





Multiple sclerosis (MS) is a chronic immunological, inflammatory, demyelinating, and neurodegenerative disease. Nutrition has been considered a possible factor in the pathogenesis of MS for some years. There is currently no consensus on the monitoring of eating habits to improve the course and/or symptoms of the disease, as there is insufficient evidence to recommend a specific diet for patients with MS. On this basis, the purpose of this study is to compare the daily eating habits of MS patients in three different countries (China, Spain, and Cuba) that allow us in the future to explore healthier diets for them, and assessing risk factors for relapse in patients with MS.
Material and methodWe have adopted a questionnaire design based on the use of the web to evaluate the daily eating habits of patients with MS in three different countries: China, Spain, and Cuba. According to the options of MS patients in the daily eating habits questionnaire, we divided them into two main eating habits: mixed diet and Mediterranean diet. We performed a logistic regression analysis to explore risk factors for relapse in patients with MS.
ResultsOur study found that in the three countries, China, Spain, and Cuba, MS patients are the most common in women, the incidence rate from women to men is 2-3:1, which usually starts between the ages of 25 and 59 years old, and relapsing–remitting is the most common type of MS, 70-80% of MS patients have experienced disease relapse to varying degrees during the course of their illness. Most MS patients in China and Cuba have a mixed diet, while MS patients in Spain have a Mediterranean diet. Through logistic regression analysis, we found that the type of diet is an important risk factor for relapse of MS (p = 0.003, OR = 2.628, 95% CI: 1.393-4.968), the risk of relapse of MS by mixed diet is 2.6 times greater than that of the Mediterranean diet.
ConclusionThe components of the daily diet of MS patients in three different countries are basically the same, but China and Cuba have mixed diets, while Spain has mainly a Mediterranean diet. Our research clearly shows that the Mediterranean diet can reduce the risk of relapses in MS patients. We believe that it is essential to carry out large-scale multicenter studies to verify these findings, which may be of great relevance in the management of MS.
La esclerosis múltiple (EM) es una enfermedad inmunológica, inflamatoria, desmielinizante y neurodegenerativa crónica. La nutrición se considera desde hace unos años un posible factor en la patogenia de la EM. Actualmente no existe un consenso sobre el seguimiento de hábitos alimentarios para mejorar el curso y / o los síntomas de la enfermedad, ya que no hay evidencia suficiente para recomendar una dieta específica para pacientes con EM. Sobre esta base, el propósito de este estudio es comparar los hábitos alimentarios diarios de los pacientes con EM en tres países diferentes (China, España y Cuba) que nos permitan en el futuro explorar dietas más saludables para ellos, y evaluar los factores de riesgo de brotes y recaídas de los pacientes con EM.
Material y métodoHemos adoptado un diseño de cuestionario basada en la utilización de la web para evaluar los hábitos alimentarios diarios de los pacientes con EM en tres países diferentes: China, España y Cuba. Según las opciones de los pacientes con EM en el cuestionario de hábitos alimentarios diarios, los dividimos en dos hábitos alimentarios principales: dieta mixta y dieta mediterránea. Realizamos un análisis de regresión logística para explorar factores de riesgo de brotes o recaídas en pacientes con EM.
ResultadosNuestro estudio encontró que en los tres países China, España y Cuba, los pacientes con EM son los más comunes en mujeres, la tasa de incidencia de mujeres a hombres es de 2-3: 1, que suele comenzar entre los 25 y 59 años, y la remitente-recurrente es el tipo de EM más común, el 70-80% de los pacientes con EM han experimentado brotes de la enfermedad en grado diferente durante el curso de su enfermedad. La mayoría de los pacientes con EM en China y Cuba tienen una dieta mixta, mientras que los pacientes con EM en España tienen una dieta mediterránea. Mediante análisis de regresión logística, encontramos que el tipo de dieta es un factor de riesgo importante para la recaída de la EM (p = 0.003, OR = 2.628, 95%CI: 1.393-4.968), el riesgo de recaída de la EM por dieta mixta es 2.6 veces mayor que el de la dieta mediterránea.
