



The global prevalence of multiple sclerosis (MS) has increased in recent decades. However, there is a need for updated prevalence data for Spain.
ObjectiveTo analyze the prevalence of MS in Spain using data from the Primary Care Clinical Database (BDCAP, for its Spanish initials) and to compare the prevalence results in different autonomous communities (AC) according to sex in 2021.
MethodsThis cross-sectional study extracted data from the BDCAP on patients with MS according to sex, age, and place of residence in 2021. Crude prevalence rates were calculated, using the population assigned for each year of the study as the denominator. The geographic pattern of MS prevalence was analyzed using the following risk estimators: standardized prevalence ratio, smoothed relative risk (RR), and posterior probability of RR >1.
ResultsWe estimated 61753 cases of MS, with a crude estimated prevalence rate of 132.0 cases per 100000 person-years and a female/male ratio of 2.0. The age-standardized prevalence rate was 123.5 cases per 100000 person-years. Age-specific prevalence rates were lower in men than in women. All indicators showed a north-south gradient. Seven ACs for women and 5 ACs for men showed a significant excess risk (primarily in the north of Spain), whereas 8 ACs for both women and men presented lower risk (mainly in the south).
ConclusionsOur results provide the most recent prevalence data for MS and the geographic patterns at the ACs level in Spain, revealing a north-south gradient. Our results pave the way for future strategies to manage the impact of MS in Spain and to understand causal hypotheses.
La prevalencia mundial de la esclerosis múltiple (EM) se ha incrementado en las últimas décadas. Sin embargo, los datos de prevalencia en España necesitan ser actualizados.
ObjetivoAnalizar la prevalencia española de EM a partir de datos de la Base de Datos Clínica de Atención Primaria (BDCAP) y comparar los resultados de prevalencia entre comunidades autónomas (CA) según sexo durante 2021.
MétodosEste estudio transversal extrajo los datos del BDCAP de casos de EM según sexo, edad y lugar de residencia en 2021. Calculamos las tasas de prevalencia brutas utilizando como denominador la población asignada a cada año de estudio. El patrón espacial de prevalencia de EM se analizó utilizando como estimadores de riesgo la razón de prevalencia estandarizada (SPR), el riesgo relativo (RR) suavizado y la probabilidad posterior (PP) de RR>1.
ResultadosSe estimaron 61.753 casos de EM, con una tasa de prevalencia bruta de 132,0 por 100.000 personas-año y una relación mujer/hombre de 2,0. La tasa de prevalencia estandarizada por edad fue de 123,5 por 100.000 años-persona. Las tasas de prevalencia específicas por edad fueron más bajas en los hombres que en las mujeres. Todos los indicadores mostraron un patrón norte-sur. En mujeres siete CA y cinco CA en hombres mostraron un exceso de riesgo significativo (principalmente en el norte de España), mientras que ocho CA en mujeres y hombres registraron un menor riesgo (principalmente en el sur).
ConclusionesNuestros resultados proporcionan los datos de prevalencia más recientes para la EM, así como los patrones espaciales a nivel de CA en España, registrándose un gradiente norte-sur. Nuestros resultados allanan el camino para futuras estrategias de gestión respecto al impacto de la EM en España, y comprender hipótesis causales.
Multiple sclerosis (MS) is an inflammatory, degenerative disorder of the central nervous system that affects approximately 2.8 million people worldwide.1 In recent decades, new technological developments, updates in diagnostic criteria, increased access to specialized healthcare, and the widespread use of disease-modifying therapies (DMT) have contributed to improving the understanding and diagnosis of MS.2,3
The prevalence of MS appears to have increased in recent decades, probably as a combined result of earlier identification and diagnosis, better disease treatment, and longer life expectancy. However, MS incidence trends over time seem to be somewhat less clear.
The variation in MS incidence and prevalence rates by geographic region is well described, with rates tending to be higher farther from the equator.4 Systematic reviews have estimated MS incidence and prevalence rates in different geographical areas and compared results between countries and regions, as well as changes in rates over time by area and globally.2,5–10
In Spain, in recent decades, there has been an increase in the incidence and prevalence of MS in various regions of the country.11 To our knowledge, no background literature assesses the prevalence rates of MS in Spain as a whole. The Primary Care Clinical Database (BDCAP, for its Spanish initials) of the National Health System was developed for statistical and research purposes, with the consensus of all autonomous communities (AC) and the National Institute of Health Management.12 This database collects annual standardized clinical information from the primary care level, based on a large random sample of clinical records in the population assigned to this level of care. These data are representative at the AC level and have been used to analyze some health problems in the country, including MS.13–18
Taking into account the detected gaps and the previous information, we set out to analyze Spanish MS prevalence rates in 2021. An additional objective is to examine the differences between regions, and the characteristics of people diagnosed with MS in terms of age, sex, and AC of residence using the information available in the BDCAP.
