

Mental illnesses are rapidly escalating on university and college campuses. It is well known that post-secondary institutions are not doing enough to address mental health concerns: this represents a significant gap in our attempts to meet the mental health needs of young people. Deficits in mental health knowledge are now proposed as a major contributing factor to both stigma and low service access, but little research has explored this issue. There is also little research to date concerning what young people want to know about mental health and how best to disseminate mental health knowledge. Without such information, knowledge may not be shared in a person-centred, meaningful manner that youth will use. We explored these issues in the present study. First year postsecondary students (N = 271; n = 183 females; n = 85 males; n = 3 other) from Ottawa, Ontario, Canada participated in the online survey. Almost half of the post-secondary youth participants, particularly males, had difficulty recognizing common mental illnesses, such as anxiety, eating disorders, and psychosis. Youth held inaccurate beliefs and stigma, as well as attitudes not in favour of help-seeking. They primarily wanted to know about symptoms of mental illnesses as well as how to cope with stress. Post-secondary students wanted to learn about mental health issues through public presentations, the Internet, and media. The present research suggests the need for an awareness and acknowledgement among policy-makers of first year post-secondary students’ knowledge gaps and youth-appropriate knowledge sharing. Assessing mental health knowledge, what post-secondary students want to know about mental health, and knowledge transfer preferences could aid in the development of a framework to address the significant gap in the mental health needs of post-secondary students in a personcentred manner.
La enfermedades mentales se están disparando en las universidades y campus. Es bien sabido que las instituciones que acogen a los alumnos que han acabado secundaria no hacen lo suficiente para cubrir las necesidades en materia de salud mental de los jóvenes. Se dice ahora que las deficiencias en los conocimientos en salud mental constituyen un factor contribuyente de primer orden al estigma y al escaso acceso al servicio, a pesar de lo cual apenas se ha investigado el fenómeno. Tampoco se ha investigado apenas hasta la fecha lo que los jóvenes quieren saber sobre salud mental y de qué manera divulgar los conocimientos en salud mental. Sin esta información, los conocimientos no pueden compartirse de un modo que tenga sentido y se centre en la persona para que lo utilicen los jóvenes. En este trabajo exploramos estas cuestiones. En la encuesta online participaron estudiantes de Otawa que habían acabado hacía un año secundaria (N = 271, n = 183 mujeres, n = 85 varones, n = otros). A casi la mitad de los participantes, sobre todo varones, les resultaba difícil reconocer enfermedades mentales como la ansiedad, trastornos de alimentación y psicosis. Estos jóvenes mantenían unas creencias erróneas y estigma, así como actitudes reacias a buscar ayuda. Querían sobre todo conocer cuestiones sobre salud mental a través de presentaciones públicas, internet y los medios de comunicación. Este trabajo propone que se necesita conciencia y reconocimiento por parte de los poderes públicos de las lagunas que sufren estos alumnos y difundir los conocimientos adecuados a la juventud. Evaluar los conocimientos en materia de salud mental, lo que los estudiantes que han acabado secundaria quieren saber sobre salud mental y las preferencias en la transferencia de conocimientos podría ayudar a desarrollar un marco en el que abordar la gran laguna en necesidades relativas a salud mental de estos estudiantes teniendo en cuenta a la persona.
Mental health concerns are rapidly escalating on university and college campuses (Stanley & Manthorpe, 2001; Storrie, Ahearn, & Tuckett, 2010). Specifically, depressive symptoms, anxiety, eating disorders, and psychotic symptoms have doubled or tripled since the mid-1990s. Currently, up to 47% of students report experiencing symptoms of these significant concerns (Roberts et al., 2001; Storrie et al., 2010). First year, or the transition to post-secondary education, is an especially stressful time and risky for adolescent mental health (Lu, 1994). It is well-known that post-secondary institutions are not doing enough to address these mental health concerns, particularly during the major life transition year to university or college (Mental Health Commission of Canada MHCC, 2010; Storrie et al., 2010): This represents a significant gap in our attempts to meet the mental health needs of these youth.
Youth mental health is the oft-ignored “orphan” within the health care system (Kirby & Keon, 2006). Service shortages and stigma due to underfunding and a lack of education surrounding this health issue lead to poor longer term mental health outcomes; mental health issues, if not addressed early in life, threaten to bankrupt our health care system (Kirby & Keon, 2006). For every dollar spent on prevention, there is an eight-dollar cost savings (MHCC, 2010).
Recent research indicates that youth, such as university and college students, lack important mental health knowledge due to a lack of mental health education (Cotton, Wright, Harris, Jorm, & McGorry, 2006; Mond et al., 2007). In fact, up to 84% of post-secondary students meeting criteria for anxiety or depression do not access mental health services (Eisenberg, Golberstein, & Gollust, 2007). The lack of service access in post-secondary students is particularly associated with a lack of perceived need, being unaware of available services, and skepticism about treatment effectiveness (Eisenberg et al., 2007). Thus, mental health knowledge is limited in the post-secondary population despite the fact that most mental health concerns emerge between the ages of 15 and 24 years and significantly affect this group (Kessler et al., 2005). Specifically, 75% of mental health symptoms emerge by age 24 (Kessler et al., 2004). As the majority of North Americans attend some post-secondary education (Schulenberg & Maggs, 2002), understanding and addressing the student population is crucial: reducing delays between first onset of symptoms and treatment should be a priority for public policy to prevent poor achievement, employment, and social outcomes for these youth (Eisenberg et al., 2007). Post-secondary campuses present a venue where youth gather, where these young people could be reached to address mental health concerns in the early stages. However, the ways to effectively mobilize mental health knowledge to these youth are unknown. Without such information, knowledge cannot be shared in a person-centred, meaningful way. Therefore, gaining an understanding of mental health knowledge and youths’ own knowledge dissemination preferences will enhance efforts to address mental health concerns during this pivotal life period.
Mental Health LiteracyThe burden of mental illness is increasing in society and limitations in treatment resources available do not adequately account for this increase (Burns & Rapee, 2006; Michael & Crowley, 2002). Deficits in mental health knowledge, or “mental health literacy,” are now proposed as a major contributing factor to both stigma and low service access (e.g., Canadian Alliance on Mental Illness and Mental Health, 2007). Mental health literacy was a term first coined by Jorm et al. (1997, p. 187) to refer to “knowledge and beliefs about mental disorders which aid their recognition, management or prevention.” Mental health literacy includes the ability to accurately recognize specific disorders, knowledge about how to seek mental health information, attitudes that facilitate problem recognition and help-seeking, as well as knowledge and beliefs about risk factors and causes for mental illness, self-help interventions, and available professional help (Canadian Alliance on Mental Illness and Mental Health, 2007; Jorm et al., 1997). Some mental health literacy research has been conducted with youth to date.
Research has found that youth, including post-secondary students, often have difficulty identifying mental illnesses presented in case vignettes (Burns & Rapee, 2006; Cotton et al., 2006; Mond et al., 2007). Moreover, regarding the definition of mental health, research with over 10,000 youth in focus groups has found that only a minority of young people (20%) define mental health in a positive manner (Youth Net, 1998). Youth also hold negative attitudes toward treatment, with many believing that problems will continue despite treatment and that evidence-based treatments may not be beneficial or may even be harmful (Burns & Rapee, 2006; Goldney, Fisher, & Wilson, 2001; Mond et al., 2007). Thus, youth indicate that they are skeptical of the value of mental health specialists, as well as medications, and note that they would be more likely to pursue alternative self-help interventions, such as getting out and about more, taking vitamins and minerals, and pursuing special diets (Burns & Rapee, 2006; Mond et al., 2007). Such interventions may not always represent healthy or even beneficial alternatives. These findings highlight that youth are indeed in need of greatly enhanced mental health knowledge.
Group differences have also been found in youth mental health literacy. Female youth appear to be significantly more likely than young males to identify specific mental illnesses, such as depression, presented in vignettes (Burns & Rapee, 2006; Cotton et al., 2006). Male youth are also less likely than females to say that they would see a physician, psychologist, or counsellor for mental illness (Cotton et al., 2006). Given these findings, it would appear that gender may play an important role in mental health literacy and associated help-seeking behaviour. However, little research exists in this area, with no research for first year post-secondary students.
Knowledge MobilizationThere is no published research to date concerning what youth want to know about mental health and how best to disseminate mental health knowledge. A needs assessment of what youth want to know, and not just what they appear to need to know, is an essential component of knowledge mobilization (Health Canada, 2002) – a component which has been ignored in youth mental health literacy research. It is also important to examine preferences concerning knowledge mobilization, as the method through which knowledge is disseminated is thought to only have a positive impact and maximize utilization of knowledge if it is consistent with the receivers’ preferences (Cunningham et al., 2008). Therefore, post-secondary students’ preferences for knowledge mobilization methods must be assessed in order for mental health awareness efforts to effectively reach their targets.
Assessing mental health literacy, what youth want to know about mental health, and knowledge mobilization preferences will aid in the development of a framework to address the significant gap in the mental health needs of first year post-secondary students.
Goals & ContributionsGiven the gaps in the existing literature, the goal of the present study was to assess: 1) mental health literacy, 2) what youth want to know about mental health, and 3) preferences concerning knowledge mobilization.
The present research is the first to explore knowledge mobilization needs among youth, which should help to maximize utilization of information by the target audience. Moreover, the measure used in this study was the first to involve youth input in development of a mental health literacy questionnaire, which should enhance research reliability and the resultant service improvement (Armstrong, 2009; Young & Armstrong, 2012). It is also the first to examine mental health literacy for a higher risk transition population for mental health concerns: first year post-secondary students. Moreover, the current research is also the first to examine what youth want to know about mental health so that we may determine what types of knowledge certain youth may be receptive to. In the longer term, the present study acts as a springboard to provide a rationale for a national study. In the shorter term, this research provides some initial insight concerning mental health literacy and knowledge mobilization in first year post-secondary students.
MethodSample & ProcedureFirst year post-secondary students (N = 271, n = 183 females, n = 85 males, n = 3 other) participated in the online survey. The ethnic distribution included participants from the following groups: 61% White, 13% Asian, 9% Arab, 8% Black, 4% Mixed Racial, 2% Aboriginal, 3% Other. Students came from the following academic programs: 30% Science, 24% Social Science, 22% Health Science, 3% Commerce, 9% Arts, 2% Law, 1% Engineering, 8% Other (including non-full time students).
All participants who completed the survey were enrolled in first-year classes at the University of Ottawa, in Ontario, Canada. Convenience sampling was used: participants were recruited within first-year university classes after a brief presentation explaining the study. Participants provided informed consent and were made aware of ethical approval from the University of Ottawa Research Ethics Board. Students could complete the survey at their leisure. There was no time limit; however, it was expected that participation would take 60minutes. After completion of the survey, participants were provided with an information sheet of mental health resource centers on campus and in the community.
MeasureThe Mental Illness Awareness and Transfer of Information Preferences Survey (MIAtips; Armstrong, Robertson, Young, & Tahir, 2012) was used in the present research. The questionnaire is an internet-based survey designed collaboratively with youth, but heavily grounded in literature and DSM-IV-TR (APA, 2004) diagnostic criteria. Both open-ended and closed-ended forced choice questions are included in this measure.
