



In clinical neuropsychology, normative data are necessary to relate the performance of a subject to a reference group. These normative data should be collected from a pertinent population taking into account sociodemographic and cultural factors.
ObjectiveThis paper describes the methods and sample characteristics of a series of Spanish normative studies on young adults (NEURONORMA young adults project, NNy). The normative information was based on a series of selected, commonly used, neuropsychological tests covering attention, language, visual-perceptual abilities, constructional tasks, memory, and executive functions.
Material and methodsA sample of 179 cognitively normal subjects from 18 to 49 years was studied. Demographics, socio-cultural, and medical data were collected. The statistical procedure used in the normative studies is described.
ResultsSociodemographic, family background, health habits, medical history and use of drugs are presented.
ConclusionsThe use of these norms should improve neuropsychological diagnostic accuracy in young Spanish subjects. These data may also be of considerable use for comparisons with other normative studies.
En neuropsicología clínica es necesario disponer de datos normativos con el fin de relacionar el comportamiento de un sujeto con un grupo de referencia. Estos datos normativos deben extraerse de una población pertinente, teniendo en cuenta las características propias de cada cultura y el efecto de las variables sociodemográficas.
ObjetivoDescribir los métodos y las características de la muestra de una serie de estudios normativos españoles en población adulta joven (Proyecto NEURONORMA jóvenes). Se incluyen tests neuropsicológicos de uso extendido para valorar atención, lenguaje, habilidades visuoperceptivas, habilidades visuoconstructivas, memoria, y funciones ejecutivas.
Material y métodosSe estudió una muestra de 179 sujetos cognitivamente normales, con un rango de edad de 18 a 49 años. Se recogieron datos demográficos, socioculturales y médicos. Se describe el procedimiento estadístico utilizado en el estudio normativo.
ResultadosSe presentan los datos sociodemográficos, los antecedentes familiares, los hábitos de salud, los antecedentes médicos y el uso de fármacos.
ConclusionesEl uso de estas normas será de gran utilidad para el diagnóstico neuropsicológico en sujetos españoles jóvenes, así como para la comparación con otros estudios normativos.
It is extremely important in clinical neuropsychology to have access to normative data in order to compare a single subject's behaviour with that of a group.1,2 During neuropsychological evaluations, a subject's performance on cognitive tests is compared with a standard chosen by the test administrator. This standard is based on normality, which can be defined for our purposes as the range of behaviours and abilities displayed by a group of individuals with a common social, educational, cultural, and generational background.3 Normative data should therefore be collected from the population in question, keeping in mind the characteristics peculiar to each culture, and the effect of sociodemographic variables.4–7 Age, educational level, and sex are sociodemographic factors with a substantial potential influence on cognitive performance.
There is consensus in the literature as to the effect of age on cognition. However, a number of factors in addition to age may contribute to a specific cognitive status. These include educational level, intelligence, lifestyle, emotional state, personal habits and interests, and general state of health.1–4 According to the classic model,8,9 verbal abilities and the array of learned information (crystallised intelligence) remain stable over time, while reasoning/resolution of unfamiliar problems (fluid intelligence) and psychomotor abilities begin to decline at about age 55. Studies using widely used test batteries clearly illustrate the effects of age on cognition. In an education-adjusted sample of subjects older than 19, Heaton et al.10 explored the effects of age on performance on different indexes in the Wechsler Adult Intelligence Scale-Third Edition (WAIS-III)11 and the Wechsler Memory Scale-Third Edition (WMS-III).12 They did not find any significant age effect on the verbal comprehension index, while the processing speed and visual memory indexes were shown to be affected by age. Effects of age were also found in performances on the Halsted–Reitan Neuropsychological Test Battery (HRB)13 in the areas of reasoning, abstraction, and logical analysis. Scores on other tests related to learning, past experience and language ability remained constant over time.14 However, some authors attribute poor performance on fluid intelligence tests to loss of speed (in psychomotor tasks and cognitive processing). This is because most of these tests include tasks with time limits.15 In a study of a sample of subjects younger than 40, Yeudall et al.16 did not find any links between age and performance on the HRB.