ConclusiónLos componentes de la dieta diaria de los pacientes con EM en tres países diferentes son básicamente los mismos, pero China y Cuba tienen dietas mixtas, mientras que España tiene principalmente una dieta mediterránea. Nuestra investigación muestra de forma clara que la dieta mediterránea puede reducir el riesgo de brotes o recaídas en pacientes con EM. Creemos que es imprescindible realizar estudios multicéntricos a gran escala para verificar estos hallazgos que pueden tener gran relevancia en el manejo de la EM.
Multiple sclerosis (MS) is a chronic immune, inflammatory, demyelinating and neurodegenerative disease of the central nervous system (CNS), characterized by demyelination that damages nerve fibers and myelin sheaths, affecting the brain, spinal cord and the optic nerves.1 The global average prevalence of MS is 33 out of 100,000 people, and it is increasing in both developed and developing countries.2 The prevalence of MS varies widely in different countries, Europe and North America have the highest prevalence (108 and 140 per 100,000 people, respectively), while Asia and sub-Saharan Africa have the lowest prevalence (2.1 and 2.2 per 100,000 population, respectively).3 MS appears mainly after the age of 30,4 and its prevalence is high in women (approximately a 3:1 ratio).5 The cause of MS is unknown, but it is believed to be the result of a complex interaction between genetic predisposition and environmental exposure,6 environmental influences modify the risk and progression of the disease, possibly through epigenetic changes that could positively or negatively regulate the immune response and influence neuronal development.3,7 Environmental factors mainly include smoking, low vitamin D due to inadequate exposure to sunlight, Epstein–Barr virus infection, and a variety of dietary factors.6,8 There is currently no curative treatment for MS, but disease-modifying therapy can stabilize its progression in the early flare phase and possibly delay the transition to a secondarily progressive phase of the disease.9
Nutrition is considered a possible influencing factor in the pathogenesis of MS. Nutritional intervention studies have shown that diet can be regarded as an adjuvant treatment to control disease progression and has the potential to reduce MS-related symptoms.10 A healthy diet, providing adequate amounts of essential nutrients and limiting saturated fat intake, can improve the course of MS,11 which is consistent with a study by Fitzgerald, which suggested that high-quality diets that emphasize the intake of fruits, vegetables, legumes, and whole grains, and low intakes of sugar and red meat are associated with lower levels of disability and fatigue in people with MS.12 The justification for the dietary intervention is based on the effect of these dietary factors in the control of the inflammation process and oxidative stress.13 The process of controlling inflammation is carried out through epigenetic changes in gene expression and changes in the composition of the intestinal microbiome.6 Diet can directly affect the gut microbiota by providing substrates to support the growth of members of the gut community, and it can also directly affect the gut microbiota by inhibiting the growth of gut community germs.14 In addition, diet can indirectly affect intestinal flora by affecting host immunity, intestinal barrier function, and the production of host-derived by-products.14
Currently, many researchers attempt to treat MS through special diets, including the Swank low saturated fat, McDougall low fat plant-based diets, Mediterranean diet, fasting/energy restriction ketogenic diet, and modified Paleolithic diet.6 Since there is currently no consensus on following eating habits to improve the course and/or symptoms of the disease, there is insufficient evidence to recommend a specific diet for MS patients. Different countries have different customs and are in different climates, so the food products are different, which leads to differences in the final food culture. Therefore, we have carried out this questionnaire to evaluate the daily eating habits of MS patients in three different countries: China, Spain, and Cuba, and explore a healthier diet for them. Furthermore, we evaluated whether different diets are risk factors for relapse in patients with MS.
