


Holistic comfort is an important outcome in palliative care and an important goal for patients, relatives and healthcare workers. Holistic comfort considers one's acceptance of life circumstances, support from loved ones and health care professionals, and peaceful resolution of relationships during stressful situations. However, this type of comfort is still difficult to measure, particularly in palliative care patients, as there is a lack of instruments available, especially in the Portuguese language. This study aims to provide an accurate and sensitive instrument to assess the spiritual comfort of Portuguese palliative care patients.
ObjectiveTo perform the cultural adaptation and validation of a Portuguese version of the End of Life Comfort Planning Questionnaire in Palliative Care patients.
MethodsMethodological research, with analytical approach. The translation, synthesis, back translation, review, pretest, semantic evaluation and analysis of the psychometric properties were performed. A total of 141 palliative care patients from acute medical-surgical settings at a central hospital in the north of Portugal were recruited. The Ethics Committee approved the research.
ResultsThe internal consistency analysis of the adapted instrument resulted in a global alpha value of 0.84 and the factor analysis presented a solution with five factors with rational meaning. The Portuguese version comprised 20 items.
ConclusionsThe instrument has good psychometric properties. It was reliable, valid and sensitive to the existence of the spiritual comfort of palliative care patients, and appropriate for further research.
Holistic comfort is important in all human life, from the beginning of life to death and grieving. Several authors have been researching the conceptual definition and implementation of comfort in recent years, particularly in the context of illness, crisis situations or life transitions.1,2 The most widely known of the abovementioned work is Kolcaba's Comfort Theory, in which comfort is described as a holistic state resulting from satisfaction of the needs of relief, ease and transcendence in the physical, psycho-spiritual, sociocultural and environmental contexts.1
Recent studies have identified some inconsistencies and gaps in knowledge, particularly in terms of classifications and taxonomies of nursing knowledge, in which the concept is defined in a reductionist perspective as it is predominantly associated with the physical dimension.2,3 These gaps and inconsistencies may be related to the difficulty of measuring the concept. Therefore, Pinto et al.2–4 supported the idea of comfort as a complex experience, dependent on the behaviors of different actors and factors in every dimension of human life. Nevertheless, current scientific evidence demonstrates the existence of several deficits in the operational implementation and measurement of the concept with patients in palliative care. Problems with measurement in this population represent a serious limitation to the study and testing of the efficacy and effectiveness of nursing interventions, particularly at end of life.2,5
Currently there are in Portugal some instruments to measure similar constructs in palliative care patients, such as quality of life or wellbeing.6 However there are very few tools available worldwide to assess specifically patient comfort at the end of life, and in Portugal there is only one: Escala de Conforto Holístico HCQ – PT-DC©.7 Although validated in a sample of palliative care patients, some inconsistencies were found in Querido's instrument which may jeopardize the global score and an accurate evaluation of the implemented interventions. One of these inconsistencies is related to item #13 (“I made the right choice in choosing this place”). Indeed, contrary to what happens in the United States (where the original version is from), the patient in Portugal is rarely able to choose the place to be treated or hospitalized, despite all the developments in palliative care in the country.8
Moreover, item #8 (“My pain is difficult to endure”) may promote difficulties in the interpretation of the concept of pain, allowing the patient to understand the concept related to total pain exclusively in a physical perspective or, alternatively, from a more holistic point of view, so promoting bias. Furthermore, in the United States, patients rate their physical pain all the time from one to ten. It does not include existential pain. In Portugal, there is a growing effort to implement the pain as the fifth vital sign, but its evaluation is not yet a standardized practice.9,10 Also in palliative care, we do not believe that addiction is an appropriate concept when pain is pervasive or severe. In palliative care, many patients may be under the influence of opioids or other analgesics, which may have influenced in their answers.11,12
Taking into account the importance of an accurate assessment (either in the clinical practice, whether for research purposes/evaluation of the effectiveness of nursing interventions), we consider it important to study another instrument. For this project, we adapted and translated the End of Life Comfort Planning Questionnaire-Patient-Version found on Kolcaba's website (www.thecomfortline.com).13 This instrument closely approximated the holistic, spiritual qualities we were seeking to capture in palliative care patients in Portugal.