MethodsTo calculate prevalence, data on the sex, age, and place of residence of patients with MS (identified with ICPC-2 code N86) were extracted from the BDCAP. The term prevalence refers to the total number of cases of MS in Spain that remained active during 2021 in the database.
This cross-sectional study was conducted in accordance with the Declaration of Helsinki and STROBE statements; ethical approval was not required due to the study design and source of data.
We calculated crude prevalence rates using the population assigned each year of the study as the denominator.19 To facilitate comparison with other European countries, national prevalence rates were adjusted for the European Standard Population of 2013, in 5-year age intervals, using the direct method.20
To examine the geographic pattern of MS prevalence, risk was estimated with the standardized prevalence ratio (SPR), the smoothed relative risk (RR), and the posterior probability (PP) of RR >1. The indirect method of standardization was performed to compare the data for each AC against the national average. To do this, we calculated the expected cases in each AC by applying age- and sex-specific rates at the national level to the different populations by age and sex at the AC level. Once the expected cases were obtained, we calculated the SPR, which measures the RR with respect to the reference region (Spain). To this end, we used the number of observed cases (O) as the numerator and the number of expected cases (E) as the denominator. Since SPRs are highly variable when analyzing diseases with few cases or in areas with small populations, we modeled risk by taking into account information from spatial neighbors. This model is based on fitting a Poisson spatial model with observed cases as the dependent variable, log-expected cases as offset, and two types of random-effects terms which take into account the following: (I) contiguity (spatial autocorrelation term) and (II) nonspatial heterogeneity. Model fitting and inference were performed using the approximate Bayesian inference technique called INLA (integrated nested Laplace approximation) in the free software program R, using the R-INLA package.21,22
Additionally, we calculated an absolute risk measure, defined as the difference between observed and expected cases (DOE). DOE is a similar indicator to the SPR mentioned above, but might be more directly useful for health management aspects because it is expressed as the number of potentially preventable cases.