Material and methodStudy designWe have designed a questionnaire in two languages: Chinese and Spanish based on the use of a website to evaluate the daily eating habits of MS patients in three different countries: China, Spain, and Cuba. The questionnaire was distributed through private institutions and social networks, we used the public platform WeChat for the Chinese, the official website of the DINAC Foundation for the Spanish and the WhatsApp platform for the Cubans. The questionnaire survey began on September 1, 2020 and ended on September 30, 2020. The first question of the questionnaire allows patients to freely choose if they are willing to participate in the study, if they wish to continue with the questionnaire, if they refuse, will exit the questionnaire. Everyone is informed of the objectives of the investigation and is asked to accept the privacy and data exchange policy. Participants' personal information is anonymized to maintain and protect confidentiality. The anonymous nature of online investigations does not allow the tracking of personal data in any way. This research was approved by the Ethics Committee of the Virgen Macarena University Hospital.
ParticipantsParticipants were recruited from MS research centers in three different countries. The participants from China, Spain, and Cuba came from the Yan'an University Medical College No.3 Affiliated Hospital, the Department of Research and Treatment of MS of the DINAC Foundation and the Department of Neurology of the Hospital Hermanos Ameijeiras in the province of Havana, respectively. All participants were over 15 years of age and diagnosed with MS according to McDonald's 2017 diagnostic criteria. Patients under 18 years of age required the consent of their legal guardians.
Demographic, anthropometric and clinical variablesFor details of the questionnaire, please refer to Supplementary 1. Through the questionnaire, we collected the demographic characteristics of the relevant participants (sex and age), anthropometric characteristics (weight, height, and calculated body mass index (BMI)), clinical characteristics (time since MS diagnosis, clinical classification of MS, if they had had flare-ups or relapses of the disease in the past year and its possible trigger).
Eating habits questionnaireThe daily eating habits questionnaire that we designed provides us with information on the daily eating habits of MS patients. The main food categories included: rice and derived products, pasta and products derived from flour, other cereals (such as beans, oatmeal, etc.), vegetables, all types of meats (including fat and lean), lean meats, fish and shellfish, eggs, milk or yogurt, butter and cream, other dairy products, olive oil, other edible oils except olive oil (such as sunflower oil, soybean oil, sesame oil, etc.), fruits, nuts, sweets (such as chocolate, cakes, ice cream, etc.), coffee, tea, low-salt diet (< 2 g/day). The self-assessment questionnaire is multiple choice, MS patients choose the options that best suit them according to their eating habits.
According to the options of MS patients in the daily eating habits questionnaire, we divided them into two main eating habits: mixed diet and Mediterranean diet. The mixed diet includes all types of meat or fish, vegetables, fruits, dairy products, and cereals. The Mediterranean diet is a diet that consumes a large amount of fruits, vegetables, lean meats, fish, shellfish, olive oil, nuts, and a small amount of butter and cream.
Statistical analysisFor statistical analysis, we used SPSS software, version 25.0. Before analyzing the data, each variable will be displayed individually, eliminating possible transcription errors. Qualitative data were expressed as mean ± standard deviation (x ± s), quantitative data were expressed as number and percentage in parentheses (%). In addition, we did a logistic regression analysis to explore risk factors for relapse in patients with MS. It was considered statistically significant when the value of p < 0.05.
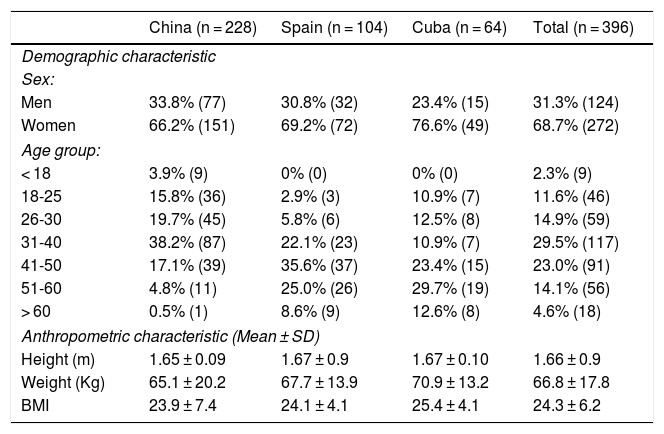
ResultsDemographic and anthropometric characteristicsThe demographic and anthropometric characteristics shown in table 1. We received a total of 396 questionnaires from patients with multiple sclerosis, and the ratio of men to women was 31.3% vs. 68.7%. In China, 228 MS patients participated in the questionnaire, of which 33.8% were men and 66.2% were women. In Spain 104 patients participated, the majority are Andalusians, of which 30.8% were men and 69.2% were women. There were 64 patients coming from Cuba, of which 23.4% were men and 76.6% were women.
Demographic and anthropometric characteristics of the study population.
| China (n = 228) | Spain (n = 104) | Cuba (n = 64) | Total (n = 396) | |
|---|---|---|---|---|
| Demographic characteristic | ||||
| Sex: | ||||
| Men | 33.8% (77) | 30.8% (32) | 23.4% (15) | 31.3% (124) |
| Women | 66.2% (151) | 69.2% (72) | 76.6% (49) | 68.7% (272) |
| Age group: | ||||
| < 18 | 3.9% (9) | 0% (0) | 0% (0) | 2.3% (9) |
| 18-25 | 15.8% (36) | 2.9% (3) | 10.9% (7) | 11.6% (46) |
| 26-30 | 19.7% (45) | 5.8% (6) | 12.5% (8) | 14.9% (59) |
| 31-40 | 38.2% (87) | 22.1% (23) | 10.9% (7) | 29.5% (117) |
| 41-50 | 17.1% (39) | 35.6% (37) | 23.4% (15) | 23.0% (91) |
| 51-60 | 4.8% (11) | 25.0% (26) | 29.7% (19) | 14.1% (56) |
| > 60 | 0.5% (1) | 8.6% (9) | 12.6% (8) | 4.6% (18) |
| Anthropometric characteristic (Mean ± SD) | ||||
| Height (m) | 1.65 ± 0.09 | 1.67 ± 0.9 | 1.67 ± 0.10 | 1.66 ± 0.9 |
| Weight (Kg) | 65.1 ± 20.2 | 67.7 ± 13.9 | 70.9 ± 13.2 | 66.8 ± 17.8 |
| BMI | 23.9 ± 7.4 | 24.1 ± 4.1 | 25.4 ± 4.1 | 24.3 ± 6.2 |
Note: BMI: body mass index; Kg: kilogram; m: meter; SD: standard deviation.
In the questionnaire, we divided different age ranges. In China, 3.9% were under 18 years old, 15.8% were between 18 and 25 years old, 19.7% were between 26 and 30 years old, 38.2% were between 31 and 40 years old, 17.1% were between 41 and 50 years old, 4.8% were between 51 and 60 years old, and 0.5% were older than 60 years of age. In Spain, 2.9% were between 18 and 25 years old, 5.8% between 26 and 30 years old, 22.1% between 31 and 40 years old, 35.6% were between 41 and 50 years old, 25.0% between 51 and 60 years old, and 8.6% were older than 60 years of age. In Cuba, 10.9% were between 18 and 25 years old, 12.5% between 26 and 30 years old, 10.9% between 31 and 40 years old, 23.4% were between 41 and 50 years old, 29.7% between 51 and 60 years old, and 12.6% were older than 60 years of age. Looking globally from the three countries together, the MS patients were mostly between 31 and 50 years old.
The average height, weight, and BMI of Chinese MS patients were 1.65 m, 65.1 kg and 23.9; of the Spanish were 1.67 m, 67.7 kg, 24.1; of the Cubans were 1.67 m, 70.9 kg, 25.4.