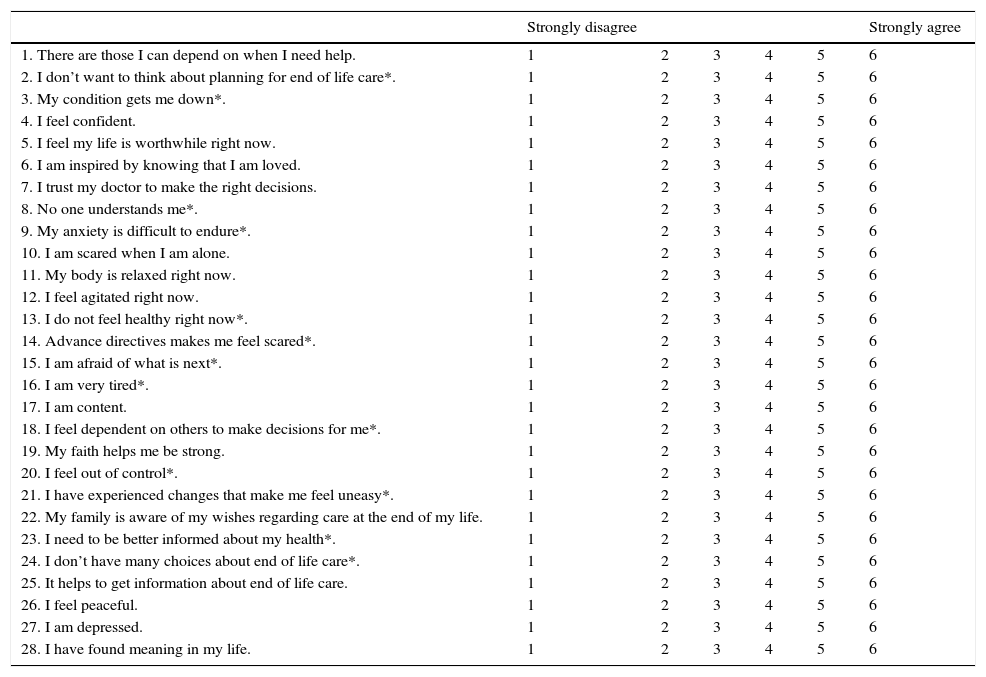
The End of Life Comfort Planning Questionnaire-PatientThe End of Life Comfort Planning Questionnaire-Patient (Table 1) was adapted and shortened from the original instrument of the Hospice Comfort Questionnaire-Patient.14 The new instrument is composed of 28 items, using a Likert scale from 1 to 6 (1 means “Strongly Disagree” and 6 “Strongly Agree”). It assesses spiritual comfort and the final score ranges from 28 to 168. The final score is calculated by the sum of the scores obtained in each item. The lower the score, the lower the comfort of the patient. For the analysis of the results it is important to consider that items #2, 3,8, 9, 13, 14, 15, 16, 18, 20, 21 and 23 and 24 are reversed.1,14 The original instrument had a Cronbach's Alpha of 0.98.14 Our End of Life Spiritual Comfort Questionnaire-Patient excludes pain and other physical symptoms assessment; however, it is very comprehensive in the assessment of psycho-spiritual-social dimensions, which are frequently neglected in health contexts in Portugal.