The GeoDa software23 was used to generated the maps illustrating the geographical distribution of MS prevalence in Spain. To facilitate visualization of the maps, the Canary Islands were moved closer to the mainland.
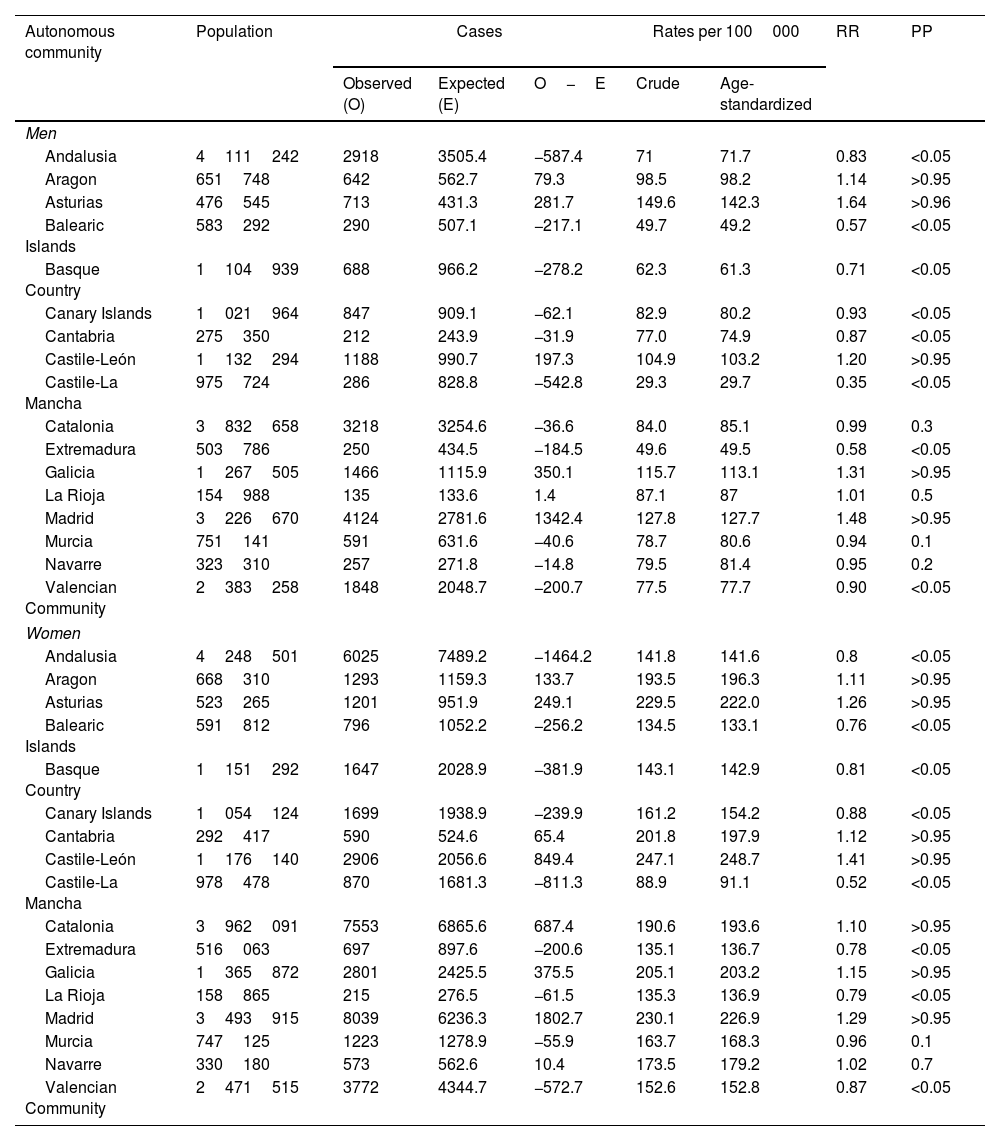
ResultsTable 1 shows the following data for each AC and sex: population assigned to primary care, MS cases (observed and expected), crude and age-standardized prevalence rates per 100000 person-years (indirect method), the RR and the PP of RR >1 in Spain. For 2021, we estimate a total of 61573 cases of MS in Spain (19673 men and 41900 women) (Table 1). This represents 0.13% of the population assigned to the primary care level within the National Health System that year. The assigned population in 2021 was 46655391, representing 98.6% of the resident population in Spain, according to the National Institute of Statistics.24 The crude estimated prevalence rate was 132.0 cases per 100000 person-years (86.1 in men and 176.0 in women), with a female/male ratio of 2.0. The standardized prevalence rate was 123.5 per 100000 person-years (165.8 in women and 80.1 in men), with a female/male ratio of 2.1.
Population, cases of multiple sclerosis (observed and expected), crude and age-standardized prevalence rates per 100000 person-years, smoothed relative risk (RR), and the posterior probability (PP) of RR >1, by sex and autonomous community. Spain 2021.
| Autonomous community | Population | Cases | Rates per 100000 | RR | PP | |||
|---|---|---|---|---|---|---|---|---|
| Observed (O) | Expected (E) | O−E | Crude | Age-standardized | ||||
| Men | ||||||||
| Andalusia | 4111242 | 2918 | 3505.4 | −587.4 | 71 | 71.7 | 0.83 | <0.05 |
| Aragon | 651748 | 642 | 562.7 | 79.3 | 98.5 | 98.2 | 1.14 | >0.95 |
| Asturias | 476545 | 713 | 431.3 | 281.7 | 149.6 | 142.3 | 1.64 | >0.96 |
| Balearic Islands | 583292 | 290 | 507.1 | −217.1 | 49.7 | 49.2 | 0.57 | <0.05 |
| Basque Country | 1104939 | 688 | 966.2 | −278.2 | 62.3 | 61.3 | 0.71 | <0.05 |
| Canary Islands | 1021964 | 847 | 909.1 | −62.1 | 82.9 | 80.2 | 0.93 | <0.05 |
| Cantabria | 275350 | 212 | 243.9 | −31.9 | 77.0 | 74.9 | 0.87 | <0.05 |
| Castile-León | 1132294 | 1188 | 990.7 | 197.3 | 104.9 | 103.2 | 1.20 | >0.95 |
