



Multiple sclerosis (MS) is a neurodegenerative disease characterised by inflammation and demyelination. It generates irreversible myelin changes, which in turn give rise to physical and cognitive disorders. The verbal fluency test (VF) has been shown to be a sensitive tool for detecting cognitive impairment in these patients.
ObjectiveTo compare quantitative and qualitative aspects of performance on semantic and phonological fluency tests between MS patients and healthy controls by analysing total words produced and strategies used (clusters and switching).
MethodWe evaluated 46 patients with MS and 33 healthy controls using the VF test.
ResultsThe semantic VF task revealed no significant differences between groups; for the phonological task, the patients demonstrated reduced word production (F [77]=2.286 P<0.001) and poorer use of grouping strategies, resulting in more frequent switching (F [77]=3.808 P<0.005).
ConclusionsThese results support using qualitative analysis for recall strategies, since the technique provides data about which components of the task are affected by brain damage. Clusters depend on the integrity of semantic memory, while switching has to do with developing effective search strategies, cognitive flexibility, and the ability to modify responses. Frontal lobe damage has been reported in MS, and this is consistent with results from the phonological VF test.
La esclerosis múltiple (EM) es un padecimiento neurodegenerativo caracterizado por inflamación y desmielinización y que conduce a un cambio irreversible de la mielina, lo que conlleva a la presencia de alteraciones físicas y cognitivas. La prueba de fluidez verbal (FV) ha demostrado ser sensible para evidenciar deterioro cognitivo en estos pacientes.
ObjetivoComparar aspectos cuantitativos y cualitativos del desempeño en pruebas de fluidez semántica y fonológica en pacientes con EM y sujetos sanos, mediante el análisis del total de palabras producidas y de las estrategias utilizadas (agrupaciones y saltos).
MétodoSe evaluaron 46 pacientes con EM y 33 sujetos sanos mediante la prueba de FV.
ResultadosEn la FV semántica no hubo diferencia estadística entre los grupos. En la FV fonológica los pacientes presentaron menor producción de palabras (F [77]=2,286; p<0,001) con una deficiente estrategia de agrupación, por lo tanto mayor número de saltos (F [77]=3,808;p<0,005).
ConclusionesEstos resultados apoyan la realización de un análisis cualitativo de las estrategias de evocación, al aportar datos sobre los componentes de la tarea que se ven alterados por el daño cerebral. Las agrupaciones dependen de la integridad de la memoria semántica, mientras que los saltos del desarrollo de una estrategia de búsqueda eficaz, de flexibilidad cognitiva y de la capacidad para modificar la respuesta. En la EM se ha reportado daño del lóbulo frontal, lo que concuerda con los resultados obtenidos en la prueba de FV fonológica.
Multiple sclerosis (MS) is a neurodegenerative disease characterised by inflammation and demyelination. It results in irreversible damage to myelin, followed by axon damage.1 The most heavily affected sites are the optic nerve, the periventricular white matter, cerebellum, and spinal cord.2
Each patient's symptoms, mainly referring to physical, cognitive, and/or emotional changes, depend on the MS lesion sites and lesion load.
The most frequent cognitive manifestations in MS are changes in short-term memory3; decreases in such abilities as attention4 and processing speed5; and difficulties with problem-solving or executive functions,6–8 visuospatial abilities,9 and verbal fluency.10 Multiple studies report that between 40% and 64% of patients experience such symptoms.11–15
Verbal fluency (VF) paradigm is commonly used in neuropsychological evaluation. These tests are classified as semantic or phonemic,16 and they are conducted by having a subjects list, in a set period of time, as many words as possible within a certain category (semantic category or words beginning with, containing, or lacking a specific letter). This test has proved its sensitivity for diagnosing cognitive impairment in MS, as shown by Paes14 and Negreiros,17 who reported a sensitivity of 80.6% and a specificity of 97.2% for this test in patients with MS.
Traditionally, this test is scored only by a quantitative scale (number of words a subject utters in a specified time period). However, qualitative analysis of the word production process has determined that words are generated according to the strategies the subject follows. According to Troyer,18 presenting words in categories or groups is known as ‘clustering’; when the group or subcategory has been exhausted, the subject will open a new category in a practice called ‘switching’.
Verbal fluency is considered a useful task for measuring different executive abilities because it involves the capacity for controlled and programmed verbal production, planning ability, organisation of responses, and elimination of previously uttered responses.19 Likewise, analysis of phonemic and semantic fluency as separate recall tasks, with emphasis on such strategies as clustering and switching, has been proposed as a means of increasing the specificity and value for lesion location of these tests.20
The purpose of this study was to compare quantitative and qualitative aspects of performance on semantic and phonemic fluency tests in patients with MS and in healthy subjects by analysing total words produced and the strategies employed (clustering and switching).
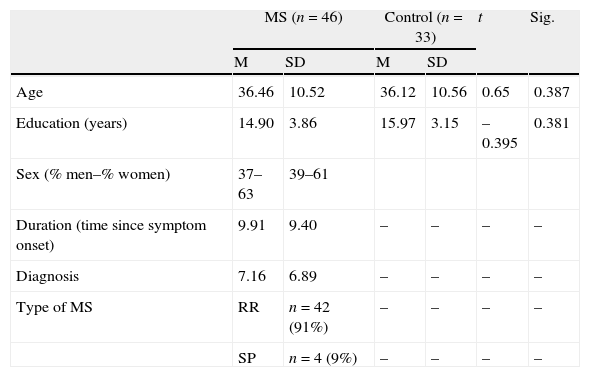
Materials and methodsSubjectsWe evaluated 79 patients divided into 2 groups: 46 patients with MS defined according to imaging criteria and the revised 2010 McDonald criteria for MS21 (clinical group); and a control group of 33 healthy age- and education-matched subjects with no history of neurological or psychiatric disease. The clinical group was composed of patients attended at the MS clinic at Mexico's National Institute of Neurology and Neurosurgery (INNNMVS). Table 1 displays sample characteristics.
Sample characteristics (MS-control).
| MS (n=46) | Control (n=33) | t | Sig. | |||
| M | SD | M | SD | |||
| Age | 36.46 | 10.52 | 36.12 | 10.56 | 0.65 | 0.387 |
| Education (years) | 14.90 | 3.86 | 15.97 | 3.15 | –0.395 | 0.381 |
| Sex (% men–% women) | 37–63 | 39–61 | ||||
| Duration (time since symptom onset) | 9.91 | 9.40 | – | – | – | – |
| Diagnosis | 7.16 | 6.89 | – | – | – | – |
| Type of MS | RR | n=42 (91%) | – | – | – | – |
| SP | n=4 (9%) | – | – | – | – | |
SD: standard deviation; M: mean; RR: relapsing-recurring; SP: secondary progressive.
Semantic VF test: this task evaluates verbal fluency for a semantic category (animals). During this test, the subject provides as many names as possible belonging to this category in one minute.
The phonemic VF test we used was the Controlled Oral Word Association Test (COWAT).22 This test consists of listing words belonging to different phonetic categories. Specifically, the subject must list in one minute all known words beginning with each letter of the triad ‘P’, ‘M’, and ‘R’.23 Restrictions apply, such as not using proper names, numbers, or diminutive or derivative forms.
All participants underwent 2 screening tests to rule out cognitive impairment and/or depression. These were the Cognitive Assessment Screening Instrument (CASI)24 with a cut-off point of 82, and the Beck Depression Inventory25 with a cut-off point of 16.
ProcedureThis study was approved by the ethics committee at INNNMVS and all participants signed an informed consent form as stipulated by the Declaration of Helsinki of 1975.
All subjects were evaluated individually by the same neuropsychologist. Instructions for the semantic VF test were as follows. “I would like you to list words belonging to the ‘animals’ category. Please think of any kind of flying or swimming animals, woodland creatures, and animals of all types. Now, name as many animals for me as you can. You have one minute to do so.” All animals named within the one-minute time limit were counted to generate the final score. We did not count duplicate names, variant names referring to the same species (horse/foal, cow/calf), names of races within a species (shepherd, greyhound, etc.) or generic categories (‘bird’ rather than ‘sparrow’, etc.). Intrusive and perseverative responses were also omitted.
Instructions for the phonemic VF test were as follows. “I am going to say a letter of the alphabet, and then I want you to give me as many words that begin with that letter as quickly as you can. You may say any words except for proper names, such as the names of people or places. Also, do not repeat words or say the same word with a different ending, as in ‘clean’, ‘cleaner’, ‘cleaning’. You have one minute to do so”. The test is scored by counting the number of words given per letter, and the statistical analysis was based on the sum of the scores for all 3 letters.
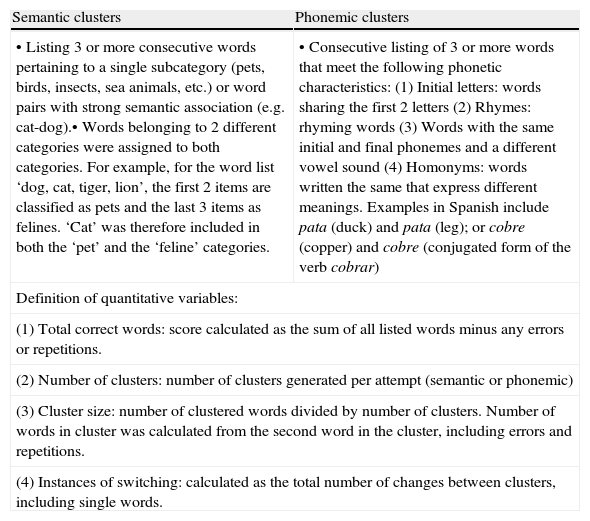
Qualitative analysis of the tests was performed using a Spanish-language adaptation (Villodre et al.20) of the criteria drawn up by Troyer et al.26 for clustering and switching (Table 2).
Scoring rules for clustering and switching.
| Semantic clusters | Phonemic clusters |
| • Listing 3 or more consecutive words pertaining to a single subcategory (pets, birds, insects, sea animals, etc.) or word pairs with strong semantic association (e.g. cat-dog).• Words belonging to 2 different categories were assigned to both categories. For example, for the word list ‘dog, cat, tiger, lion’, the first 2 items are classified as pets and the last 3 items as felines. ‘Cat’ was therefore included in both the ‘pet’ and the ‘feline’ categories. | • Consecutive listing of 3 or more words that meet the following phonetic characteristics:(1) Initial letters: words sharing the first 2 letters(2) Rhymes: rhyming words(3) Words with the same initial and final phonemes and a different vowel sound(4) Homonyms: words written the same that express different meanings. Examples in Spanish include pata (duck) and pata (leg); or cobre (copper) and cobre (conjugated form of the verb cobrar) |
| Definition of quantitative variables: | |
| (1) Total correct words: score calculated as the sum of all listed words minus any errors or repetitions. | |
| (2) Number of clusters: number of clusters generated per attempt (semantic or phonemic) | |
| (3) Cluster size: number of clustered words divided by number of clusters. Number of words in cluster was calculated from the second word in the cluster, including errors and repetitions. | |
| (4) Instances of switching: calculated as the total number of changes between clusters, including single words. | |
Data were analysed using SPSS statistical software, version 15.0 and t-test analysis was applied to study intra-group differences between demographic variables. The different measures of verbal fluency were analysed using one-way ANOVA and the Pearson correlation coefficient. The level of statistical significance was set at P<0.05.
ResultsDemographic variablesNo significant age or education-related differences were found between the groups. We examined the impact of these variables on total word production and on the strategies employed. Educational level was positively correlated to total production of words beginning with ‘P’ (r=0.346; P<0.001) and number of switching instances in the same task (r=0.263; P<0.05). No statistically significant correlations were found between age and VF.
We observed that the control group displayed significant sex-related differences for phonemic VF: men produced more words (50.38±8.57) than women (43.05±3.31) (P<0.022). Women in the MS group listed more words during both the semantic task (19.76±4.87 vs 15.53±4.23; P<0.004) and the phonemic task (38.52±11.23 vs 27.47±9.04; P<0.001), with a higher switching frequency (34.9±11.5 vs 23.4±8.6).
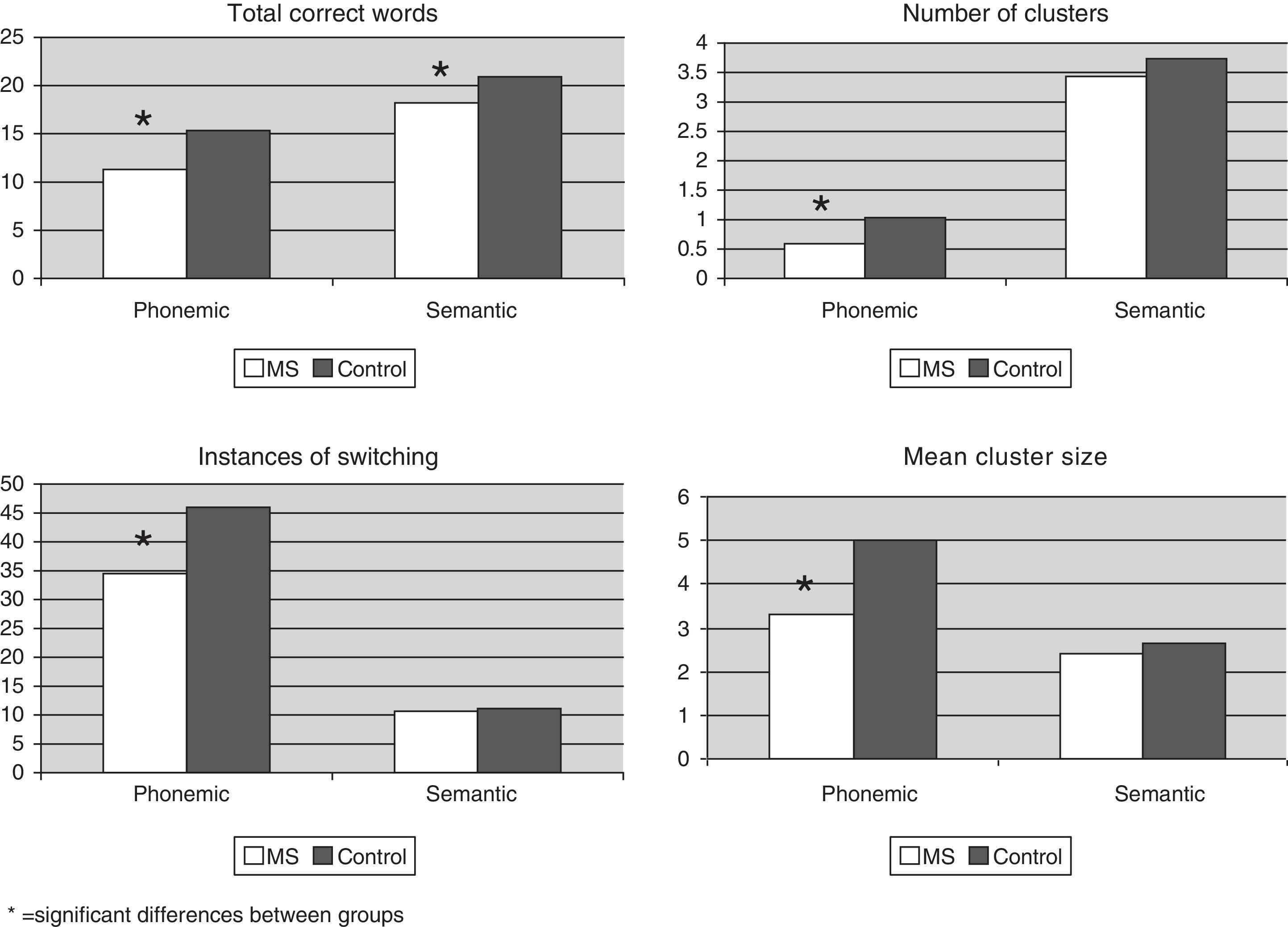
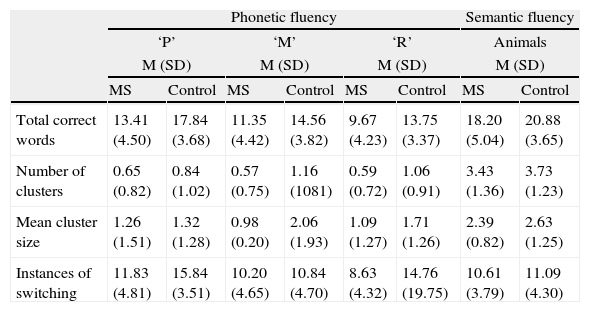
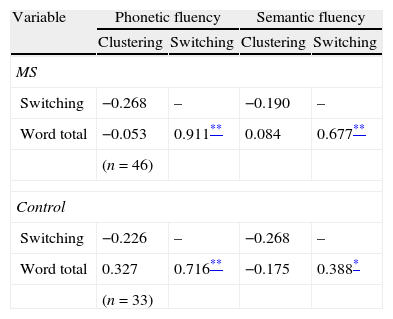
Recall strategies: clustering and switchingFor the sample total, word production for the semantic fluency task (19.32±4.67) was greater than for the phonemic fluency task (13.08±4.03) and semantic clustering (2.49±1.02) was more frequent than phonemic clustering (1.35±0.09). As a result there were fewer instances of semantic switching (10.81±3.99) than of phonemic switching (11.16±3.73). Analysis of the phonemic VF test showed that the subjects uttered more words, with more clustering and switching for the initial letter ‘P’ than for ‘M’ or ‘R’ (Table 3). This is confirmed in the correlation analysis in which the total number of words generated in both the semantic and the phonemic tasks by both groups was positively correlated to instances of switching (P<0.01) (Table 4).
Verbal fluency production strategies for the 2 study groups: means (M) and standard deviations (SD).
| Phonetic fluency | Semantic fluency | |||||||
| ‘P’ | ‘M’ | ‘R’ | Animals | |||||
| M (SD) | M (SD) | M (SD) | M (SD) | |||||
| MS | Control | MS | Control | MS | Control | MS | Control | |
| Total correct words | 13.41 (4.50) | 17.84 (3.68) | 11.35 (4.42) | 14.56 (3.82) | 9.67 (4.23) | 13.75 (3.37) | 18.20 (5.04) | 20.88 (3.65) |
| Number of clusters | 0.65 (0.82) | 0.84 (1.02) | 0.57 (0.75) | 1.16 (1081) | 0.59 (0.72) | 1.06 (0.91) | 3.43 (1.36) | 3.73 (1.23) |
| Mean cluster size | 1.26 (1.51) | 1.32 (1.28) | 0.98 (0.20) | 2.06 (1.93) | 1.09 (1.27) | 1.71 (1.26) | 2.39 (0.82) | 2.63 (1.25) |
| Instances of switching | 11.83 (4.81) | 15.84 (3.51) | 10.20 (4.65) | 10.84 (4.70) | 8.63 (4.32) | 14.76 (19.75) | 10.61 (3.79) | 11.09 (4.30) |
Fluency variable correlation coefficients for the 2 groups.
Comparing performances between the 2 groups revealed significant differences in phonemic VF limited to the 4 recall strategies: word total (F[77]=22.38; P<0.001), number of clusters (F[77]=10.86; P<0.001), number of switches (F[77]=7.67; P<0.007), and cluster size (F[77]=7.70; P<0.007) (Fig. 1).
Discussion
Analysis of performance on VF tests has gained importance in recent decades in such fields as neurology and neuropsychology. These tests are quick and easy to use in both clinical and research settings and they have demonstrated high diagnostic sensitivity for cognitive changes in neurological patients.
This study suggests that performance on VF tests should be analysed both quantitatively and qualitatively, using recall strategies (number and size of clusters; use of switching). This analysis provides information that will be useful for detecting cognitive changes in patients with MS.
In addition to considering the impact of demographic variables (age, educational level, sex) on verbal fluency test performance,27 Dursun et al.28 examined the effects of age and years of education on VF results in healthy subjects. Both variables were shown to be good predictors of scores on the FAS test, and no sex effect could be identified. Similarly, Lanting et al.29 found an age effect but no sex effect. In our study, both sex and educational level were linked to significant differences; within the MS group, men showed poorer performance on semantic and phonemic fluency tasks, as well as poorer use of recall strategies. Results from the phonemic VF task for the letter ‘P’ showed a positive correlation with educational level since there are more words beginning with this letter, as reported by other studies.30,31
Regarding clinical variables such as type of MS and progression time, some authors point to significant cognitive differences between patients with relapsing-remitting MS, which mainly impacts memory tasks, and secondary progressive MS, which predominantly affects the frontal lobe tasks involved in executive processes.32,33 Other authors mention that patients with a long history of chronic MS perform poorly on both semantic and phonemic VF tests.34 In this study, progression time was not correlated to any of the VF scores, and no links could be established between VF scores and types of MS because of the heterogeneity of the patient sample.
From the anatomical and physiological standpoint, it should be stressed that VF is a multidimensional process, and good performance will require access to semantic memory and an efficient recall process. In other words, memory and the executive functions related to the temporal and frontal lobes must be in good working order. In this way, we can distinguish between semantic VF and phonemic VF: the former is related to temporal lobe function and the latter35–37 to frontal lobe function.38–40 This concept was developed thanks to lesion studies and functional neuroimaging techniques that provided information about cerebral correlates of such tasks. Using SPECT studies, Pozzilli et al.41 found a significant reduction in the frontal and left temporal lobes in patients with MS. They highlighted the relationship between left temporal lobe anomaly and deficient verbal memory and VF.
Psycholinguistic analysis of the VF task allows us to distinguish between 2 types of fluency. First, semantic VF, which is based on the property of language for grouping named objects in categories. De Vega et al.42 write that “the cognitive system reduces the universe's complexity and variability to a limited conceptual structure”, thus delivering a system of categories. In contrast, phonemic VF for a task with specific instructions requires the creation of uncommon word recall strategies based on their lexical features and suppressing meaning-based responses.43 It differs from semantic VF in the number of cognitive steps the subject must take before recalling the word.
On the other hand, it is important to consider the fact that word recall is determined by the ‘availability’ of these words, whether individually or grouped. ‘Availability’ is determined from 2 angles. On the one hand, there are prototypes, i.e. all elements serving a function within a category (for example, domestic animals, farm animals, etc.). On the other hand, we find cognitive factors affecting recall of the word, that is, the subject's familiarity with the word, age at acquisition, and frequency of the word.44
This being the case, the most available words also tend to be the most familiar, and they are therefore used more frequently. Manoiloff et al.45 wrote that patients with MS tend to establish fewer clusters among the words they utter, and that these clusters consist of words that are very familiar in our cultural setting.
ConclusionsPatients with MS and the general population show similar total scores and number of clusters on VF tests. Nevertheless, they show fewer instances of switching, a strategy related to the executive component. This phenomenon may be linked to changes in the frontal component, whereas the temporal component may remain intact. VF performance may be used as a linguistic marker to differentiate between patients with MS and healthy subjects. Qualitative analysis of recall strategies allows us to perform a more in-depth study of cognitive changes which may not be noticed in some patients.
Results from this study therefore have implications for both clinical practice and research; clustering seems to predict organisational strategies, while the switching pattern may indicate problems with executive function in neurological disorders. Nevertheless, one of our study's limitations is its sample size, and we recommend performing larger studies to follow up on this idea.
FundingCONACYT (Mexican Council of Science and Technology).
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors would like to thank Dr Francisco Paz for his assistance with statistical analysis in this project.
Please cite this article as: Velázquez-Cardoso J, Marosi-Holczberger E, Rodríguez-Agudelo Y, Yañez-Tellez G, Chávez-Oliveros M. Estrategias de evocación en la prueba de fluidez verbal en pacientes con esclerosis múltiple Neurología. 2014;29:139–145.
