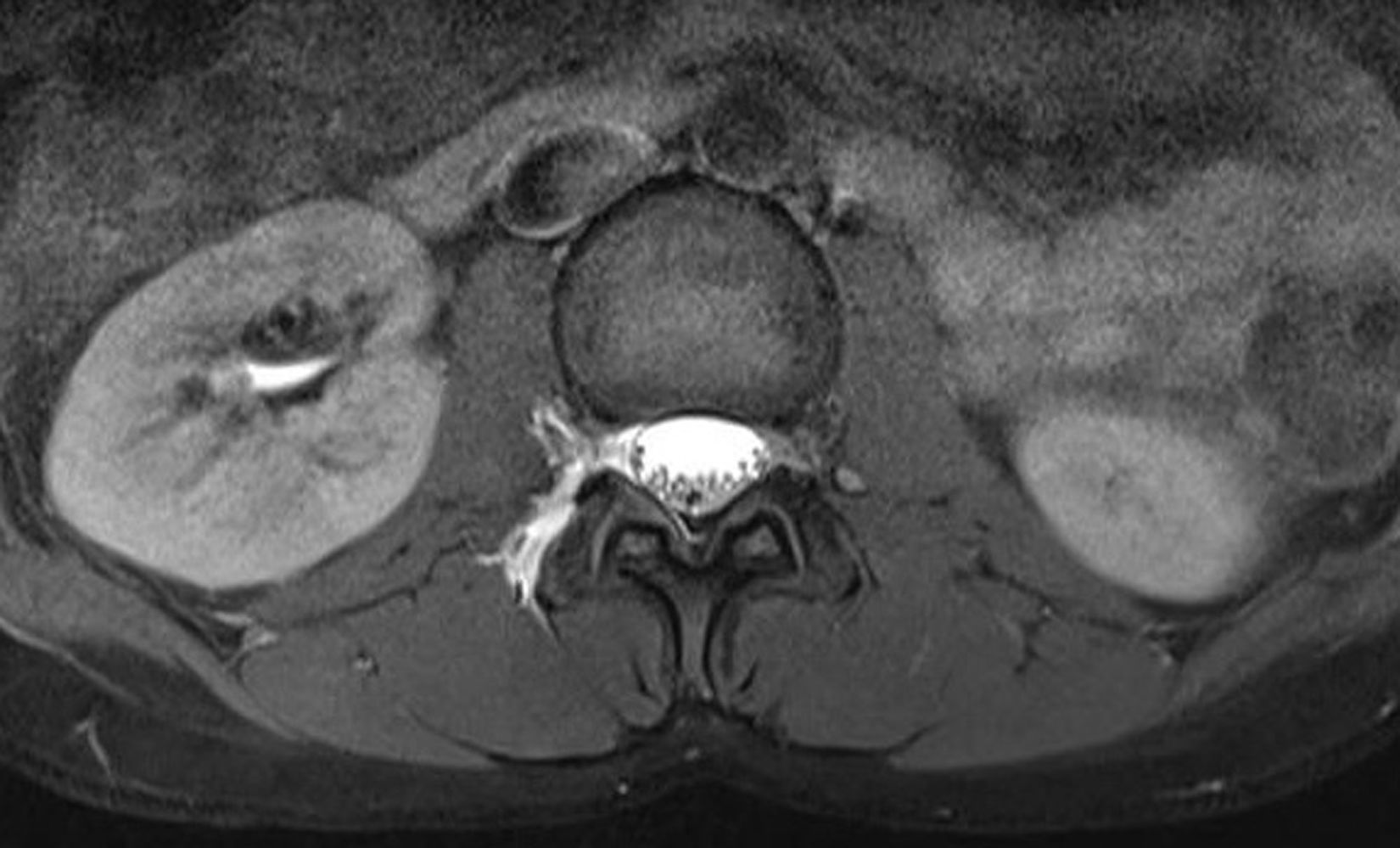
We suspected post-traumatic low CSF pressure headache, and the patient was admitted to the neurology department. A contrast-enhanced brain magnetic resonance imaging (MRI) scan only revealed generalised smooth dural enhancement (Fig. 1); a cervical, dorsal, and lumbar MRI with and without contrast showed no significant alterations; an MR myelography revealed an opening pressure of 1cm of water and bilateral extravasation of the contrast agent and CSF through the L1/L2, L2/L3, L3/L4, L4/L5 roots; this was compatible with CSF leak, possibly associated with rupture of the meningeal diverticula (Fig. 2).


These findings confirmed the diagnosis of low CSF pressure secondary to meningeal tear of the L1/L2, L2/L3, L3/L4, and L4/L5 roots of post-traumatic aetiology, associated with rupture of the meningeal diverticula.
As the site of CSF leak was located by MRI, symptoms could be controlled by placing an autologous blood patch at the site of the fistula.
Minor trauma has been described as a cause of CSF leaks,2 although the site is not always located. If this entity is not previously suspected, the diagnosis may be overlooked in these cases, given the apparent unimportance of the trauma.
The most frequent findings in contrast MRI3 are: (a) diffuse dural enhancement (the most frequent and characteristic) and pituitary enlargement caused by venous vasodilation compensating for the decreased CSF volume, leading to meningeal and pituitary gland congestion, and in turn, to increased contrast uptake4; and (b) presence of subdural fluid collections (intracranial and spinal). Intracranial collections are secondary to venous rupture after a decrease in CSF volume and downward displacement of the brain; spinal collections are mainly caused by the leakage and physical accumulation of CSF due to the effect of gravity,5 as in the case of our patient. In any case, rostrocaudal gradient and the presence of subdural collections are relatively infrequent.1,6
Locating the site of CSF leak is important because it may facilitate treatment with autologous blood patches at the site of the fistula, with the upper thoracic spine or cervico-thoracic junction being the most frequent locations, as mentioned previously.1
The interest of this case is the unusual location of the site of the CSF leak, and the neuroimaging findings, which clearly located the site of the CSF leak by showing the presence of a spinal subdural fluid collection and the extravasation of contrast agent at the level of the lumbar roots, which is a relatively infrequent occurrence.1
Please cite this article as: García Martín G, Rodríguez Belli AO, Padilla Parrado F, Aguilar Cuevas R. Localización del punto de fuga de líquido cefalorraquídeo en un caso de hipotensión de líquido cefalorraquídeo. Neurología. 2018;33:207–209.