Published literature recognises the influence of educational level on a subject's performance on cognitive tests. The effects of education on test performance have been widely demonstrated for both verbal tests and cognitive tasks such as those drawing on visual memory, although it was once believed that education had no influence whatsoever on that area.1–4 Le Carret et al.17 found a significant link between subjects’ level of education and control over mental processing and conceptualisation abilities. Kaufman et al.18 concluded that education had a greater impact on verbal tasks than on non-verbal tasks. However, Heaton et al.10 found that education had a considerable effect on WAIS-III and WMS-III indexes, especially those having to do with verbal comprehension, perceptual organisation, and processing speed.
Most studies found similar levels of general intelligence between men and women. However, they have identified differences on tests evaluating specific abilities. Men tend to score higher on tests of spatial relationships, quantitative abilities, physical strength and motor speed, while women tend to score higher on tests of verbal ability.1,3 There are a number of models offering explanations; some attribute differences between the sexes to biological factors, others to psychosocial factors, and still others, to both.8,9
A few normative studies for neuropsychological tests in Spanish-speaking subjects have been published. For a full list, refer to the compendia of neuropsychological tests.1–4 However, most of these studies were carried out using small samples which differed from test to test. Furthermore, the tests are not adapted on the cultural and/or linguistic levels since they do not allow for certain characteristics of the Spanish population (educational system, types of bilingualism, etc.).
We are therefore faced with a need for normative data from the Spanish population. This gap was partially filled by the recent publication of the NEURONORMA project (NN), a study which obtained normative data on a selection of widely used neuropsychological tests from a Spanish population older than 49.19–25 However, data from young adults are still lacking. The present study, NNy, aims to build upon NN by gathering normative and psychometric information from a sample of subjects younger than 50, thereby remedying the lack of this type of data in Spain.
Our article provides a description of the sample and the general methodology used in NNy. The same neuropsychological tests were employed in both NNy and NN. Normative data from the tests described in this study have been published in independent articles.
Material and methodsSubjectsThe study was carried out in the Behavioural Neurology and Dementia unit at Hospital del Mar, Barcelona, Spain. Its design was cross-sectional. The project was approved by the Clinical Research Ethics Committee at Barcelona's Municipal Institute of Medical Research. The study was carried out according to the Declaration of Helsinki26 and European regulations on medical research.
Subjects were recruited from the following pools: (a) family members of patients cared for by the Behavioural Neurology and Dementia Unit at Hospital del Mar, Barcelona; (b) employees at the same hospital; and (c) family members and acquaintances of coordinators of the Master in Neuropsychology and Behavioural Neurology at Universitat Autònoma de Barcelona. All the participants were of European race and educated in Spain, regardless of their first language (for bilingual subjects). Recruitment was stratified by age and educational level. We defined 5 age ranges and 3 educational levels. A total of 179 subjects were included.
Subjects were selected according to the following inclusion and exclusion criteria:
Inclusion criteria: (a) signature of an informed consent document approved by the Ethics Committee; (b) age range between 18 and 49 years; (c) hearing, sight, and physical condition sufficient for testing purposes; (d) minimal ability to read and write; (e) Modified Ischemia Score27 equal to or less than 4; (f) score of 37 on the Interview for the Deterioration of Daily Living in Dementia (IDDD)28,29; (g) score on Mini Mental State Examination (MMSE)30,31 greater than or equal to 24; (h) score on the Memory Impairment Screen (MIS)32,33 greater than or equal to 4; (i) medical condition and medications stable in the 3 months prior to the start of the study; and (j) no clinically significant anomalies in the subject's medical history.