The End of Life Comfort Planning Questionnaire-Patient.
| Strongly disagree | Strongly agree | |||||
|---|---|---|---|---|---|---|
| 1. There are those I can depend on when I need help. | 1 | 2 | 3 | 4 | 5 | 6 |
| 2. I don’t want to think about planning for end of life care*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 3. My condition gets me down*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 4. I feel confident. | 1 | 2 | 3 | 4 | 5 | 6 |
| 5. I feel my life is worthwhile right now. | 1 | 2 | 3 | 4 | 5 | 6 |
| 6. I am inspired by knowing that I am loved. | 1 | 2 | 3 | 4 | 5 | 6 |
| 7. I trust my doctor to make the right decisions. | 1 | 2 | 3 | 4 | 5 | 6 |
| 8. No one understands me*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 9. My anxiety is difficult to endure*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 10. I am scared when I am alone. | 1 | 2 | 3 | 4 | 5 | 6 |
| 11. My body is relaxed right now. | 1 | 2 | 3 | 4 | 5 | 6 |
| 12. I feel agitated right now. | 1 | 2 | 3 | 4 | 5 | 6 |
| 13. I do not feel healthy right now*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 14. Advance directives makes me feel scared*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 15. I am afraid of what is next*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 16. I am very tired*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 17. I am content. | 1 | 2 | 3 | 4 | 5 | 6 |
| 18. I feel dependent on others to make decisions for me*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 19. My faith helps me be strong. | 1 | 2 | 3 | 4 | 5 | 6 |
| 20. I feel out of control*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 21. I have experienced changes that make me feel uneasy*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 22. My family is aware of my wishes regarding care at the end of my life. | 1 | 2 | 3 | 4 | 5 | 6 |
| 23. I need to be better informed about my health*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 24. I don’t have many choices about end of life care*. | 1 | 2 | 3 | 4 | 5 | 6 |
| 25. It helps to get information about end of life care. | 1 | 2 | 3 | 4 | 5 | 6 |
| 26. I feel peaceful. | 1 | 2 | 3 | 4 | 5 | 6 |
| 27. I am depressed. | 1 | 2 | 3 | 4 | 5 | 6 |
| 28. I have found meaning in my life. | 1 | 2 | 3 | 4 | 5 | 6 |
The instrument has already been adapted to the Brazilian population with Cardiac Insufficiency15 but there are few instruments concerning the assessment of non-physical comfort in palliative care. Non physical comfort refers to dimensions which do not “pertain to bodily sensations and homeostatic mechanisms”,1, p. 12 not only in Portugal but also around the world. Given the above, and with the objective of a holistic assessment of comfort, we propose that the Spiritual Comfort instrument supplements a physical comfort assessment. This supplemental assessment could be used in conjunction with a pain scale or in a more comprehensive approach, the assessment of the most prevalent physical symptoms in end of life stages, for example through the revised Edmonton Symptom Assessment Scale.16
ObjectiveTo perform the cultural adaptation and validation of a Portuguese version of the End of Life Comfort Planning Questionnaire in Palliative Care patients.
MethodsThis was a methodological study including translation, semantic and cultural adaptation, and evaluation of the psychometric properties, according to the guidelines proposed by Beaton et al.17 and STARD Reporting Guidelines.18 A research protocol was designed, analyzed and approved by the ethics committee of the institution where the study was conducted (authorization number CHSJ, CES 191-14, 14 November 2014). Participants were recruited at five in-patient medical-surgical settings (medicine, general surgery, vascular surgery, neurosurgery, pulmonology) and day hospital for chemotherapy from a central hospital in the north of Portugal. The sample was obtained after consecutive selection. The inclusion criteria were as following: Portuguese nationality, aged over 18 years old, and being followed by the palliative care team or under palliative chemotherapy. Exclusion criteria comprised cognitive impairment, lack of capacity to agree with the informed consent, and unclear diagnoses. The sample was consecutively recruited and participants were informed of the voluntary nature of their participation, they were given guarantees of data confidentiality and anonymity, and informed consent was obtained from each one.
The following stages composed the translation, semantic and cultural adaptation of the instrument:
- 1.
Linguistic translation of the instrument into European Portuguese by three translators, native in Portugal and fluent in American English. Two translators were unaware of the concepts under study, but the third one had theoretical, practical and research knowledge in palliative care and nursing;
- 2.
Synthesis of the first translation, by the three authors (SP, SC, JCM) (Translation Synthesis I – TS I);
- 3.
Review of the TS-I by the three translators. The final version was obtained from the second version (Translation Synthesis II – TS II);
- 4.