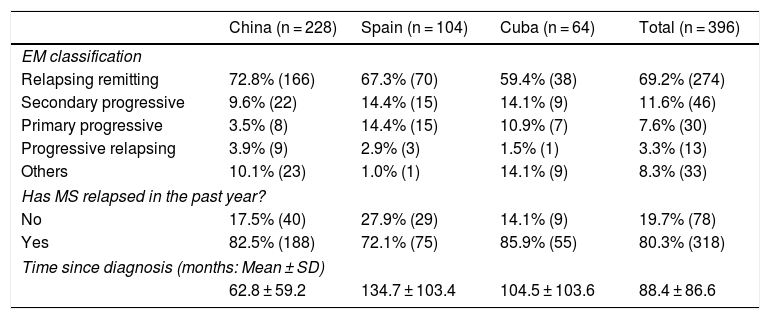
Clinical featuresThe clinical characteristics of the population are shown in table 2. Regarding the phenotypic classification, the relapsing remitting type was the most frequent and it was presented globally by 69.2% in the three countries, 72.8% in the Chinese, 67.3% in the Spanish, and 59.4% in the Cubans. The rest of secondary progressive, primary progressive, and progressive relapsing affect 9.6%, 3.5%, and 3.9% in Chinese; 14.4%, 14.4%, and 2.9% in the Spanish, and 14.1%, 10.9%, and 1.5% in the Cubans, respectively. Chinese patients with MS who have experienced relapse of the disease accounted for 82.5%, Spaniards accounted for 72.1%, and Cubans accounted for 85.9%. Since the diagnosis of MS patients, the mean duration of MS in China was 62.8 months, that of the Spanish was 134.7 months, and that of the Cubans was 104.5 months. The mean duration of MS in these three countries was 88.4 months.
Clinical characteristics of the study population.
| China (n = 228) | Spain (n = 104) | Cuba (n = 64) | Total (n = 396) | |
|---|---|---|---|---|
| EM classification | ||||
| Relapsing remitting | 72.8% (166) | 67.3% (70) | 59.4% (38) | 69.2% (274) |
| Secondary progressive | 9.6% (22) | 14.4% (15) | 14.1% (9) | 11.6% (46) |
| Primary progressive | 3.5% (8) | 14.4% (15) | 10.9% (7) | 7.6% (30) |
| Progressive relapsing | 3.9% (9) | 2.9% (3) | 1.5% (1) | 3.3% (13) |
| Others | 10.1% (23) | 1.0% (1) | 14.1% (9) | 8.3% (33) |
| Has MS relapsed in the past year? | ||||
| No | 17.5% (40) | 27.9% (29) | 14.1% (9) | 19.7% (78) |
| Yes | 82.5% (188) | 72.1% (75) | 85.9% (55) | 80.3% (318) |
| Time since diagnosis (months: Mean ± SD) | ||||
| 62.8 ± 59.2 | 134.7 ± 103.4 | 104.5 ± 103.6 | 88.4 ± 86.6 | |
Note: MS: multiple sclerosis; SD: standard deviation.
The daily diets of Chinese MS patients mainly include: rice (83.8%), pasta (60.5%), legumes (28.5%), vegetables (85.5%), all kinds of meats (including fat and lean 51.3%), lean meat (37.3%), fish and seafood (36.8%), eggs (76.3%), milk or yogurt (58.3%), butter and cream (4.39%), other dairy products (7.46%), olive oil (6.58%), other food oils except olive oil (28.5%), fruits (78.5%), nuts (37.8%), and sweets (18.42%). The daily diets of Spanish MS patients mainly include: rice (57.7%), pasta (59.6%), legumes (56.7%), vegetables (83.7%), all kinds of meats (including fat and lean 57.7%), lean meat (27.9%), fish and seafood (75.0%), eggs (79.8%), milk or yogurt (66.3%), butter and cream (19.2%), other dairy products (18.3%), olive oil (94.2%), other food oils except olive oil (6.7%), fruits (78.8%), nuts (56.7%), and sweets (29.8%). The daily diets of Cuban MS patients mainly include: rice (95.3%), pasta (53.1%), legumes (32.8%), vegetables (65.6%), all kinds of meats (including fat and lean 82.8%), lean meat (7.81%), fish and seafood (37.5%), eggs (89.1%), milk or yogurt (75.0%), butter and cream (26.6%), other dairy products (25.0%), olive oil (15.6%), other food oils except olive oil (64.1%), fruits (71.9%), nuts (9.38%), and sweets (60.9%). A comprehensive comparison of the diets in the three countries shows that the basic dietary structure is very similar, but there are also some important differences (fig. 1). For example, the daily diet of the Spanish in fish, shellfish, nuts, and olive oil is significantly higher than that of China and Cuba. In Cuba, the daily intake of butter, cream, sweets, and coffee is significantly higher than that of China and Spain, and the diet of Cubans is mainly low in salt.

Based on the daily eating habits of each MS patient, we divide their diet into two main types: mixed diet and Mediterranean diet. The main diet of Chinese MS patients was the mixed diet, which accounted for 96.9% (221), and the Mediterranean diet accounted for only 3.1% (7). In Cuban MS patients, the mixed diet represented 90.6% (58) and the Mediterranean diet represented 9.4% (6). However, Spanish patients with MS dominate the Mediterranean diet 78.8% (82), and the mixed diet only represented 21.2% (22) (fig. 2).
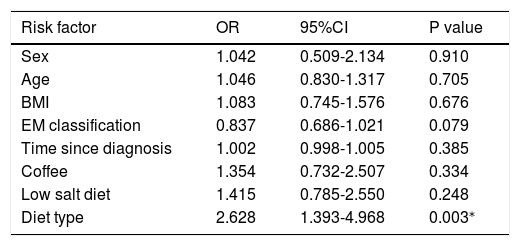
Risk factors affecting relapse in MS patients
We used logistic regression analysis to screen for risk factors for MS relapse, we found that the type of diet was a significant risk factor for MS relapse (p = 0.003, OR = 2.628, 95% CI: 1393-4968), while other variables were not risk factors for MS relapse, such as age, sex, BMI, MS Classification, Time since MS diagnóstico, Coffee, and a low-salt diet (table 3). The risk of relapse of MS with a daily mixed diet is 2.6 times higher than that of the Mediterranean diet.
Logistic regression analysis of the risk factors for relapse of MS.
| Risk factor | OR | 95%CI | P value |
|---|---|---|---|
| Sex | 1.042 | 0.509-2.134 | 0.910 |
| Age | 1.046 | 0.830-1.317 | 0.705 |
| BMI | 1.083 | 0.745-1.576 | 0.676 |
| EM classification | 0.837 | 0.686-1.021 | 0.079 |
| Time since diagnosis | 1.002 | 0.998-1.005 | 0.385 |
| Coffee | 1.354 | 0.732-2.507 | 0.334 |
| Low salt diet | 1.415 | 0.785-2.550 | 0.248 |
| Diet type | 2.628 | 1.393-4.968 | 0.003⁎ |
Note: BMI: body mass index; CI: confidence interval; MS: multiple sclerosis; OR: odds ratio.
MS is a chronic disease of the central nervous system with inflammatory and neurodegenerative components, most patients initially present a remitting–recurrent course. MS is believed to be the result of a combination of genetic predisposition and environmental influences. Diet is an important source of environmental interaction, and dietary metabolites exert far-reaching systemic effects, making diet an attractive candidate as a potential environmental mediator in MS.15 Diets cannot replace conventional treatment in MS patients, but a healthy nutritional intervention is well accepted and can improve their physical and inflammatory condition.10 A study on this topic revealed that increased fruit and vegetable intake is associated with lower levels of disease activity and disability reported by MS patients.16 Another prospective pediatric MS study points to an increased risk of relapse associated with higher intake of saturated fat, and also noted that as vegetable intake increases, the relapse rate decreases.17 Furthermore, it has been found that patients perceive how the severity of the daily manifestations of their disease symptoms is directly related to the excessive consumption of meat, fatty foods, and processed sugars.9 However, and despite the importance of diet for the disease, eating habits in patients with MS have not been studied in depth so far. With this in mind, the purpose of this study is to compare the daily eating habits of MS patients in three different countries (China, Spain, and Cuba) and to explore healthier diets for them, and to assess the risk factors for relapse of MS patients.