Exclusion criteria: (a) unwillingness or inability to participate fully; (b) any central nervous system disease that may affect cognition (movement disorder, brain tumour, hydrocephalus, epilepsy, subdural haematoma, multiple sclerosis, history of cerebral infarct or severe cranial trauma, etc.); (c) major depressive episode or dysthymia, according to DSM-IV criteria; (d) active or uncontrolled presence of systemic illness associated with a cognitive disorder (examples: hypothyroidism, vitamin B12 deficiency, insulin-dependent diabetes mellitus, kidney or liver disease or failure); (e) known unstable cardiovascular disease with a potential effect on cognitive functions; (f) infectious diseases (tertiary syphilis, known HIV); and (g) history or presence of abuse of alcohol or other drugs in the 24 months prior to the study.
The following tests were selected for use in the study:
- •
Spanish version of the MMSE validated by Blesa et al.30,31
- •
Spanish version of the MIS validated by Böhm et al.32,33
- •
Spanish version of the IDDD validated by Böhm et al.28,29 This scale measures functional disability in self-care (16 items) and in complex activities (17 items).
- •
Modified Ischemia Score27 to assess cerebrovascular risk.
We employed the neuropsychological profile established within the framework of the NN.19 The following tests were included: the Spanish version of verbal span (direct and inverse digit span)34; visuospatial span (Corsi block-tapping test) based on WAIS-R-NI35; Letter-Number Sequencing (WAIS-III)11; Trail Making Test36,37; Symbol Digit Modalities Test38; Boston Naming Test39,40; Token Test41; a selection of sub-tests from the Visual Object and Space Perception Battery42,43; Judgment of Line Orientation44,45; Rey–Osterrieth Complex Figure (copy and memory)46,47; Free and Cued Selective Reminding Test48,49; verbal fluency50, including 3 semantic fluency tasks (animals, fruits and vegetables, and kitchen tools), 3 formal phonemic tasks (words beginning with p, m, and r), 3 excluded-letter tasks (words not containing a, e, and s)51 and a verb fluency task; Stroop Color-Word Interference Test52,53; and Tower of London Drexel University version.54
ProceduresIn order to perform uniform evaluations, we implemented a series of measures to standardise procedures, methods, and diagnostic criteria. All the evaluators were psychologists with experience in test administration and neuropsychological diagnosis. The evaluators received training at the beginning of the project in order to employ the same testing method. The tests were administered according to the standard procedures described in their manuals.
Subjects were studied in a session lasting approximately 2hours, divided in 2 parts. In the first part, patients signed the informed consent form and researchers gathered the following information: health habits, medical history, pharmacological treatments, score on the Modified Ischemia Scale, the functional scale (IDDD) and the cognitive screening tests (MMSE, MIS). The second part consisted of administering the neuropsychological test battery selected for the normative study.
Statistical analysisStatistical analysis was performed using SPSS computer software version 18.0. The descriptive analysis included total percentage, mean, standard deviation and range. For articles in which data for each of the tests were analysed, we adopted a uniform normative procedure that followed the model used in NN.19
The procedure was as follows:
- (a)
Creation of a normative table of scaled scores (SS). This generated an array of accumulated frequencies of raw scores for the entire group. According to the methodology described by Peña-Casanova et al.,19 percentile ranges were assigned to raw scores according to their positions within the distribution. Percentile ranges were then converted to NSS (NEURONORMA Scaled Scores) ranging from 2 to 18. This transformation of raw scores to NSS produced a normal distribution (mean=10, standard deviation=3) to which linear regressions could be applied.
- (b)
Definition of age, sex, and education effects. Coefficients of correlation (r) and determination (R2) were determined for univariate regression analyses of NSS with age, years of education, and sex for each of the tests. Test scores were adjusted in cases in which the explained variation for sociodemographic factors exceeded 5%, and where coefficients of regression were statistically significant. Statistical significance was established at values of P<.05.
- (c)
Adjustments for age, education and sex. Adjustments to the NSS for age, education and sex were calculated according to the following formula: NSSA&E&S=PE−(β1*[Age-35]+β2*[Education-13]+β3*Sex). The regression coefficient (β) from this analysis was used as the basis for corrections. Mean age (35) and mean years of education (13) were used to centre adjustments. The resulting adjustment values were truncated to the lower whole number.