Back-translation of the TS II by two other translators, natives of the USA and fluent in Portuguese. They did the semantic analysis and had an agreement result of 100.0%;
- 5.
Review of all translations by a panel of experts (two in research and methodological studies, one expert in the Portuguese language, one expert in palliative care, one expert in the study of comfort and, also, all translators and back-translators). The Kappa of Cohen value was 0.88.
- 6.
Format the instrument according to the original;
- 7.
Assessment of face validity through a pre-test on a sample of 30 palliative care patients, in January 2015, which aimed to verify the understanding of the items, the ease of using the response set, the font size (given the specifics of the sample in question) and the response time. Although the instrument is designed to be a self-answered questionnaire, these patients had some difficulties because of weakness and/or cognitive deficits. It was decided to change to a form applied as an interview conducted by trained interviewers. No other changes were made. The instrument was easily understood, and the patients answered when requested. The average answer time was 8min for the entire questionnaire.
After the study of the face validity of the instrument, its psychometric properties were studied. Although the literature proposes the inclusion of 5–10 participants per item for the sample,19 there were several difficulties in recruiting participants for cultural and clinical reasons. Most Portuguese patients in end of life are referred to the palliative care teams at an advanced stage and, therefore, some patients were not in clinical conditions to participate. Regardless of this difficulty, the inclusion of five participants per item was estimated and the final sample was composed of 141 cancer patients in palliative care.
Data analysisData were analyzed using SPSS, version 23, for Windows. A critical significance value lower than 0.05 was assumed (p<0.05). The answers to the different items of the questionnaire were scored from 1 (Strongly Disagree) to 6 (Strongly Agree) after reversal of reversed items (items 2, 3, 8, 9, 13, 14, 15, 16, 18, 20, 21, 23 and 24).
ResultsParticipants’ characterizationAll 141 participants were recruited from acute medical-surgical settings in a central hospital in the north of Portugal (medicine, general surgery, vascular surgery, neurosurgery, pulmonology and day hospital for chemotherapy). All participants had an incurable, chronic and progressive illness and were in palliative care.
The average age was 59.97 years (SD=13.16 years, mode=66years, minimum=21 years and maximum=91 years). The majority of participants were male (60.60%), married (93.00%) and attended four years of school (54.20%). Although the vast majority were already retired (57.70%), a significant proportion of the participants (30.00%) had been working before the illness, and was on sick leave. With regard to spiritual/religious beliefs, 89.40% stated they were Catholic and 10.60% reported other spiritual or religious beliefs.
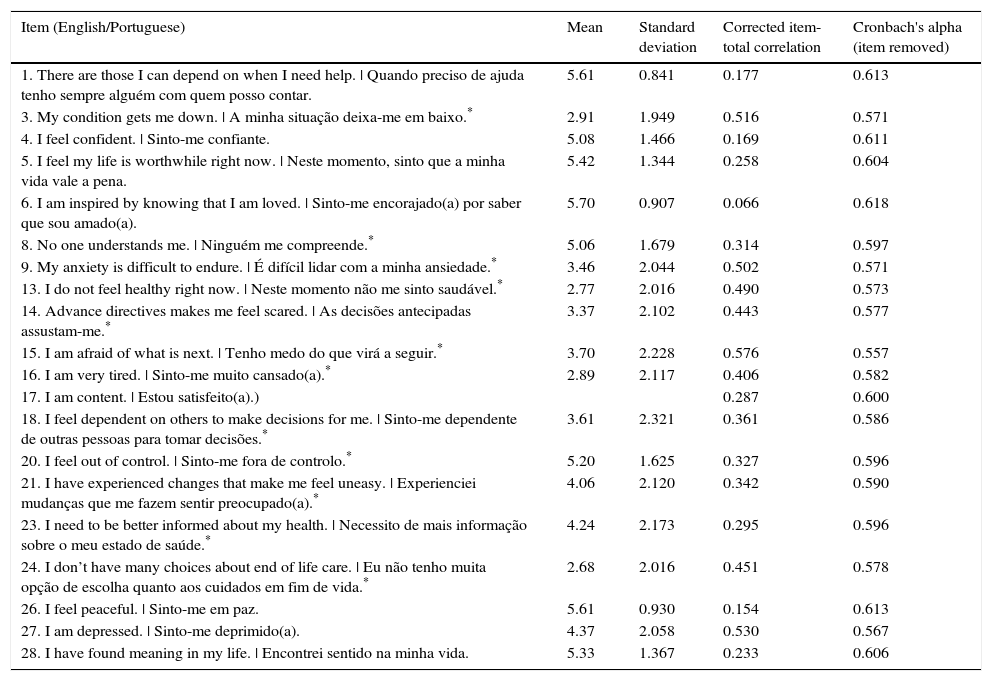