| Castile-La Mancha | 975724 | 286 | 828.8 | −542.8 | 29.3 | 29.7 | 0.35 | <0.05 |
| Catalonia | 3832658 | 3218 | 3254.6 | −36.6 | 84.0 | 85.1 | 0.99 | 0.3 |
| Extremadura | 503786 | 250 | 434.5 | −184.5 | 49.6 | 49.5 | 0.58 | <0.05 |
| Galicia | 1267505 | 1466 | 1115.9 | 350.1 | 115.7 | 113.1 | 1.31 | >0.95 |
| La Rioja | 154988 | 135 | 133.6 | 1.4 | 87.1 | 87 | 1.01 | 0.5 |
| Madrid | 3226670 | 4124 | 2781.6 | 1342.4 | 127.8 | 127.7 | 1.48 | >0.95 |
| Murcia | 751141 | 591 | 631.6 | −40.6 | 78.7 | 80.6 | 0.94 | 0.1 |
| Navarre | 323310 | 257 | 271.8 | −14.8 | 79.5 | 81.4 | 0.95 | 0.2 |
| Valencian Community | 2383258 | 1848 | 2048.7 | −200.7 | 77.5 | 77.7 | 0.90 | <0.05 |
| Women | ||||||||
| Andalusia | 4248501 | 6025 | 7489.2 | −1464.2 | 141.8 | 141.6 | 0.8 | <0.05 |
| Aragon | 668310 | 1293 | 1159.3 | 133.7 | 193.5 | 196.3 | 1.11 | >0.95 |
| Asturias | 523265 | 1201 | 951.9 | 249.1 | 229.5 | 222.0 | 1.26 | >0.95 |
| Balearic Islands | 591812 | 796 | 1052.2 | −256.2 | 134.5 | 133.1 | 0.76 | <0.05 |
| Basque Country | 1151292 | 1647 | 2028.9 | −381.9 | 143.1 | 142.9 | 0.81 | <0.05 |
| Canary Islands | 1054124 | 1699 | 1938.9 | −239.9 | 161.2 | 154.2 | 0.88 | <0.05 |
| Cantabria | 292417 | 590 | 524.6 | 65.4 | 201.8 | 197.9 | 1.12 | >0.95 |
| Castile-León | 1176140 | 2906 | 2056.6 | 849.4 | 247.1 | 248.7 | 1.41 | >0.95 |
| Castile-La Mancha | 978478 | 870 | 1681.3 | −811.3 | 88.9 | 91.1 | 0.52 | <0.05 |
| Catalonia | 3962091 | 7553 | 6865.6 | 687.4 | 190.6 | 193.6 | 1.10 | >0.95 |
| Extremadura | 516063 | 697 | 897.6 | −200.6 | 135.1 | 136.7 | 0.78 | <0.05 |
| Galicia | 1365872 | 2801 | 2425.5 | 375.5 | 205.1 | 203.2 | 1.15 | >0.95 |
| La Rioja | 158865 | 215 | 276.5 | −61.5 | 135.3 | 136.9 | 0.79 | <0.05 |
| Madrid | 3493915 | 8039 | 6236.3 | 1802.7 | 230.1 | 226.9 | 1.29 | >0.95 |
| Murcia | 747125 | 1223 | 1278.9 | −55.9 | 163.7 | 168.3 | 0.96 | 0.1 |
| Navarre | 330180 | 573 | 562.6 | 10.4 | 173.5 | 179.2 | 1.02 | 0.7 |
| Valencian Community | 2471515 | 3772 | 4344.7 | −572.7 | 152.6 | 152.8 | 0.87 | <0.05 |
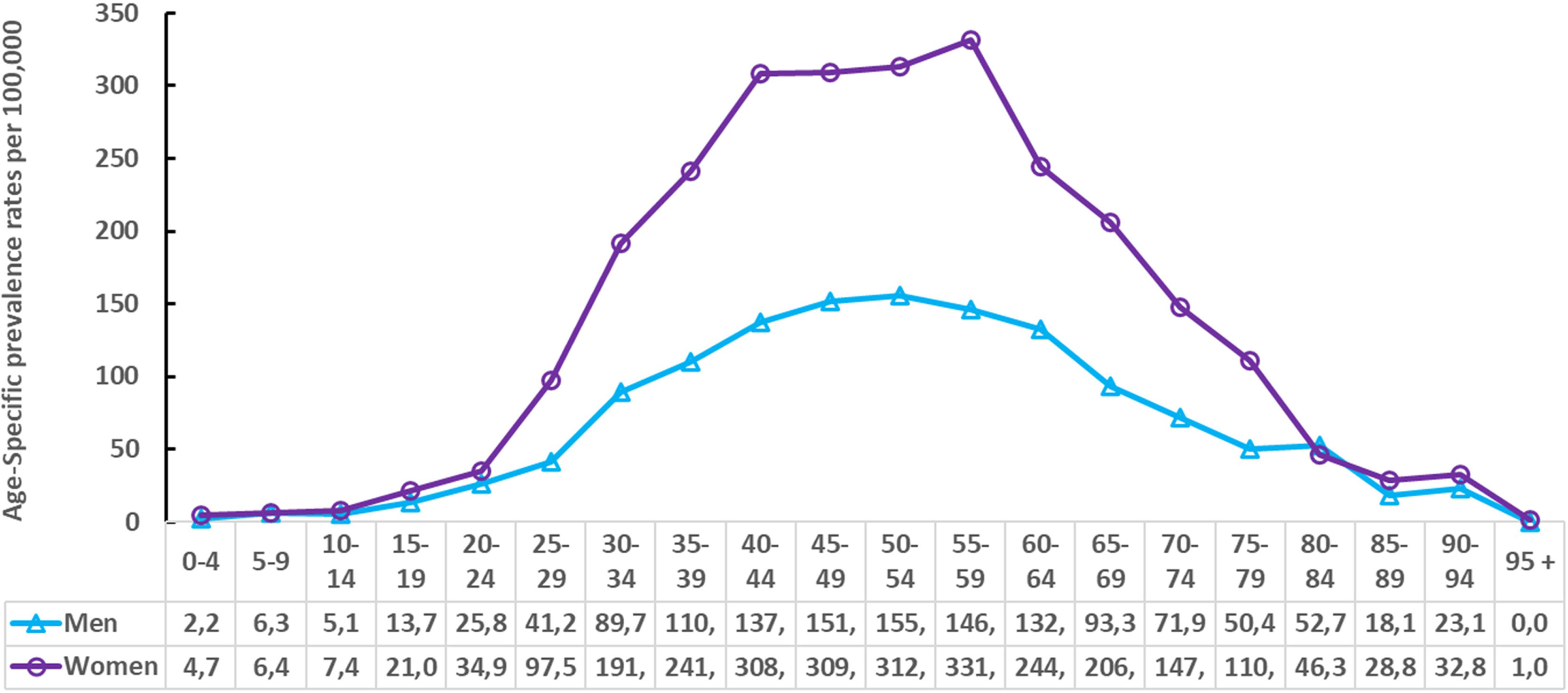
Fig. 1 shows the age- and sex-specific prevalence rates in the Spanish population assigned to the primary care level used to estimate the expected cases in each AC. In all age groups, men presented lower rates than women, except for the 80–84 age group.