Like past mental health literacy research (e.g., Jorm, 1997), youth are also presented with scenarios about a “friend” meeting diagnostic criteria for Major Depression, an Anxiety Disorder, an Eating Disorder, and Psychosis. Following each scenario, participants are then given an open-ended question: “What, if anything, is going on with your friend?” Responses can be categorized into: 1) correct identification of the specific presented mental illness, 2) identification that the person has a mental illness (general response), or 3) no reference to mental illness. Attitudes and stigma toward mental illness are also measured and can be examined in relation to correct identification of mental illnesses and youth knowledge preferences. Specifically, following each scenario, participants are presented with a series of five items, measuring stigma or inaccurate attitudes that are common myths, assessed from strongly disagree to strongly agree. For example, “This is a sign of personal weakness;” “Most people our age experience this.” Internal consistency reliability in the standardization sample for these 5 items was averaged at .72 for each of the scenarios (ranging from .71 to .73), which is considered to be adequate, based on Hunsley and Mash (2008) criteria. In the standardization sample, correct identification of mental illnesses and low stigma or accurate attitudes also demonstrated convergent validity with having a close friend or family member who has been diagnosed with a mental illness (Young & Armstrong, 2012).
Youth preferences about receiving certain types of mental health knowledge and the methods through which young people want that information delivered to them are also assessed. Assessing what youth want to know about mental illness and how they want that information shared with them is the key way in which this survey differs from past research. More specifically, young people are asked whether they would like to know about symptoms of mental illness, how to cope with stress, community mental health services, different options for therapy, self-help techniques, and how to help someone who might be suicidal. The MIAtips also includes an open-ended opinion question about “good ways to share mental health knowledge” with young people. A closed-ended question follows in which young people can endorse preferred ways to learn about mental health, mental illness, and mental health services. Young people rank order these means of knowledge mobilization from 1 to 13, with 1 being perceived as the most helpful: online, health promotion campaigns, community health services, books, classes, friends, family, public presentations by professionals, presentations by people who have a mental illness, through music, through television, through billboard ads, through print media.
Statistical AnalysesData screening and cleaning, and all statistical analyses, were carried out with SPSS-PSAW 19.0 Statistical Package. SPSS Frequencies were used to calculate percentages of youth endorsing the various mental health literacy and knowledge mobilization items. A one-way Analysis of Variance (ANOVA) by gender and correlational analyses were also carried out. Results were considered to be significant at p < .05.
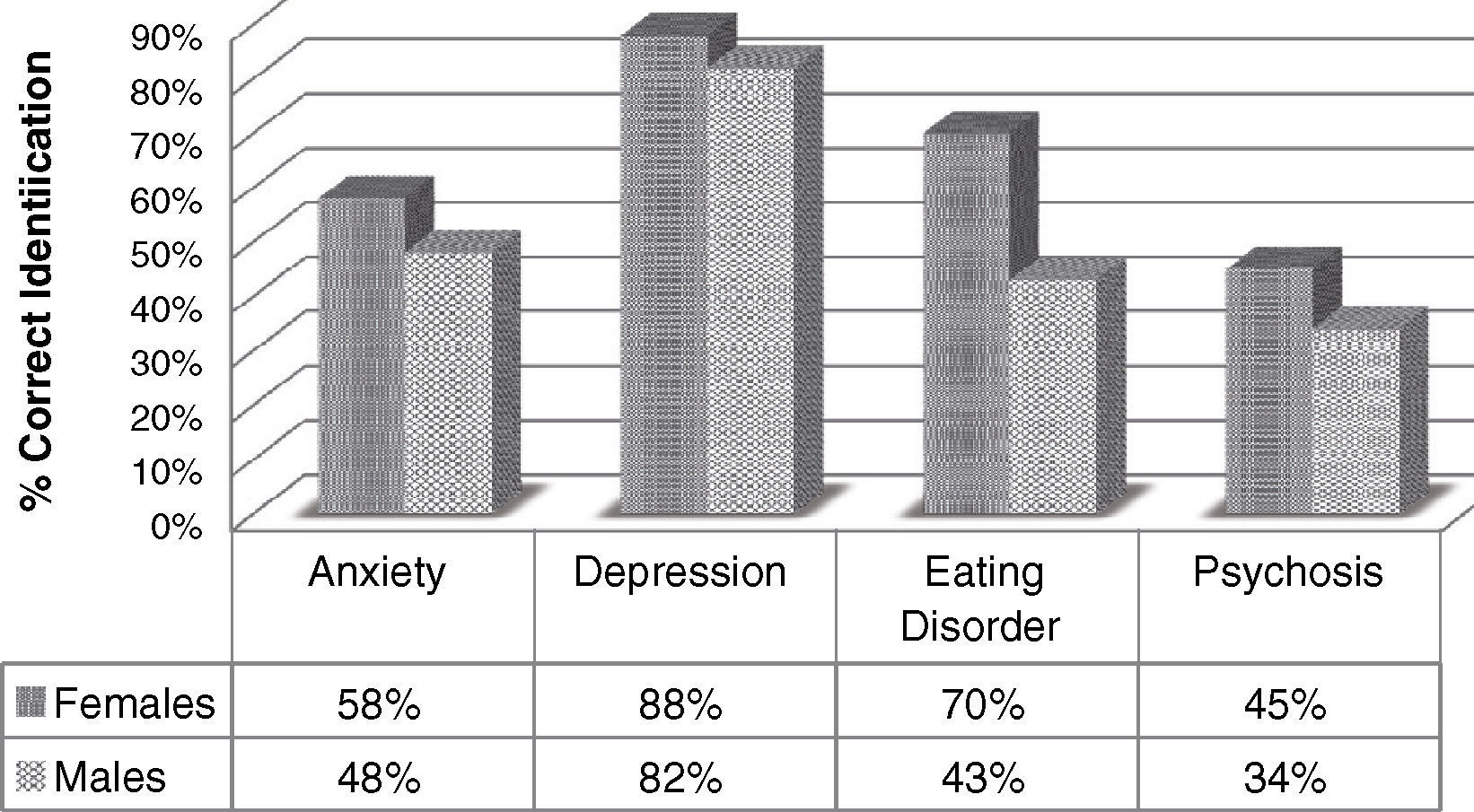
ResultsMental Health LiteracyResponse frequencies can be found by gender in Figure 1. As noted in the figure, depression was the most correctly identified mental illness for both genders. A one-way ANOVA yielded gender differences in the identification of all presented mental illnesses, with females correctly identifying significantly more concerns than males: Anxiety, F(1, 270) = 14.76, p < .001; Depression, F(1, 270) = 8.61, p = .003; Eating Disorder/Anorexia, F(1, 270) = 119.48, p < .001; Psychosis/Schizophrenia, F(1, 270) = 17.68, p < .001. Bivariate correlations demonstrated that correct identification of mental illnesses was inversely associated with inaccurate perceptions and stigma toward mental illness: Anxiety, r = -.23, p < .001; Depression, r = -.25, p < .001; Eating Disorder/Anorexia, r = -.31, p < .001; Psychosis/Schizophrenia, r = -.16, p < .001. Inaccurate attitudes and stigma were significantly associated with attitudes not in favour of help-seeking, r = .32, p < .001.
What Youth Want to Know About
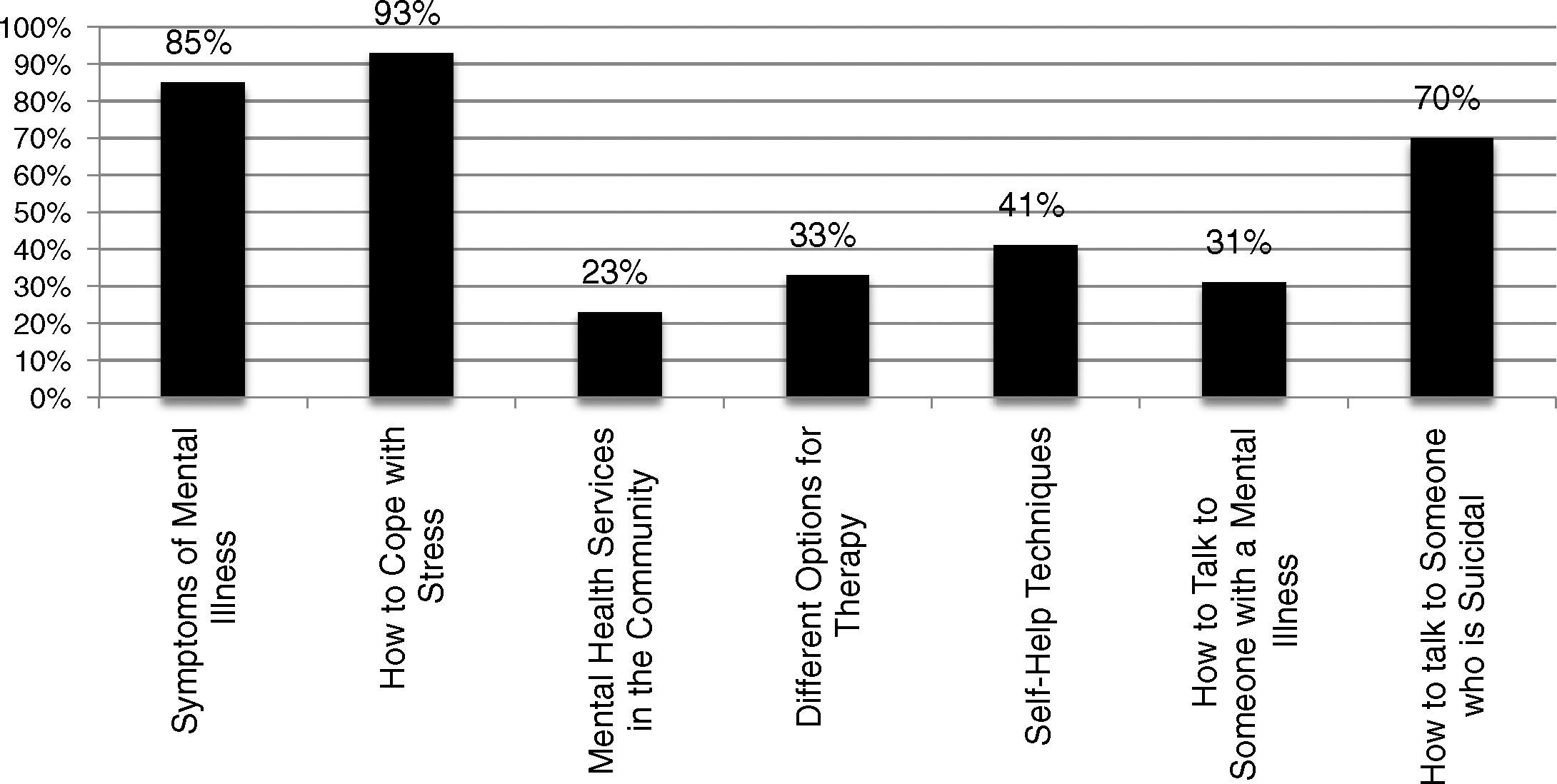
What youth want to know about mental health is presented in Figure 2. Questions were asked in a Yes/No format. “Yes” responses are presented in the figure. The majority of youth respondents wanted to know about how to cope with stress, symptoms of mental illness, and how to talk to someone who is suicidal. The majority of respondents expressed that they do not want to learn about mental health services in the community, different options for therapy, how to talk to someone with a mental illness, and self-help techniques for symptoms of mental illness.
Preferred Knowledge Mobilization Methods.")
Respondents were asked an open-ended question concerning the method by which they would like to learn mental health information. Youth indicated that they wanted to learn about mental health through: large-group/classroom presentations by professionals or those with lived experience (21%), small-group interactive presentations (20%), online (14%), music lyrics or video material (13%), and books or other print material (7%). The remainder of the youth suggested a variety of alternate knowledge mobilization methods or did not provide a suggestion.
DiscussionWith the exception of depressive symptoms, first year post-secondary youth were fairly poor at recognizing symptoms of common mental illnesses, such as anxiety, eating disorders, and psychosis. In particular, males had more difficulty identifying mental illnesses than females. Likely given poor recognition of symptoms, first year youth do not express an interest in learning about community mental health resources or self-help techniques: they potentially do not believe such services are helpful for, or targeted at, them. In fact, those who did not recognize symptoms of common mental illnesses generally held stigmatized and inaccurate attitudes toward those with mental illness. They also did not hold beliefs in favour of self or other help-seeking.
Prochaska's Transtheoretical Model of Behavioural Change suggests that before a person contemplates healthy change, they have to recognize that there is a problem (Prochaska & DiClemente, 2005). In the “precontemplation” phase of their model, people have no intention of taking action and may not recognize that there is a problem. This theory fits the present findings. Consistent with previous mental health literacy research, a lack of service access in post-secondary students is particularly associated with a lack of perceived need (Eisenberg et al., 2007). Before one can teach youth about available mental health services, the present research findings extend beyond the existing mental health literacy literature to suggest that youth need to learn about symptoms of common mental illnesses first. Myths and inaccurate attitudes also need to be countered. Teaching about symptoms of common mental illnesses is fortunately consistent with first year post-secondary students’ stated knowledge learning preferences. Only after first year post-secondary students learn about symptoms of common mental illnesses and recognize that they themselves may be experiencing these concerns, might they move to the “contemplation” phase of Prochaska's model – Should I seek help? Following this self-awareness, it would be time to share knowledge about available community mental health services or self-help techniques.
To share mental health information with first year post-secondary youth, it is helpful to present information in a way that is consistent with the receivers’ preferences (Cunningham et al., 2008). In the current study, youth suggest that they would prefer information to be shared with them through both traditional and non-traditional methods. More specifically, they would primarily appreciate classroom-based presentations or information presented through the Internet or other media (e.g., music, video).
The present research suggests the need for an awareness and acknowledgement among policy-makers of first year post-secondary students’ knowledge gaps and youth-appropriate knowledge sharing. Expert, stakeholder, and post-secondary institution partnerships would be beneficial in the development of appropriate knowledge mobilization protocols. If stakeholders are not involved in designing services that affect them, resultant services can fail to meet their needs (Amsden & VanWynsberghe, 2005). As resources for mental health education are limited within the funding system, it is imperative that protocols be appropriate and effective. Acknowledging limitations that this is the first study to explore mental health knowledge needs and mobilization preferences with a single sample, the current findings suggest youth-friendly knowledge sharing mediums and topics that may meet first year post-secondary students’ mental health literacy needs.
Given the existing knowledge gaps, myths or inaccurate beliefs, and attitudes not in favour of help-seeking found in the present study, it would appear that there is an urgent need to enhance mental health literacy in first year post-secondary students. This group of students is particularly vulnerable to mental health concerns and, compounding the problem, the majority of those with symptoms do not seek help (Eisenberg et al., 2007; Lu, 1994). With enhanced knowledge shared in a person-centred manner, and likely resultant increased help-seeking, we can hope to decrease the risk for academic, future career, and interpersonal problems due to untreated symptoms of mental illness.
Conflict of InterestThe authors of this article declare no conflict of interest.
Financial SupportThe authors would like to acknowledge the Ontario Mental Health Foundation and the Provincial Centre of Excellence for Child & Youth Mental Health for supporting this research.