ReliabilityIn this study, the assumptions used in the original version were followed and internal consistency reliability was assessed, using Cronbach's alpha. According to the literature, alpha values under 0.50 are unacceptable, from 0.50 to 0–60 are questionable, from 0.60 to 0–70 are acceptable, from 0.70 to 0.80 are good, from 0.80 to 0.90 are very good, and over 0.90 are considered excellent.20,21 In a first analysis of internal consistency reliability (considering the 28 items of the scale), an alpha of 0.727 was obtained. This value, considered “good”, did not provide certainty concerning the internal consistency of the instrument, because some items had inverse correlations with the scale's overall score. For this reason, the items that scored negative correlations or very close to zero with the global score were successively removed. At the same time, the global alpha was analyzed when removing the items (Table 2), and after several hypotheses it was clear that items #2, 7, 10, 11, 12, 19, 22 and 25 were negatively influencing the global score, both in the value of alpha and in their correlation with the total.
Correlation matrix of items and value of alpha when items were removed.
| Item (English/Portuguese) | Mean | Standard deviation | Corrected item-total correlation | Cronbach's alpha (item removed) |
|---|---|---|---|---|
| 1. There are those I can depend on when I need help. | Quando preciso de ajuda tenho sempre alguém com quem posso contar. | 5.61 | 0.841 | 0.177 | 0.613 |
| 3. My condition gets me down. | A minha situação deixa-me em baixo.* | 2.91 | 1.949 | 0.516 | 0.571 |
| 4. I feel confident. | Sinto-me confiante. | 5.08 | 1.466 | 0.169 | 0.611 |
| 5. I feel my life is worthwhile right now. | Neste momento, sinto que a minha vida vale a pena. | 5.42 | 1.344 | 0.258 | 0.604 |
| 6. I am inspired by knowing that I am loved. | Sinto-me encorajado(a) por saber que sou amado(a). | 5.70 | 0.907 | 0.066 | 0.618 |
| 8. No one understands me. | Ninguém me compreende.* | 5.06 | 1.679 | 0.314 | 0.597 |
| 9. My anxiety is difficult to endure. | É difícil lidar com a minha ansiedade.* | 3.46 | 2.044 | 0.502 | 0.571 |
| 13. I do not feel healthy right now. | Neste momento não me sinto saudável.* | 2.77 | 2.016 | 0.490 | 0.573 |
| 14. Advance directives makes me feel scared. | As decisões antecipadas assustam-me.* | 3.37 | 2.102 | 0.443 | 0.577 |
| 15. I am afraid of what is next. | Tenho medo do que virá a seguir.* | 3.70 | 2.228 | 0.576 | 0.557 |
| 16. I am very tired. | Sinto-me muito cansado(a).* | 2.89 | 2.117 | 0.406 | 0.582 |
| 17. I am content. | Estou satisfeito(a).) | 0.287 | 0.600 | ||
| 18. I feel dependent on others to make decisions for me. | Sinto-me dependente de outras pessoas para tomar decisões.* | 3.61 | 2.321 | 0.361 | 0.586 |
| 20. I feel out of control. | Sinto-me fora de controlo.* | 5.20 | 1.625 | 0.327 | 0.596 |
| 21. I have experienced changes that make me feel uneasy. | Experienciei mudanças que me fazem sentir preocupado(a).* | 4.06 | 2.120 | 0.342 | 0.590 |
| 23. I need to be better informed about my health. | Necessito de mais informação sobre o meu estado de saúde.* | 4.24 | 2.173 | 0.295 | 0.596 |
| 24. I don’t have many choices about end of life care. | Eu não tenho muita opção de escolha quanto aos cuidados em fim de vida.* | 2.68 | 2.016 | 0.451 | 0.578 |
| 26. I feel peaceful. | Sinto-me em paz. | 5.61 | 0.930 | 0.154 | 0.613 |
| 27. I am depressed. | Sinto-me deprimido(a). | 4.37 | 2.058 | 0.530 | 0.567 |
| 28. I have found meaning in my life. | Encontrei sentido na minha vida. | 5.33 | 1.367 | 0.233 | 0.606 |
Those items were removed after a critical analysis by one of the authors of the original version, resulting in positive correlation between all items and with the global score and a Cronbach's alpha of 0.835, which is considered a very good value especially for new instruments.20,21