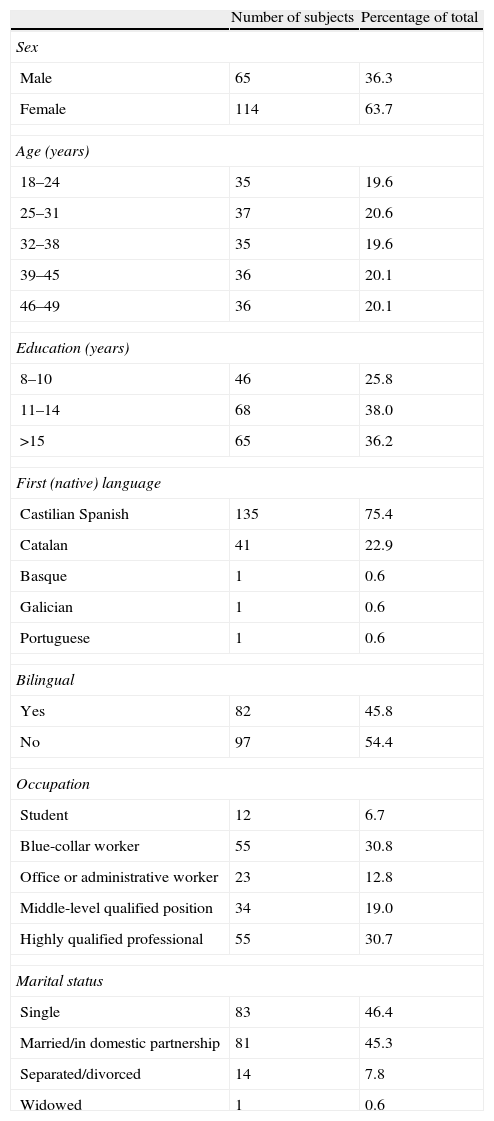
Table 1 summarises the sample's demographic characteristics (N=179). The sample contained more women than men. Most of the participants were categorised as married/in a domestic partnership or single, while a very low percentage was categorised as separated/divorced; only 1 subject was widowed. The largest employment categories were blue-collar workers and highly qualified professionals, while there were fewer administrative workers or those with middle-level qualifications. Only 2% were unemployed or students.
Sociodemographic characteristics.
| Number of subjects | Percentage of total | |
| Sex | ||
| Male | 65 | 36.3 |
| Female | 114 | 63.7 |
| Age (years) | ||
| 18–24 | 35 | 19.6 |
| 25–31 | 37 | 20.6 |
| 32–38 | 35 | 19.6 |
| 39–45 | 36 | 20.1 |
| 46–49 | 36 | 20.1 |
| Education (years) | ||
| 8–10 | 46 | 25.8 |
| 11–14 | 68 | 38.0 |
| >15 | 65 | 36.2 |
| First (native) language | ||
| Castilian Spanish | 135 | 75.4 |
| Catalan | 41 | 22.9 |
| Basque | 1 | 0.6 |
| Galician | 1 | 0.6 |
| Portuguese | 1 | 0.6 |
| Bilingual | ||
| Yes | 82 | 45.8 |
| No | 97 | 54.4 |
| Occupation | ||
| Student | 12 | 6.7 |
| Blue-collar worker | 55 | 30.8 |
| Office or administrative worker | 23 | 12.8 |
| Middle-level qualified position | 34 | 19.0 |
| Highly qualified professional | 55 | 30.7 |
| Marital status | ||
| Single | 83 | 46.4 |
| Married/in domestic partnership | 81 | 45.3 |
| Separated/divorced | 14 | 7.8 |
| Widowed | 1 | 0.6 |
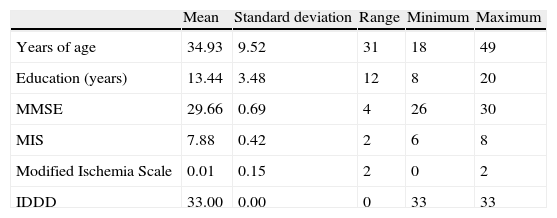
Table 2 shows the details of the inclusion criteria. Scores on the MMSE and MIS were within normal parameters in all subjects. IDDD scores showed that all patients were functionally normal. None of the subjects was at risk for ischaemia according to their Modified Ischemia Scores.27
Inclusion criteria.
| Mean | Standard deviation | Range | Minimum | Maximum | |
| Years of age | 34.93 | 9.52 | 31 | 18 | 49 |
| Education (years) | 13.44 | 3.48 | 12 | 8 | 20 |
| MMSE | 29.66 | 0.69 | 4 | 26 | 30 |
| MIS | 7.88 | 0.42 | 2 | 6 | 8 |
| Modified Ischemia Scale | 0.01 | 0.15 | 2 | 0 | 2 |
| IDDD | 33.00 | 0.00 | 0 | 33 | 33 |
IDDD: Interview for the Deterioration of Daily Living in Dementia; MIS: Memory Impairment Screen; MMSE: Mini Mental State Examination.
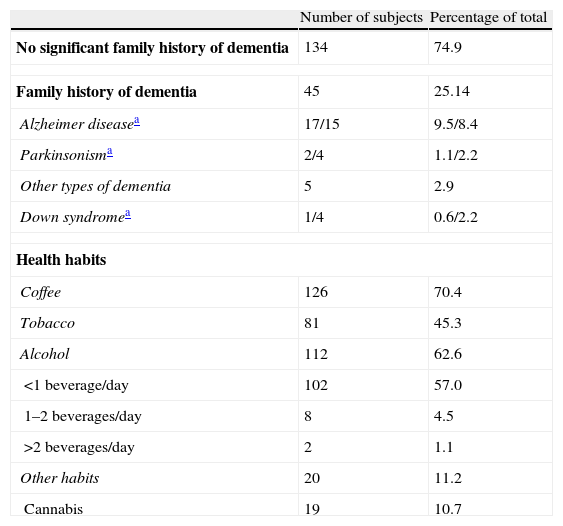
Table 3 offers a summary of family history and health habits. Alzheimer disease was the most common event in family histories. Most of the participants were daily coffee drinkers and consumed less than one alcoholic beverage per day. Occasional cannabis use was reported by 10.7%. Based on subjects’ consumption habits (frequency, quantity, and duration) and prior findings,55 cannabis use was not considered to have an effect on cognitive performance.
Family history and health habits.
| Number of subjects | Percentage of total | |
| No significant family history of dementia | 134 | 74.9 |
| Family history of dementia | 45 | 25.14 |
| Alzheimer diseasea | 17/15 | 9.5/8.4 |
| Parkinsonisma | 2/4 | 1.1/2.2 |
| Other types of dementia | 5 | 2.9 |
| Down syndromea | 1/4 | 0.6/2.2 |
| Health habits | ||
| Coffee | 126 | 70.4 |
| Tobacco | 81 | 45.3 |
| Alcohol | 112 | 62.6 |
| <1beverage/day | 102 | 57.0 |
| 1–2beverages/day | 8 | 4.5 |
| >2beverages/day | 2 | 1.1 |
| Other habits | 20 | 11.2 |
| Cannabis | 19 | 10.7 |
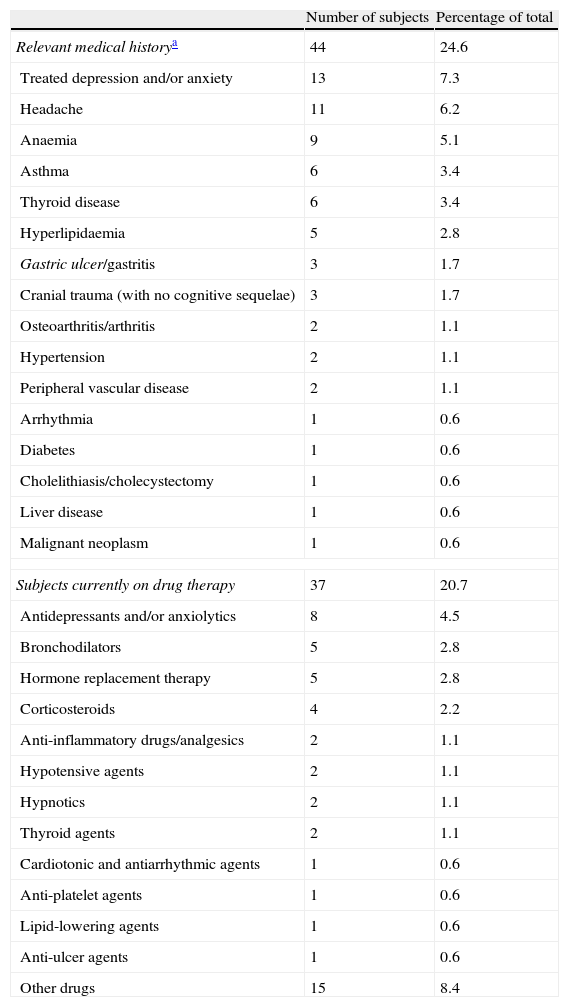
Table 4 lists medical histories and medication use. Of the subjects, 24.6% reported experiencing or having experienced one of the pathologies listed in the study. Headache was the most common pathology, followed by anaemia, followed by depression, asthma and anxiety. At the time of this study, all cases of depression and anxiety were controlled with medication and these illnesses had no effect on cognitive function. In addition, 20.7% of the participants were on medication at the time of the study. The most common drugs were bronchodilators, antidepressants, and hormone replacement treatments.
Medical history and medication use.
| Number of subjects | Percentage of total | |
| Relevant medical historya | 44 | 24.6 |
| Treated depression and/or anxiety | 13 | 7.3 |
| Headache | 11 | 6.2 |
| Anaemia | 9 | 5.1 |
| Asthma | 6 | 3.4 |
| Thyroid disease | 6 | 3.4 |
| Hyperlipidaemia | 5 | 2.8 |
| Gastric ulcer/gastritis | 3 | 1.7 |
| Cranial trauma (with no cognitive sequelae) | 3 | 1.7 |
| Osteoarthritis/arthritis | 2 | 1.1 |
| Hypertension | 2 | 1.1 |
| Peripheral vascular disease | 2 | 1.1 |
| Arrhythmia | 1 | 0.6 |
| Diabetes | 1 | 0.6 |
| Cholelithiasis/cholecystectomy | 1 | 0.6 |
| Liver disease | 1 | 0.6 |
| Malignant neoplasm | 1 | 0.6 |
| Subjects currently on drug therapy | 37 | 20.7 |
| Antidepressants and/or anxiolytics | 8 | 4.5 |
| Bronchodilators | 5 | 2.8 |
| Hormone replacement therapy | 5 | 2.8 |
| Corticosteroids | 4 | 2.2 |
| Anti-inflammatory drugs/analgesics | 2 | 1.1 |
| Hypotensive agents | 2 | 1.1 |
| Hypnotics | 2 | 1.1 |
| Thyroid agents | 2 | 1.1 |
| Cardiotonic and antiarrhythmic agents | 1 | 0.6 |
| Anti-platelet agents | 1 | 0.6 |
| Lipid-lowering agents | 1 | 0.6 |
| Anti-ulcer agents | 1 | 0.6 |
| Other drugs | 15 | 8.4 |
This study describes the sample and methodology used in expanding the NN to include the young adult population. The main purpose of our project was to obtain normative data for a population of young Spanish adults using a battery of neuropsychological tests. A number of cognitive tests were normalised at the same time (simultaneous normalisation) and the scores converted to a single scale. This permitted direct comparisons between performances related to different cognitive functions. This approach lets us identify models of characteristic neuropsychological syndromes.56
Cognitive normality of the study subjects was validated by means of cognitive screening tests (MMSE and MIS). As in NN,19 subjects did not have to be wholly disease-free in order to participate in the study.57 As a result, subjects with active or chronic medical, psychiatric, or neurological disorders and/or physical disabilities were included in the sample if the disorder was properly controlled or resolved, and if the researchers felt that it did not cause cognitive decline. The same criteria also applied to cases of consumption of medications or psychoactive drugs.
Spanish speakers who also spoke one of Spain's co-official languages (Catalan, Galician, or Basque) were included. This characteristic is a true reflection of the sociodemographic make-up of Spain. One participant whose first language was Portuguese was also included, as the subject had been educated in Spain and was fully competent in Spanish. Sample characteristics with regard to health habits, medical history and drug use were clearly described.
Comparison of the samples from both NN studies reveals a few differences which are listed below. These must be taken into account if we are to consider the data obtained from both samples as a single dataset. Firstly, the NNy group did not include subjects with fewer than 8 years of formal education, while subjects of this description were included in the older subject sample. This difference in range for the “years of education” variable is the reason why explained variation is lower in the young adult group. This phenomenon might lead us to believe that the effect of education on performance was weaker in the young adult sample, but this is not the case. Secondly, fewer subjects were included in NNy and use of the midpoint statistical technique was discontinued.19 Lastly, subjects in the young adult sample presented fewer concomitant illnesses and were treated with fewer drugs.
Raw scores were converted into scaled scores so as to be able to compare performances on different tests. Linear regression analysis was performed to adjust scores by age, education, and sex for variables identified as having a significant effect on those factors.
This study has several limitations. One is its relatively small sample size. Even so, we should be mindful of the fact that the study was completed in order to fill an urgent healthcare need.
Another of the study's limitations is that we did not use epidemiological recruitment methods. Stratifying the sample by 3 educational levels and 5 age groups was identified as the most economical and practical solution. We did not recruit completely uneducated or minimally educated subjects because such subjects would be very rare given the current sociodemographic conditions.
The study also has the limitations common to all normative studies. The use of normative data is appropriate for patients whose demographic characteristics resemble those of subjects in the normative sample.4 We cannot conclude that these norms could be generalised to other Spanish-speaking populations without empirical evidence to support their applicability. However, the data from this study may be used with caution to evaluate Spanish-speaking subjects from other countries, since some evidence suggests that age and educational level affect performance more than country of origin. This was the conclusion reached by multiple meta-analyses that compared semantic verbal fluency data.58,59
Lastly, we should mention that sociodemographic characteristics help predict performance on neuropsychological tests without there being a cause–effect relationship between those characteristics and performance. They should therefore be used with caution when identifying acquired cerebral lesions in the case of subjects with developmental disorders or educated in special school systems.3
Nonetheless, this study improves on other prior studies in the area of neuropsychological examinations in young adults in that it gathers scaled scores that can be applied to a cognitive profile permitting direct comparison between tests.
Conclusions and future researchThis study provides normative data from an array of cognitive tests that are widely used in neuropsychological examinations. These data have been treated so as to be useful to doctors providing diagnoses. These new data serve as an aid in clinical tasks, differential diagnosis, establishing prognosis, planning treatment, and performing public health studies and clinical research.60
Lastly, we propose the following objectives for future studies: (a) complete and expand the current sample in the context of a Spanish multicentre project; (b) develop a complete cognitive profile for young adults; (c) study different types of patients in order to establish cognitive profiles that may aid in differential diagnosis; and (d) study the behaviour of the different samples included in the NN as a whole.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Peña-Casanova J, et al. Estudios normativos españoles en población adulta joven (Proyecto NEURONORMA jóvenes): métodos y características de la muestra. Neurología. 2012;27:253–60.