Our study found that in the three countries of China, Spain, and Cuba, MS patients are the most common in women, the incidence rate from women to men is 2-3:1, which usually occurs between 25 and 59 years, which coincides with the epidemiological characteristics of MS.18 Recurrent–remitting type is the most common type of MS in the three different countries, including 70-80% of MS patients have experienced relapse of the disease to varying degrees during the course of their disease. Most MS patients in China and Cuba have a mixed diet, while MS patients in Spain (most are Andalusian) have a typical Mediterranean diet. Mediterranean diets are low in saturated fat, high in polyunsaturated and monounsaturated fats (especially fish and olive oil), high in fruits, vegetables, nuts, and low in processed foods, which implies a low salt content. The Mediterranean diet is proposed to influence inflammation through increased consumption of antioxidants, including polyphenols.19 A recent study showed that adherence to the Mediterranean diet was associated with a reduction in the risk of MS.20 Another study randomly divided women with MS into a Mediterranean diet or a control diet for six months, the result showed that the Expanded Disability Status Scale (EDSS) was reduced and fatigue improved.21 Through logistic regression analysis, we found that the type of diet is an important risk factor for relapse of MS (p = 0.003, OR = 2.628, 95% CI: 1.393-4.968), the risk of relapse of MS by mixed diet is 2.6 times greater than that of the Mediterranean diet; Furthermore, other variables are not risk factors for relapse, such as age, sex, BMI, MS classification, time since MS diagnosis, coffee, and low-salt diet.
Well-designed studies have shown the benefits of the Mediterranean diet in preventing cardiovascular disease. In the 10-year follow-up of a cohort of almost 33,000 women in Sweden, a self-administered questionnaire recorded the food composition of the Mediterranean diet.22 The results showed that among these people who adhere to the Mediterranean diet, the incidence of myocardial infarction, acute ischemic stroke, and heart failure have been reduced.22 Both the American Heart Association and the American Stroke Association recommend a Mediterranean diet to prevent strokes.23 In addition, some studies have also shown that the Mediterranean diet is related to Alzheimer's disease or mild cognitive impairment, such as the degree of longitudinal cognitive impairment.24 The Mediterranean diet is considered a healthy diet, but there is very little work on the Mediterranean diet in MS. In this study we show that the Mediterranean diet can reduce relapse in MS patients, but large-scale multicenter studies are still needed to verify our findings in the future.
To our knowledge, this study is the first study to compare the daily eating habits of MS patients in three different countries and assesses the relationship between the Mediterranean diet and relapse of MS disease. However, we also admit that our study has its limitations, among them that the number of patients is small and the study population is limited to China, Spain, and Cuba. These patients come from different patients from different health systems, and the treatment standards they receive are not uniform. Second, the research is based on Internet questionnaires, which have their own shortcomings. Third, we have not yet considered the impact of disease-modifying treatments on results. Also, there is no healthy control group in this study and selection bias may exist. In the future, research should be conducted to cover patients from other countries, so that the MS eating habits of different ethnic and regional groups can be compared and analyzed.
ConclusionDiets cannot replace conventional treatment in MS patients, but a healthy nutritional intervention can be beneficial. There are few studies on the eating habits of MS patients in different countries and their effects on the disease. Our study found that the daily diet of MS patients in China and Cuba is based on mixed diet, while MS patients in Spain are based on Mediterranean diet. Our research shows that the Mediterranean diet can reduce the risk of flare-ups in MS patients. In the future, more large-scale, multicenter studies are still needed to verify our findings in the future.
Authors contributionsWen-Ting Zhang and Guo-Xun Zhang conceived and designed the study. Wen-Ting Zhang and Guo-Xun Zhang are responsible for data collection, analysis, and writing of the manuscript. Run-Ze Zhao, Shuai-Shuai Gao help in data collection. Gang Zhao provides advice on the manuscript. Guillermo Izquierdo is responsible for the conceptualization and revision of the manuscript. All authors read and approved the manuscript.
Questionnaire survey on daily eating habits of patients with multiple sclerosis (MS)