It was not possible to perform test–retest reliability due to the health condition of the participants. The fatigue and physical weakness of the majority of participants confirmed the decision to apply it as an interview, but this limited the possibility of undertaking a retest. Nevertheless, since the purpose of the instrument was to assess the immediate state of holistic comfort of the person at the end of life, the respect for human dignity always took precedence over the interests of the research.
Construct validityThe items that showed negative correlation with the global score of the scale may be adding a cultural bias and were removed with the author's permission (items #2, 7, 10, 11, 12, 19, 22 and 25) (Table 1). The concurrent validity, convergent-discriminant validity and also the principal component analysis confirmed the factors produced by the instrument and identified the items associated with each factor.
Concurrent validity. With regard to concurrent validity, the correlation between the instrument and another measure of the same concept was studied: Escala de Conforto Holístico HCQ - PT-DC©7 which is the Portuguese version of the Hospice Comfort Questionnaire–Patient.14 This Portuguese instrument was composed of 26 items and measures the holistic comfort in three dimensions: relief, ease and transcendence. However, as explained before, this instrument is not the most suitable to capture comfort of the Portuguese population in palliative care. Nevertheless, and because there is not in Portugal other measure to assess comfort of palliative care patients, we used this instrument as a criterion. In a first analysis a Spearman's correlation (ρ) of 0.74 (p=0.000) between the two questionnaires was obtained. The Escala de Conforto Holístico had a Cronbach alpha of 0.61,7 with items #8 and #13 contributing negatively to the global score and were removed from the analysis. Then a Cronbach alpha of 0.84 and correlation of 0.74 (p=0.000) was obtained. These inconsistencies validated the need for a different measure.
Convergent-discriminant validity. The items with factor loadings greater than 0.30 or lower than −0.30 were removed, since the original study is not absolutely clear on all procedures used.14 We then performed a principal components analysis with orthogonal rotation (varimax method with Kaiser normalization), according to the original version.
Although the instrument is one-dimensional, the taxonomic structure of comfort created by Kolcaba1 proposes the evaluation of three types of comfort (relief, ease and transcendence) in four contexts (physical, psycho-spiritual, social and environmental). The factor analysis was only studied by her on the original General Comfort Questionnaire, which had 48 items and was performed with acute care patients and community persons. This analysis excluded palliative care patients, and proposed a 3-factor solution which was consistent with the three types of comfort.1
The initial exploratory factor analysis of our study proposed six factors. This structure was, however, inconsistent with the theoretical organization of items and had no relationship with the Kolcaba's taxonomic structure nor a coherent conceptual point of view. However, the solution with five factors is aligned with the results of a qualitative study concerning comfort experiences in a sample of hospitalized patients in palliative care.22 The findings of this qualitative study highlighted five themes regarding physical, psychological, spiritual and social dimensions, and also environmental factors. Despite these considerations, the instrument remains unidimensional, which is why the organization in different factors serves to provide a better understanding of the instrument.