.")
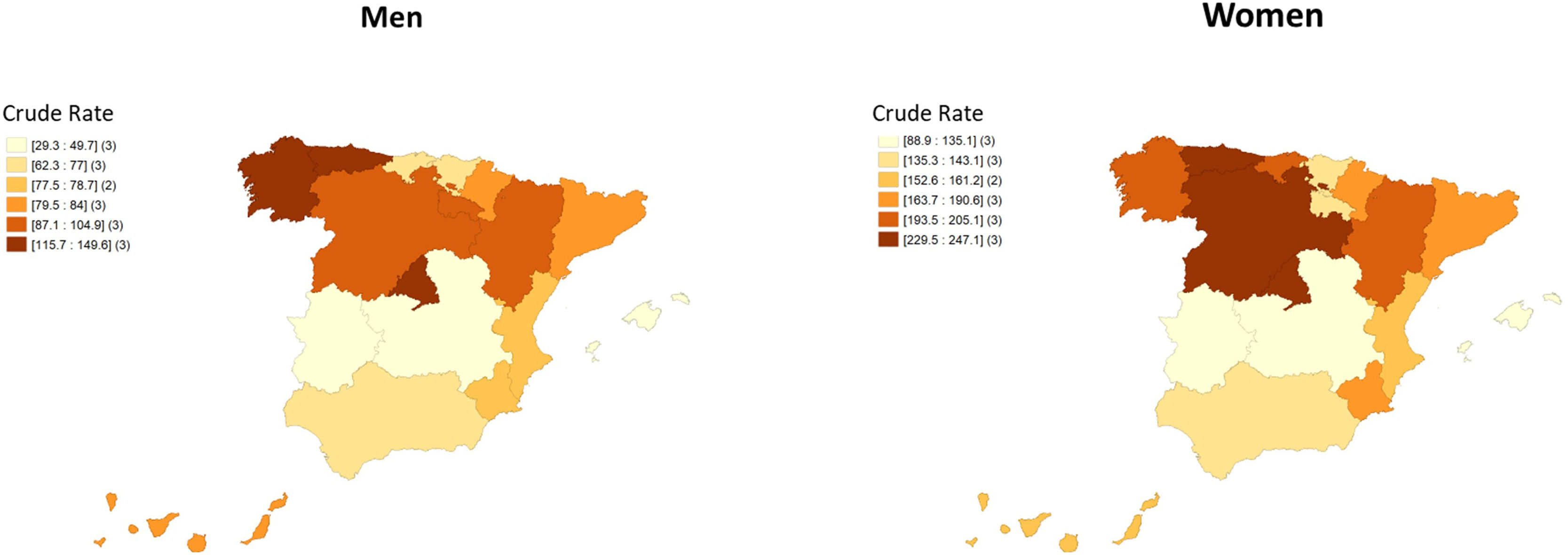
Fig. 2 shows the crude prevalence rates per 100000 person-years by sex. In both cases, a north-south gradient was observed, with the rates being higher in the north and lower in the south. Men presented lower rates than women in all ACs. The female/male ratio ranged from 1.5 in Asturias to 3.0 in Castile-La Mancha.

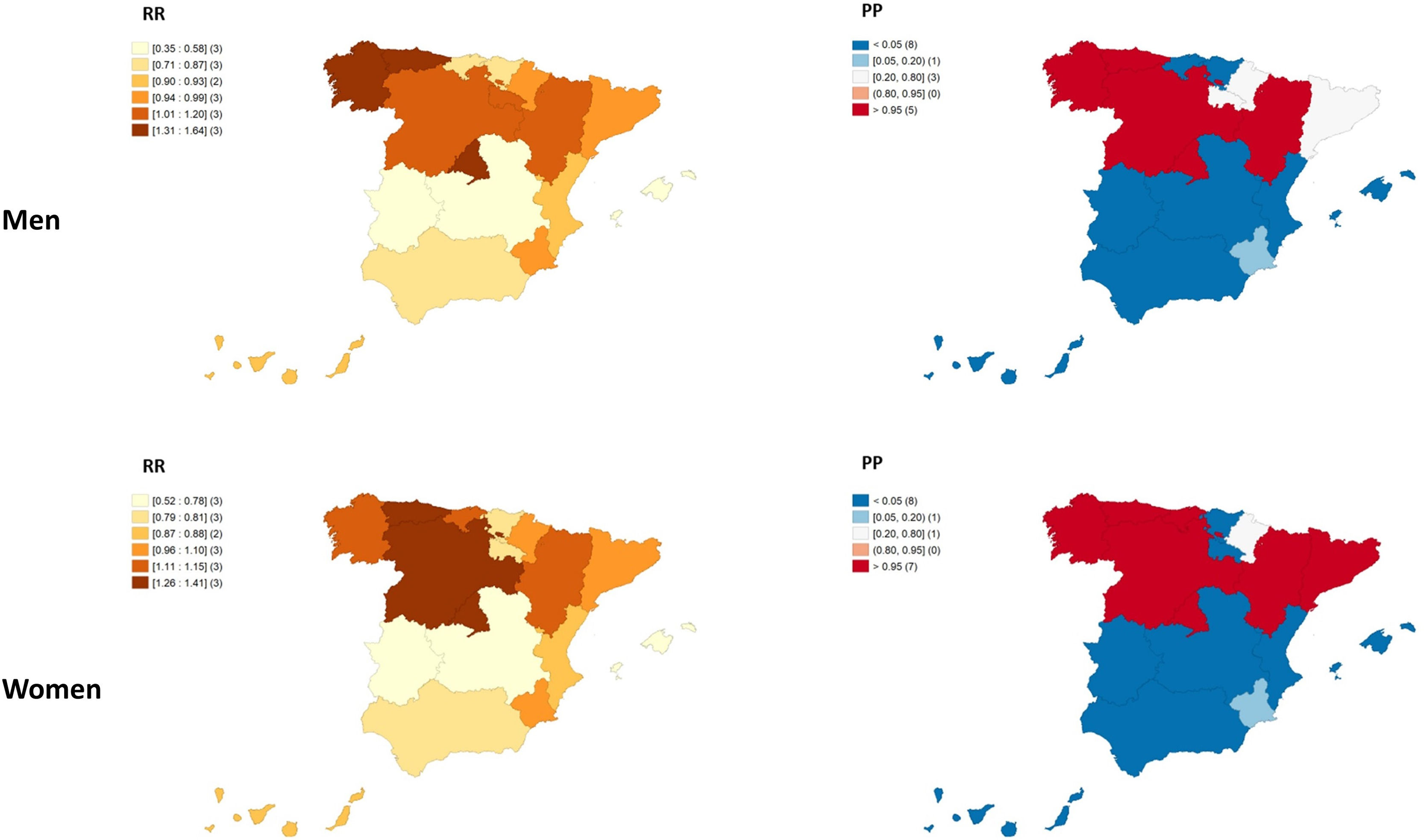
Fig. 3 shows the RR and PP of RR >1 for men and women in each AC. As in crude rates, a north-south gradient was detected, with higher and significant RRs in the north and lower and significant RRs in the south. In women, 7 ACs showed a significant excess risk and 8 ACs showed a significantly lower risk; all were located in the south, except the Basque Country and Navarre in the north. In men, we recorded a similar pattern as in women, with 5 northern ACs showing excess risk and 8 ACs showing minor risk (all located in the south, except the Basque Country and Cantabria in the north).

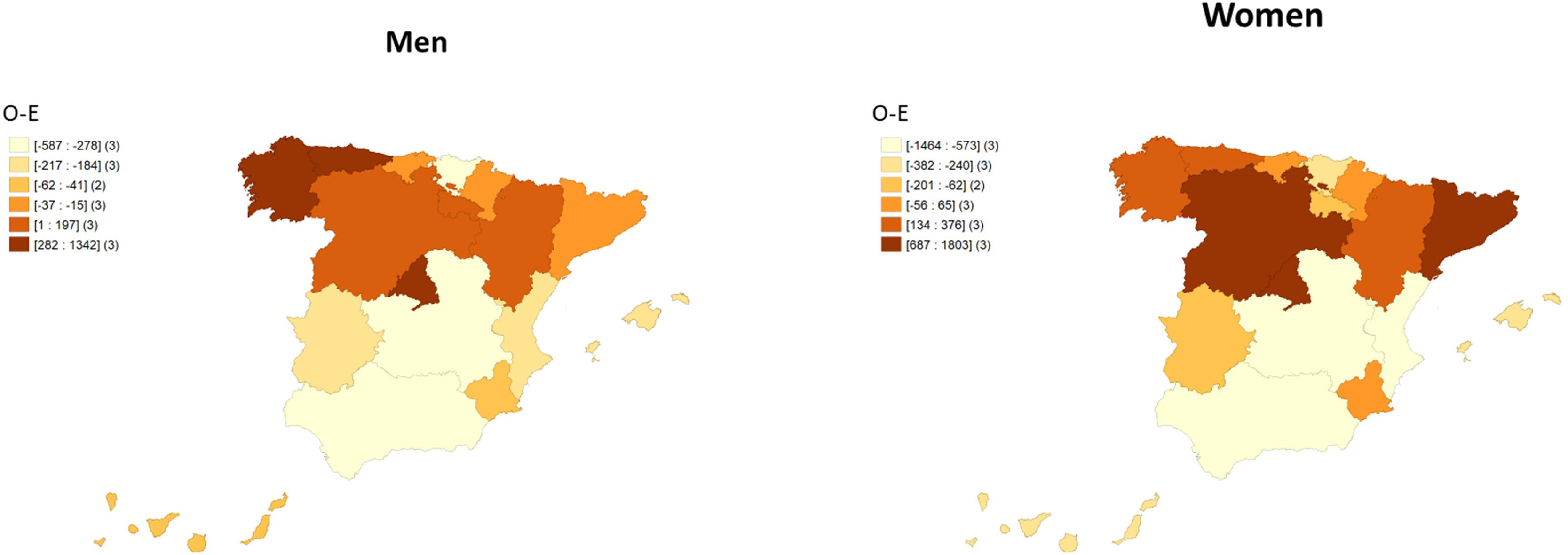
Fig. 4 shows the difference between the observed and the expected cases by AC and sex. Once again, we found a north-south gradient, with the highest excess cases in the north in both sexes. With RRs of 1.29 in women and 1.48 in men (both with PP >0.95), the Community of Madrid showed the highest number of cases above expected (1803 in women and 1342 in men).
Discussion
Our results provide the most recent estimates of MS prevalence in Spain and the geographical distribution of the disease at the AC level by sex, based on data from the BDCAP of the National Health System.
Our results showed differences in prevalence rates between Spanish ACs, which could indicate that genetic, environmental, and/or health practice differences play a role in the geographical distribution of prevalence rates. This may support the existence of a north-south gradient in Spain. Our findings are consistent with previous studies reporting a north-south gradient in both MS mortality25,26 and prevalence11 in Spain, as well as in other countries.4,27–30 Furthermore, a recent systematic review of MS prevalence studies in Spain revealed that MS prevalence has increased over the last decades, and that for every 10 degrees of latitude, the point prevalence per 100000 population increased by 13 cases. In general, studies presented data from specific areas of the different ACs, except Extremadura. The sources used to identify patients with MS were medical records from neurology services, data from the minimum basic dataset at hospital discharge, and primary care physicians, among others.11
In this study, we identified a higher adjusted prevalence rate (123.5 cases per 100000 population) in Spain than in previous studies carried out in different geographical areas of the country.11 Our results are consistent with previous studies that supported an increase in MS prevalence and placed Spain in the high-risk area of MS.11 In San Vicente del Raspeig (a town located in the AC of Valencia) during the period 2005–2018, the prevalence increased from around 6 cases per 100000 in the 1980s to 111.9 (the age-adjusted prevalence for the European standard population20 was 107 cases per 100000).31 Unfortunately, the authors do not provide age- and sex-adjusted data. Our results for the AC of Valencia showed an unadjusted prevalence rate of 115.8 cases per 100000, similar to that observed in this town.
The increase in prevalence may be related to an increase in MS incidence derived from a higher number of diagnosed patients and/or an increased risk of disease, or to greater survival due in part to the use of DMTs. Diagnostic improvements with magnetic resonance imaging, the cerebrospinal fluid analysis, and advances in MS diagnostic criteria allow the identification of previously underdiagnosed cases of MS.32
The female/male ratio was 2.0, which was similar to the ratio found in other European studies.33 Our results support the notion that MS is more prevalent in women, especially at younger ages.
Environmental and lifestyle factors, such as vitamin D deficiency, smoking, and Epstein-Barr virus infection,34 interacting with genetic factors can contribute to susceptibility and disease severity35 and could contribute to the geographic pattern observed through increased incidence.
It is possible that the differences observed in the prevalence of MS between autonomous communities located at the same latitude (such as Galicia and the Basque Country) are due to a combination of genetic susceptibility and variations in environmental and lifestyle factors. However, since our study is descriptive in nature, we can only speculate on these differences.
Recent evidence suggests that lifestyle changes, including increased use of sunscreen, together with higher rates of obesity and overweight, have led to a decline in vitamin D levels in the general population. This decline in vitamin D levels is thought to have contributed to an increase in the frequency of HLA-DRB1*15, a genetic risk factor for MS.36
Galicia has a significant excess of cases, and prevalence rates are among the highest in the country, for both men and women. It has a rainy climate, with few hours of sunshine per year and little exposure to UV rays; in this regard, it has been found that a high proportion of the Galician population is vitamin D-deficient.37 Furthermore, the increase in incidence and prevalence rates in recent decades in certain areas of Galicia has been attributed to a decrease in mortality and, consequently, prolonged survival.38 This may have contributed to the higher prevalence of MS observed in our study results for both sexes. Furthermore, in some areas of this AC, MS prevalence rates were among the highest observed to date in Spain, with figures close to those of northern areas of Nordic and Anglo-American influence.37,39–41 It should be noted that this geographical region has historically been exposed to several Viking settlements and invasions, as well as other Norman invasions, resulting in a high genetic susceptibility to MS.42
In Spain, according to BDCAP data, only 6% of patients with MS (3913 cases) were born in other countries, with a prevalence rate of 61 cases per 100000, lower than that recorded in the population of Spanish origin (147 cases per 100000).43 A French study44 showed that prevalence data and the north-south gradient could be modified due to the proportion and distribution of immigrants across the territory studied. Nonetheless, we did not find any change in our spatial-temporal pattern related to the inclusion of this population. The changes in the north-south gradient could be related to intrinsic characteristics of immigration, such as genetic factors or associated comorbidities.45 An example is the Roma population that migrated to the southern area of Spain, in which it has been postulated that MS prevalence is lower than the white population in Spain.46 Furthermore, in recent decades, there has been significant immigration and settlement in these regions of the Latin American population, among whom the prevalence of MS was lower.47
Although greater harmonization is taking place, there are still differences in diagnostic and therapeutic approaches in Spain depending on the place of residence and local policy guidelines related to pharmaceutical spending. Thus, the excess cases observed in the AC of Madrid could be associated with a greater diagnostic capacity, as the region has five multidisciplinary units for the management of MS. Three of these centers are considered national reference centers, out of a total of 12. On the other hand, Andalusia, with two MS reference units, and Murcia, with one, presented significantly fewer cases than expected. For this reason, we cannot rule out that these differences in prevalence were related to differences in healthcare resources between ACs.48
Since survival may be influenced by the use of DMTs, future epidemiological studies should evaluate their use in the regions studied. In Spain, the few studies that report information on the use of DMTs show an increase.31,46 Information on the use of DMTs in different countries is also scarce, although a European survey of neurologists highlighted the variability in many aspects of MS management.49
Strengths and limitationsThe main limitations of the study arise from its design, as it is a cross-sectional study of data from actual practice in primary care; its main strength is the use of a large, nationally representative sample. Data were obtained from individuals registered in the public primary care system (98.6% of the resident population of Spain), although it was not possible to include data from those registered in private care. Furthermore, given the particular characteristics (mainly their small population) of the autonomous cities of Ceuta and Melilla (located on the coast of North Africa), they were not included in this study to preserve the confidentiality of potential cases. This could lead to an underestimation of the true prevalence and should therefore be taken into account when interpreting our results.
The delay between disease onset and diagnosis, as well as the possibility that some patients with mild symptoms did not seek medical attention, may have contributed to an underestimation of prevalence. It is also possible that the primary care physician was unaware of the diagnosis and did not refer the patient to a neurologist. In addition, given the differences in the coding systems used to identify the different health problems in the different autonomous communities, the BDCAP standardized the original ICD-9, ICD-10ES, and ICPC-2 codes, and translated them into a common classification based on the ICPC-2. This was a major limitation of the study, as it was not possible to analyze prevalence data according to different MS phenotypes. However, our findings may lead to the development of new causal hypotheses.
Although our study has certain limitations (given its descriptive nature), it still provides important information that may inform future research efforts. By taking a systematic approach to analyzing the data and developing informed hypotheses, we can begin to unravel the complex mechanisms underlying the geographic pattern observed and pave the way for more comprehensive analytical studies that may shed more light on the geographic differences observed.
ConclusionsWe calculated an MS prevalence rate of 123.5 cases per 100000 person-years in Spain in 2021. In addition, after mapping the prevalence results at the AC level, we detected a north-south gradient similar to that observed in other countries and reported in previous studies. Our results provide further evidence of the increase in MS risk observed in Spain over the last 3 decades, with prevalence rates placing Spain in a high-risk prevalence zone. We were unable to assess prevalence data distributed by the different MS phenotypes. However, our results pave the way for future strategies to understand the causal hypothesis and to establish future care strategies to manage the burden of MS in Spain.
FundingResearchers did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ contributionsLucía Cayuela: conceptualization; research; methodology; manuscript drafting. Cristina García-Muñoz: supervision; validation; visualization; manuscript review and editing. Susana Sainz de la Maza: supervision; validation; visualization; manuscript review and editing. Aurelio Cayuela: conceptualization; data curation; formal analysis; research; methodology; project administration; supervision; validation; visualization; manuscript drafting.
Conflicts of interestNone declared.
Data availabilityThe data that support the findings of this article will be shared on reasonable request to the corresponding author and are available from the Primary Care Clinical Database (BDCAP).