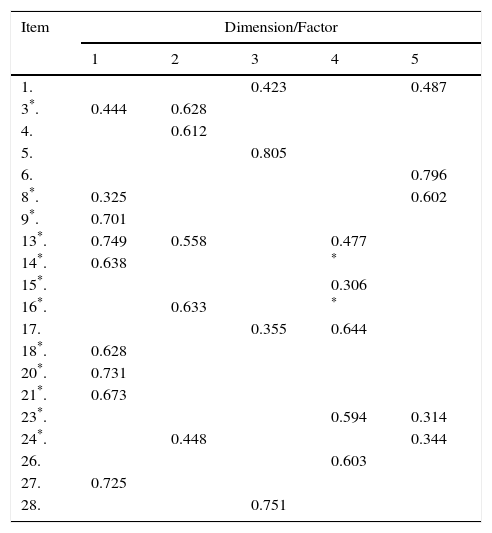
The rotation was forced to three, four and five factors and the factor structure with five factors was the one that presented the best correlations between the items and more consistency from a conceptual perspective (Table 3).
Principal components analysis with orthogonal rotation (varimax method with Kaiser normalization).
The high correlation between the majority of items with the dimension/factor to which they belonged (and not to others dimensions/factors) was a good indicator of convergent validity.
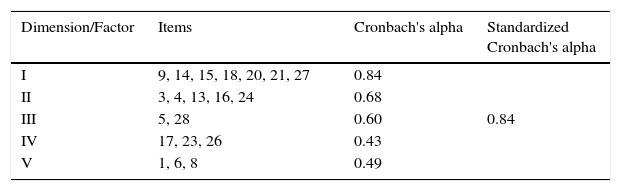
The factor analysis with five dimensions generates a variance of 57.307%, with alpha values between 0.43 and 0.84 (Table 4).
The matrix presented corrected item-total correlation values ranging between 0.59 and 0.678.
These values support the high correlation between almost all items of the questionnaire contributing, also, to a high alpha value (α=0. 835).
DiscussionRegarding the characteristics of the instrument, it was considered more appropriate to designate the Portuguese version as “Portuguese End of Life Spiritual Comfort Questionnaire”.
As stated by Kolcaba in her website,13 “comfort is a larger umbrella term compared to pain” and the discomfort caused by this symptom is “often a significant detractor from comfort”. In a holistic perspective, despite the physical origin of pain, comfort is greatly influenced by psychospiritual, sociocultural, and environmental factors, such as loneliness, fear, anxiety or noxious stimuli. Therefore, symptom management is an important goal of palliative care patients. For this reason, the additional evaluation of physical symptoms (not evaluated by the Portuguese End of Life Spiritual Comfort Questionnaire) should be considered. The use of the revised Edmonton Symptom Assessment Scale16 should be considered, as it is commonly used in this population for physical symptom assessment. In addition to these considerations, it is important to note that, in the development of comfort assessments, Kolcaba stated that “For clinical purposes, I prefer Verbal Rating Scales (“How would you rate your total comfort right now from 0 – 10?” 0 being no comfort at all, 10 being highest comfort possible in this situation.” Longer instruments (questionnaires) are most appropriate for research purposes (personal communication, 3.05.16).
Regarding the study of the translation and semantic adaptation of the End of Life Comfort Planning Questionnaire,13 there were no significant changes. Indeed, the items in the Portuguese version (Appendix 1) had very similar translations and meanings, and some were equal to those obtained from the validation of the Brazilian version beforehand.15 However the Portuguese and Brazilian population are different, not only regarding their language but also culturally which required a new validation. The semantic similarity supports the theoretical consistency of the instrument and the methodological rigor in the process of translation and back-translation.
The original versions of comfort instruments are intended to be used as self-administration questionnaires or interview questionnaires.14 It was found during the pre-test, particularly the study of face validity, that palliative participants had serious difficulties in completing the questionnaire. This is why it was decided to perform it as an interview, conducted by trained interviewers. Novak et al.14 also reported having to conduct their instrumentation study as an interview. This need was not found in the validation study in Brazil,15 despite the authors’ report on the participants’ conditions of advanced heart failure, as 60% had class II heart failure – slight limitation on exercise, which tends to disappear with rest – according to the classification proposed by the New York Heart Association. Another requirement was the reduction of items in the Portuguese version (Appendix 1), which did not happen in the Brazilian version, which remained with 28 items.15 In this study, the initial analysis of 28 items resulted in respectable alpha values (α=0.727), but the items were not consistent with each other and some of them had a negative correlation with the global score.
The palliative care movement is relatively recent in Portugal.23 Death or advance health care directives remains taboo subjects,24–25 which may explain why a great majority of Portuguese population refers not knowing what is palliative care (items #2, #7, #22, #25).26 Furthermore, the palliative Portuguese patient has the right to be accompanied by a relative or any other significant person for 24h.27 It is also common the patient to be in hospital wards with other patients, which may reduce their feelings of fear of loneliness (item #10).28,29 The vast majority of terminal patients could be under the effect of opioids and/or other sedative therapies that promote a state of relaxation (items #11, #12).12,30 The majority of participants were Catholic. These data are in line with the national profile and may justify the biased response to item #19 (“My faith helps me to be strong”). These data support the results of another study carried out in Portugal, with palliative care patients, in which the authors found that age, religious practice and education influence the experience of spirituality. In that study, the elderly and those with fewer academic qualifications tend to put their trust in God.31,32
However, this study has some limitations, and caution is needed when interpreting the results. Participants had incurable, chronic and progressive diseases and their clinical condition associated with a late referral to palliative care resulted in data collection difficulties. Thus we were limited the number of participants in the study, and could not perform test–retest reliability due to the health condition of the participants. The literature reports that studies with terminally ill patients, although difficult (for clinical and ethical reasons), are needed since they contribute to the development of knowledge and contribute to more efficient and effective practice and should be encouraged. The instrument especially important for research purposes. For clinical purposes the use of verbal rating scales is recommended, which is also holistic.
ConclusionSpiritual comfort is defined in this study as an immediate state and an outcome. It is a central concept in palliative care and, in this sense, should be measured holistically in order to obtain a larger and better assessment of the efficacy and effectiveness of the implemented interventions. Despite these considerations, there are few tools for its evaluation.
This study opens new perspectives for the evaluation of comfort as a holistic outcome and suggests the need for more studies with larger samples. It also suggests the usefulness of shorter instruments, taking into account the clinical characteristics and conditions of the person suffering from a terminal illness.
The Portuguese End of Life Spiritual Comfort Questionnaire represents a new approach to this important strategy of measuring a person's overall sense of wellbeing and meaningful life, we propose will should impacts on pain management effectiveness. Using this instrument in conjunction with a pain measure will give us important insight into spiritual comfort and its potential to decrease the amount of pain meds necessary when the patient has more spiritual comfort. The instrument has good psychometric properties and is reliable, valid and sensitive to the study of spiritual comfort of the person in the final stages of life, particularly for research purposes. It is a strong supplement to measures of physical symptoms.
Author's contributorsConception and design of the work, acquisition of data, or analysis and interpretation of data (Sara Pinto, Sílvia Caldeira, José Carlos Martins); Drafting the article or revising it critically for important intellectual content (Sara Pinto, Sílvia Caldeira, José Carlos Martins, Katharine Kolcaba); Final approval of the version to be published (Sara Pinto, Sílvia Caldeira, José Carlos Martins, Katharine Kolcaba).
Conflict of interestThe authors declare no conflicts of interest.
FundingSara Pinto received a grant from Nursing Order, North Section – Portugal (Research Grant Maria Aurora Bessa). The funding source had no such involvement in the study. For the remaining authors none were declared.
The authors acknowledge all translators and experts who have collaborated in the cultural adaptation of the instrument.
The following are the supplementary data to this article: