



Research into the adoption of technological innovations often evaluates the features that users engage with when using these innovations (Leal & Albertin, 2015; Perez, 2006; Perez & Zwicker, 2010). In this research, we identified the internal factors affecting the adoption of a technological innovation, as defined by information systems (IS) in healthcare, the electronic health record, and evaluated the results of adoption for individuals and groups using this system. We opted for a study in a hospital in Porto Alegre-Rio Grande do Sul, with mother and child specialties. Quantitative techniques were selected, questionnaires with users of the electronic health record, physicians, administrators, nurses, and technicians. We used a multivariate statistical technique of structural equation modeling, using the statistical software SmartPLS®. The survey results indicated that some internal variables to the health sector, such as communication, the participatory process and the form of decision for innovation can contribute effectively to the adoption of technological innovations. The proposed model also served to evaluate the results achieved with the adoption of this IS, which is realized through the following: the introduction of new processes; improvement of the existing ones; easier access to patient information, and creating new solutions for customers. Before the system, these were not possible to implement.
The search for process improvement and the increase in the supply of new products and services in various market sectors has led to different sizes of organizations and in different sectors, including healthcare, to invest increasing amounts in the acquisition of information systems (IS) and information and communication technologies (ICT). However, as advocated by Perez and Zwicker (2010) as important as investing, is managing IS/ICT resources.
In the case of modern IS, its use has become increasingly intense and it has taken different work groups to work collaboratively toward a common goal, which was hardly possible to achieve in centralized systems (Larsen & McGuire, 1998). Health is a typical example of this situation, since professionals, such as doctors, nurses, laboratory technicians, and social workers, can use the IS for information or to provide the IS with the central point that their mission is to save lives.
Healthcare has adopted several innovations introduced by IS, among which stands out the electronic health record (EHR), or electronic medical records, or the electronic patient record, which is the target of this study in innovation. This system provides a substantial number of benefits, which include better patient care, the centralization of information and the reduction in costs (Bowman, 2013).
Most studies about the EHR discuss the dimensions of the quality of the data provided by the system, such as completeness, accuracy, consistency, and plausibility (Weiskopf & Weng, 2013), or the possibility of obtaining gains with the implementation of this type of system (Bowman, 2013). However, the deployment and adoption of this type of system should take into account, in addition to the factors related to the system itself, the various factors related to the internal structure of the organization. Beyond the question of the integration of its various users and teams, healthcare also benefits from the EHR in improving operational and strategic results (Perez & Zwicker, 2010).
Rogers (2003) argues that the adoption of technological innovations, as in the case of the EHR, is associated with the assessment, on the part of users, of aspects that show its contribution to the work process or to the organization, as well as internal organizational factors. However, these internal organizational factors, as well as the results obtained with the adoption of a technological innovation, have not been prevalent in studies on the adoption of innovation, which focus more on the perception of users (Perez, 2006; Rogers, 2003), including in the area of health.
There are few studies on the adoption of innovations, as defined by the adoption of IS in the health area in Brazil. A contribution of this study to the advancement of knowledge about the adoption of technologies is the possibility of evaluating an organization's internal variables that favor the adoption of an innovation, which could pave the way for the proposal of other variables, beyond those indicated by Rogers (2003), contributing to the adoption of innovations of a technological nature in health and other areas.
Considering this argument, this study formulated the following research question: which internal factors favor the adoption of the EHR in a healthcare organization? The overall objective of the study was to identify the key internal factors that favor the adoption of EHR as a technological innovation in healthcare. Specific objectives were to identify the results achieved by the adoption of the EHR in terms of improvements of processes, products and services, and to validate a structural model to assess the adoption of the EHR.
Theoretical frameworkICT and knowledge management are relatively recent, emerging in Brazil in the 1970s in computer and telecommunications users and in the mid-1980s at the business schools of Brazil (Albertin & Albertin, 2005). According to these authors, it is regarded as one of the most important components of the current business environment, at both the strategic and operational levels.
To Laurindo (2002), the concept is more comprehensive than the concepts of data processing, IS, software engineering, information technology, and the set of hardware and software. It also involves human, administrative and organizational aspects. Generally speaking, a collection of computer systems used by the organization is called information technology, or IT (Turban, Volonino, & Wood, 2013).
To Turban et al. (2013), an IS is a system able to collect, process, store, analyze, and disseminate information to suit a particular purpose. Like any system, an IS includes entries (data and instructions) and outputs, such as reports and calculations (O’Brien & Marakas, 2013) and also encompasses people, procedures and physical facilities, and operates in a particular environment (Turban et al., 2013).
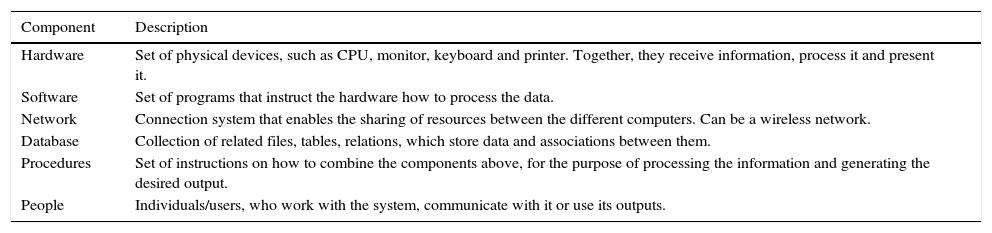
Although an IS is not necessarily an operation based on computers, many of the IS found in a modern organization are computer-based (Turban et al., 2013). The authors present an IS of six components (Table 1), with the caveat that not all IS include all of these components and that an IS has a purpose and a social context.
The six components of an information system.
| Component | Description |
|---|---|
| Hardware | Set of physical devices, such as CPU, monitor, keyboard and printer. Together, they receive information, process it and present it. |
| Software | Set of programs that instruct the hardware how to process the data. |
| Network | Connection system that enables the sharing of resources between the different computers. Can be a wireless network. |
| Database | Collection of related files, tables, relations, which store data and associations between them. |
| Procedures | Set of instructions on how to combine the components above, for the purpose of processing the information and generating the desired output. |
| People | Individuals/users, who work with the system, communicate with it or use its outputs. |
Laudon and Laudon (2013) argue that, from the perspective of a company, an IS is an organizational and administrative solution that takes ICT to face the challenges proposed by the environment, such that the manager needs to know the broader dimensions of organization, administration and information technology systems and their ability to provide solutions to the challenges and problems in the field.
Use of systems and information technology in healthcareShortliffe and Blois (2014) indicate that medical informatics or biomedical informatics is a fast-developing scientific field that deals with storage, retrieval and use of information, data and biomedical knowledge for problem solving and decision-making. The main areas of medical informatics are: health IS; electronic patient records; telemedicine; decision support systems; biological signal processing; medical image processing; internet in health, and the standardization of health information.
According to Raitoharju and Laine (2006), the acceptance of IS/ICT is one of the critical success factors for the achievement of the expected benefits from the investments made in this type of technology. These authors emphasize that, despite several studies on the acceptance of IS/ICT, very little is known about the factors which affect the process of adoption by health professionals of this type of technological innovation. The effective implementation and use of this type of technology in healthcare require multi-professional cooperation, as well as the involvement of doctors, nurses, social workers, and other professionals.
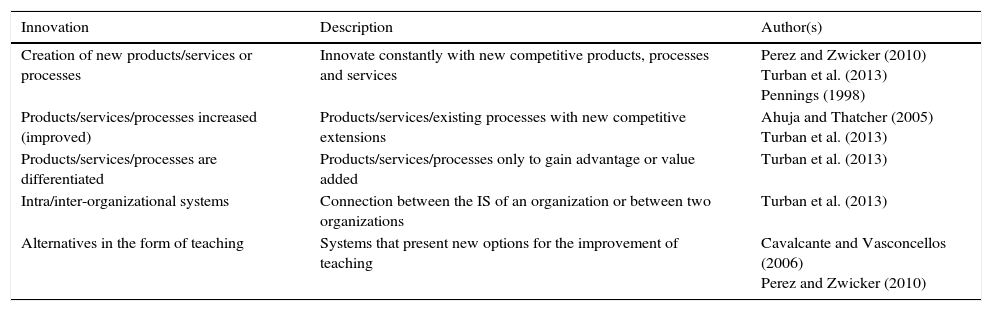
Results of the use of information systems and technologiesVarious authors (Table 2) have identified numerous internal improvements and results obtained with the introduction of the IS/ICT in the business world, in several segments. The results range from the improvement of the processes, products and services that exist, to the creation of new products that reach the market.
Results obtained by the use of an information system.
| Innovation | Description | Author(s) |
|---|---|---|
| Creation of new products/services or processes | Innovate constantly with new competitive products, processes and services | Perez and Zwicker (2010) Turban et al. (2013) Pennings (1998) |
| Products/services/processes increased (improved) | Products/services/existing processes with new competitive extensions | Ahuja and Thatcher (2005) Turban et al. (2013) |
| Products/services/processes are differentiated | Products/services/processes only to gain advantage or value added | Turban et al. (2013) |
| Intra/inter-organizational systems | Connection between the IS of an organization or between two organizations | Turban et al. (2013) |
| Alternatives in the form of teaching | Systems that present new options for the improvement of teaching | Cavalcante and Vasconcellos (2006) Perez and Zwicker (2010) |
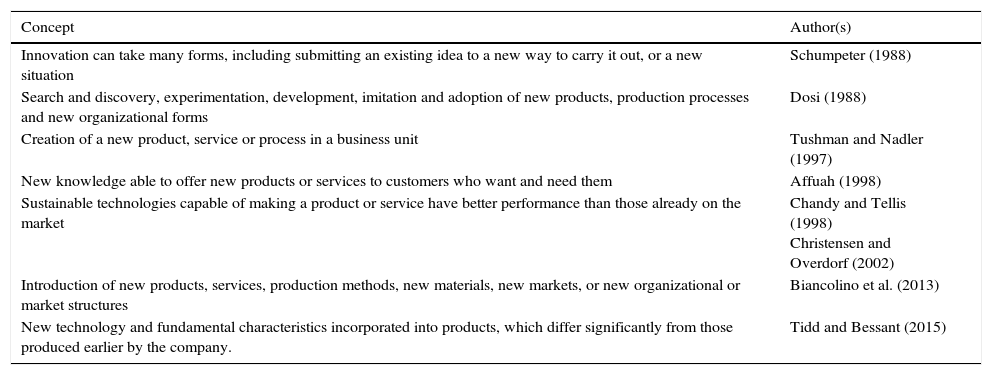
For Tidd and Bessant (2015) to talk about innovation is essentially to talk about change. Burgelman, Christensen, and Wheelwright (2004) supplement that by saying that innovation generally refers to changes in technology. Some recommendations, according to Drucker (2004), are essential for innovation: (a) innovation is conceptual and perceptual; (b) to be effective, it should be simple and punctual; (c) effective innovations begin modestly and try to accomplish something specific; (d) a successful innovation aims at leadership; (e) it must be intentional and systematic, and (f) must begin with the meticulous analysis of the sources of opportunities.
Tushman and Nadler (1997) are alert to the fact that innovation applied to product, service or process should be seen as a way to compete in dynamic environments living with continuing technological changes. Schumpeter (1988) indicates that innovation can take many forms; it is not necessary to invent something new, or even submit an existing idea to a new way to perform it or a new situation. Innovation involves the introduction of new products, services, production methods, new materials, new markets, and new organizational or market structures (Biancolino, Maccari, & Pereira, 2013).
Another interesting concept is presented by Christensen and Overdorf (2002) and Chandy and Tellis (1998), which combines innovation with sustainable technologies, able to make a product or service which has a better performance than those already on the market, leading consumers to seek this differentiator. Table 3 presents a summary of the key concepts of innovation found.
Innovation concepts.
| Concept | Author(s) |
|---|---|
| Innovation can take many forms, including submitting an existing idea to a new way to carry it out, or a new situation | Schumpeter (1988) |
| Search and discovery, experimentation, development, imitation and adoption of new products, production processes and new organizational forms | Dosi (1988) |
| Creation of a new product, service or process in a business unit | Tushman and Nadler (1997) |
| New knowledge able to offer new products or services to customers who want and need them | Affuah (1998) |
| Sustainable technologies capable of making a product or service have better performance than those already on the market | Chandy and Tellis (1998) Christensen and Overdorf (2002) |
| Introduction of new products, services, production methods, new materials, new markets, or new organizational or market structures | Biancolino et al. (2013) |
| New technology and fundamental characteristics incorporated into products, which differ significantly from those produced earlier by the company. | Tidd and Bessant (2015) |
As shown, several authors conceptualize innovation as a new product, service or process, or new ways to perform procedures or produce goods or services, including the technological aspect. These concepts are applicable to the target innovation of this study: the EHR used in a healthcare institution.
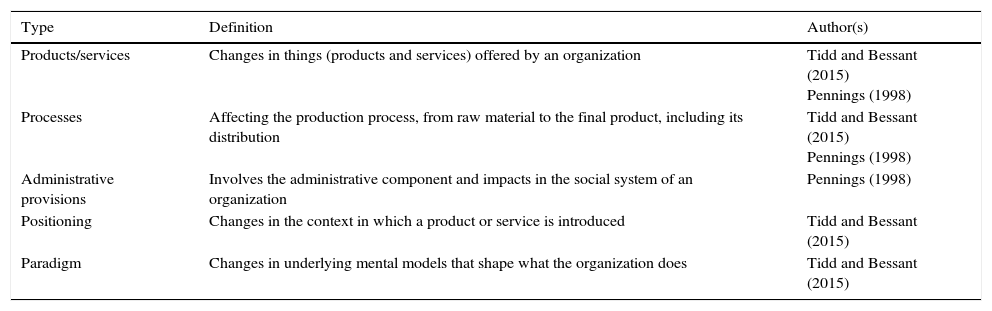
Several authors present different types or categories of innovation. Tidd and Bessant (2015) emphasize that, when speaking about innovation, the essential approach should be based on the change, which can take various forms. These authors present four broad categories (the ‘4Ps’ of innovation): innovation in products/services, innovation, innovation processes, and innovation of positioning paradigm. Pennings (1998) classifies innovation into three distinct types: products, services and administrative processes. Table 4 presents a summary of the types of innovation.
Types of innovation.
| Type | Definition | Author(s) |
|---|---|---|
| Products/services | Changes in things (products and services) offered by an organization | Tidd and Bessant (2015) Pennings (1998) |
| Processes | Affecting the production process, from raw material to the final product, including its distribution | Tidd and Bessant (2015) Pennings (1998) |
| Administrative provisions | Involves the administrative component and impacts in the social system of an organization | Pennings (1998) |
| Positioning | Changes in the context in which a product or service is introduced | Tidd and Bessant (2015) |
| Paradigm | Changes in underlying mental models that shape what the organization does | Tidd and Bessant (2015) |
The innovation process should be divided into two stages: the stage of innovation and the generation stage of adoption/diffusion (De Vries, Bekkers, & Tummers, 2014). The diffusion of an innovation is the process of its communication in a given social context involving individuals and groups, often members of an organization. In turn, the adoption of an innovation is also a process in which individuals and groups decide upon its use (full adoption) as the best course of action available (Rogers, 2003). The consideration of adoption can be rejection, i.e., when the decision is for non-adoption.
According to Rogers (2003), the theory of diffusion of innovation began to be developed in the 1930s. Rogers (2003) indicates that the diffusion of an innovation is a kind of social communication, in which the messages are related to new ideas, or the process by which an innovation is communicated over time, through certain channels, between the various members of a social system.
The way in which an innovation is adopted depends directly on the perceived attributes of this innovation by its users (Perez & Zwicker, 2010; Rogers, 2003). Rogers (2003) points out five intrinsic attributes of innovation affecting adoption: comparative advantage, compatibility, complexity, experimentation, and observability, which explain between 50% and 80% of the variance in the rate of adoption. Larsen and McGuire (1998) argue that these attributes are universal for studies of adoption of innovations. In practical terms, these attributes affect the behavior of individuals as they are perceived by individuals who use technological innovation (Moore & Benbasat, 1991).
The perceived attributes of innovation as mentioned above have received more extensive investigation by authors, with predominantly quantitative research (Leal & Albertin, 2015; Perez & Zwicker, 2010). However, other variables, such as those inherent in the domestic context of Non-Governmental Organizations, have received attention from researchers in the processes of adoption and diffusion of innovation (Perez & Zwicker, 2010; Rogers, 2003).
In addition to these five variables (attributes), Rogers (2003) features four other variables related to the context of an organization, which can be useful for explaining the add-on of the variance of the rate of adoption not explained by the attributes previously presented:
- 1.
the type of decision for innovation: the way in which an innovation is decided can be optional, collective or authoritarian. The more people involved in the decision-making process of an innovation, the slower its adoption rate.
- 2.
the nature of the communication channels: relates to forms of communication used in the various stages of the diffusion process. Communication channels can be individual or mass (face to face).
- 3.
the nature of the social system: internal standards, leadership and the degree of internal network connection of communication are determining factors in the diffusion of an innovation.
- 4.
role of the promoter of change: the relevance of a promoting agent of change (champion) in promoting efforts to disseminate innovation, since generally only 3–16% of individuals adhere to new ideas (changes).
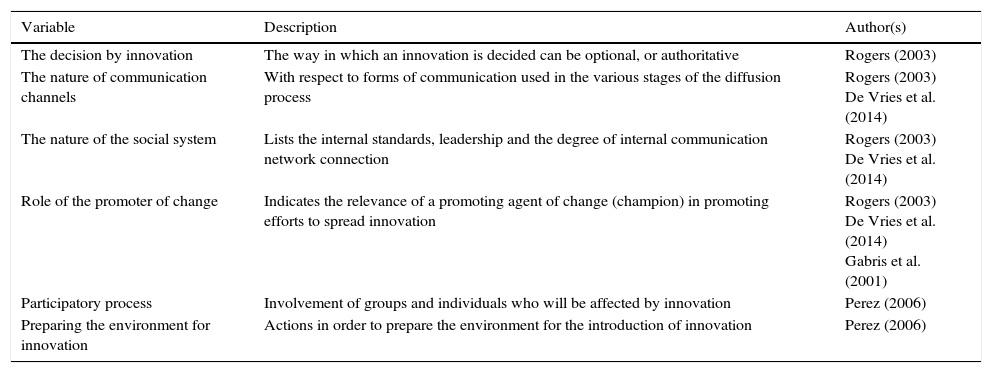
In a study in the public sector, De Vries et al. (2014) identified the following variables related to the organizational level: availability of resources; leadership styles; risk aversion; clarity of goals; conflicts, and organizational structure. The variables identified by the authors used in this research are the three variables with meanings equivalent to Rogers's (2003) study, i.e., leadership styles, clarity of goals, and organizational structure, which equate to performance of agent of change, nature of communication channels, and nature of the social system, respectively. Leadership also featured in the study by Gabris, Golembiewski, and Ihrke (2001).
When assessing the internal context of healthcare institutions, Perez (2006) identified two additional variables relating to the internal organizational environment of organizations that can affect the adoption and the consequent use of a technological innovation: (1) the participatory process that involves groups and individuals affected by innovation, and (2) preparation of the environment for innovation that will be introduced. Table 5 presents a summary of the internal organizational environment variables.
Internal organizational environment variables.
| Variable | Description | Author(s) |
|---|---|---|
| The decision by innovation | The way in which an innovation is decided can be optional, or authoritative | Rogers (2003) |
| The nature of communication channels | With respect to forms of communication used in the various stages of the diffusion process | Rogers (2003) De Vries et al. (2014) |
| The nature of the social system | Lists the internal standards, leadership and the degree of internal communication network connection | Rogers (2003) De Vries et al. (2014) |
| Role of the promoter of change | Indicates the relevance of a promoting agent of change (champion) in promoting efforts to spread innovation | Rogers (2003) De Vries et al. (2014) Gabris et al. (2001) |
| Participatory process | Involvement of groups and individuals who will be affected by innovation | Perez (2006) |
| Preparing the environment for innovation | Actions in order to prepare the environment for the introduction of innovation | Perez (2006) |
The gap in research addressing the influence of variables of the external context with respect to the adoption of technological innovations is developed in this study. Based on Tables 2 and 5, the following hypothesis were formulated to be tested with respect to the adoption of the EHR:H1 The decision type significantly affects innovation adoption/use of EHR. Communication channels significantly affect the adoption/use of EHR. The nature of the social system significantly affects the adoption/use of EHR. The promoter of change significantly affects the adoption/use of EHR. A participatory process significantly affects the adoption/use of EHR. Preparing for change significantly affects the adoption/use of EHR. Adoption/use positively affects the EHR results of use (processes and services).
It is important to emphasize that the authors surveyed point factors and attributes that affect the adoption of an innovation (Perez & Zwicker, 2010; Rogers, 2003), or factors/attributes that affect the adoption or use of a technological innovation in IS/ICT (Moore & Benbasat, 1991). This study adopted the term ‘adoption/use’ as indicated by recent authors in research involving IS for use in healthcare.
Innovation and institution targets of researchThe electronic health recordAccording to Turban et al. (2013), the EHR can be classified as one IS that allows users (doctors, nurses, social workers, and managers) to collect, process, store, and analyze information to serve a specific purpose, namely, to provide a better service to their patients. The EHR is a planned system to receive all data from a patient, in an integrated manner and that can be used in several of the steps in the care of a patient, starting with reception in the office, clinic, or emergency room, to being discharged after attendance (Bowman, 2013).
An EHR also assists various healthcare professionals in their daily activities, which are related to a more organized form of work, new forms of patient care, faster access to information, centralization of information, as well as the use of legacy data that can be used in future research, healthcare statistics and, mainly, in medical diagnostic aid (Perez, 2006).
The hospital: HO-RSFor reasons of confidentiality, the location of the health research will be referred to as HO-RS. The HO-RS is located in Porto Alegre-Rio Grande do Sul, with mother and child specialties. Currently, it takes private patients and was created in the mid-1950s. In the early 1980s, the HO-RS became the regional center for serving high-risk pregnant women, enjoying a privileged position in the ranking of hospitals run by the health plan with INAMPS (Brazilian National Institute of Medical and Social Assistance). In 1991, assigned to the Ministry of Education and Culture, the hospital was administered by the Federal School of Medical Sciences of Porto Alegre, until 1995.
At the end of the 1990s, discussions began in defense of decentralization and of maintaining the public character of the HO-RS, relying on political mobilization and union representation in the area of health. In March 2000, a technical committee was appointed to support the discussion on the persuasion toward the municipalization of the hospital. Through an agreement signed in August 2000 between the Ministry of Health and the City of Porto Alegre, the HO-RS came under municipal management. The specialties of the HO-RS are gynecology, obstetrics, psychiatry, and pediatrics.
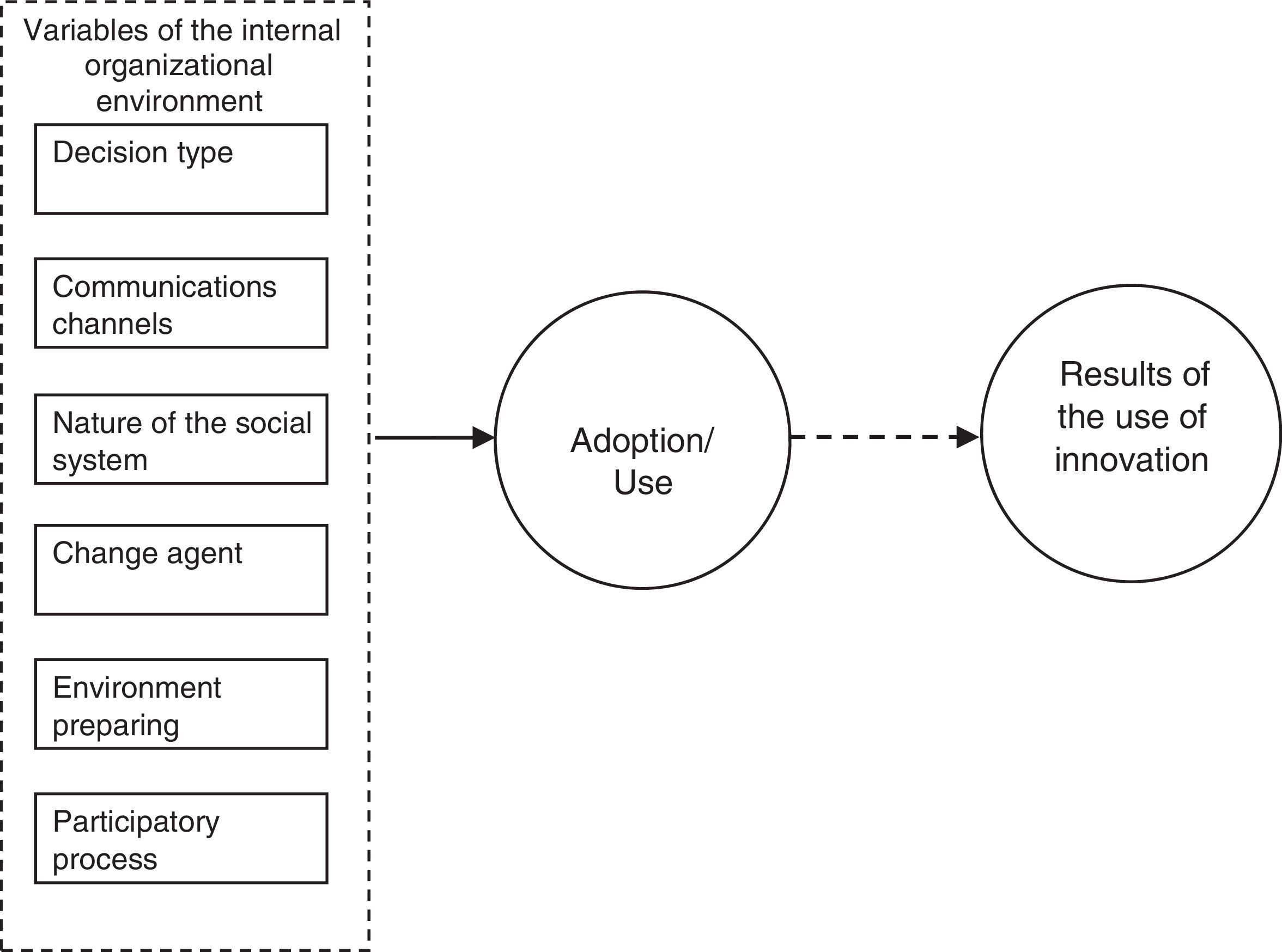
Methodological proceduresBased on the propositions of the problem and the research objectives, we proposed a structural model of research, which can be observed in Fig. 1, that synthesized the diffusion process of a technological innovation as proposed by Rogers (2003). It can be observed that the social context of internal factors of organizations affect the adoption of an innovation process: the type of decision for innovation; communication channels used to communicate innovation; the nature of the internal social system, and the effort of the promoting agent of change, complemented by two factors suggested by Perez (2006), which are participatory process and preparation of the environment for innovation.

To validate the proposed research schema in Fig. 1, we defined ‘results of the use of technological innovation’ as the dependent variable. The independent variables were represented by set of six ‘variables of internal organizational environment’. In Fig. 1, the variable ‘adoption/use of innovation’ (EHR) is a mediator between the internal organizational environment variables and the results of the use of innovation variable, which justifies the proposition of the structural model.
When the variables studied are related to complex concepts (internal organizational environment, adoption/use of technological innovation, and results of use), the use of constructs or latent variables can facilitate educational and reflective understanding of these concepts. According to Hair, Anderson, Tatham, and Black (2010), the constructs can be understood as theoretical concepts to be used by researchers, which can be defined in abstract terms, but cannot be measured directly.
In the proposed model, it should be noted that variables related to internal organizational environment were developed from Table 5 and variables related to the results of the use of technological innovation have been developed as indicated in Table 2. We can see from this picture that the results obtained by the use of an IS can be achieved by creating and offering new products, services and processes, as well as the improvement of those that already exist, in addition to the possibilities of new administrative processes and new intra/inter-organizational processes. Adoption/use variables were defined from the current use and intent to intensify the use of the EHR, as indicated in Table 6.
Variables use/adoption of electronic health record.
| Use/Adoption of innovation | Variable |
|---|---|
| I consider myself an intensive user of the electronic health record | US1 |
| As soon as possible I want to use the electronic health record more intensively | US2 |
| In general, I believe that the institution uses the electronic health record satisfactorily | US3 |
The sample used was the non-probability type for convenience, because of the difficulties and physical limitations of ensuring the application of a probability sampling technique. For sample size, recommendations adopted Hair et al. (2010) indicate that the number of respondents should be at least eight times the number of study constructs, which in this case is eight, as shown in Fig. 1.
The data collection instrument adopted was a questionnaire with closed questions. A scale of Likert-type agreement of seven points, one being the minimum level and seven the maximum level of agreement. Once we knew that there was no scale like this in existence, we decided to develop a scale suited to the goals of the research. For validation purposes, the questionnaire was reviewed by five experts, after which a pre-test was carried out with seven users of the system, and we requested feedback after completion.
Techniques for data analysisThe multivariate analysis technique called structural equation modeling was used, conducted by the partial least squares (PLS) method. The PLS method is suitable for the restrictive conditions imposed by the data in this research. The conditions presented by Chin (2000) in which the PLS should be considered, are highlighted below and occurred in the research: (a) the theoretical model involves latent variables; (b) for non-standard data; (c) sample size is small, and (d) indicators are training.
The choice of SmartPLS® software Version 3.0 was made on the basis of the structural model proposed in Fig. 1. The term structural equation modeling designates a family of related procedures (Kline, 2005). For this author, other terms, such as covariance structure analysis and modeling of the covariance structure, are also used in the literature to sort these various techniques together in a single technique.
According to Byrne (2001), when working with techniques of structural equations, it is recommended that the distinction is made between exogenous and endogenous latent variables. Latent exogenous variables are synonymous with independent variables, since they cause fluctuations in the value of other latent variables in the model. Changes in the value of the exogenous variables are not explained by the model. They are influenced by factors external to the model (Byrne, 2001). Already, the endogenous latent variable is as dependent on or results in at least a causal relationship (Hair et al., 2010). The endogenous latent variable is a synonym of the dependent variable, being affected by an exogenous variable in the model, either directly or indirectly (Byrne, 2001).
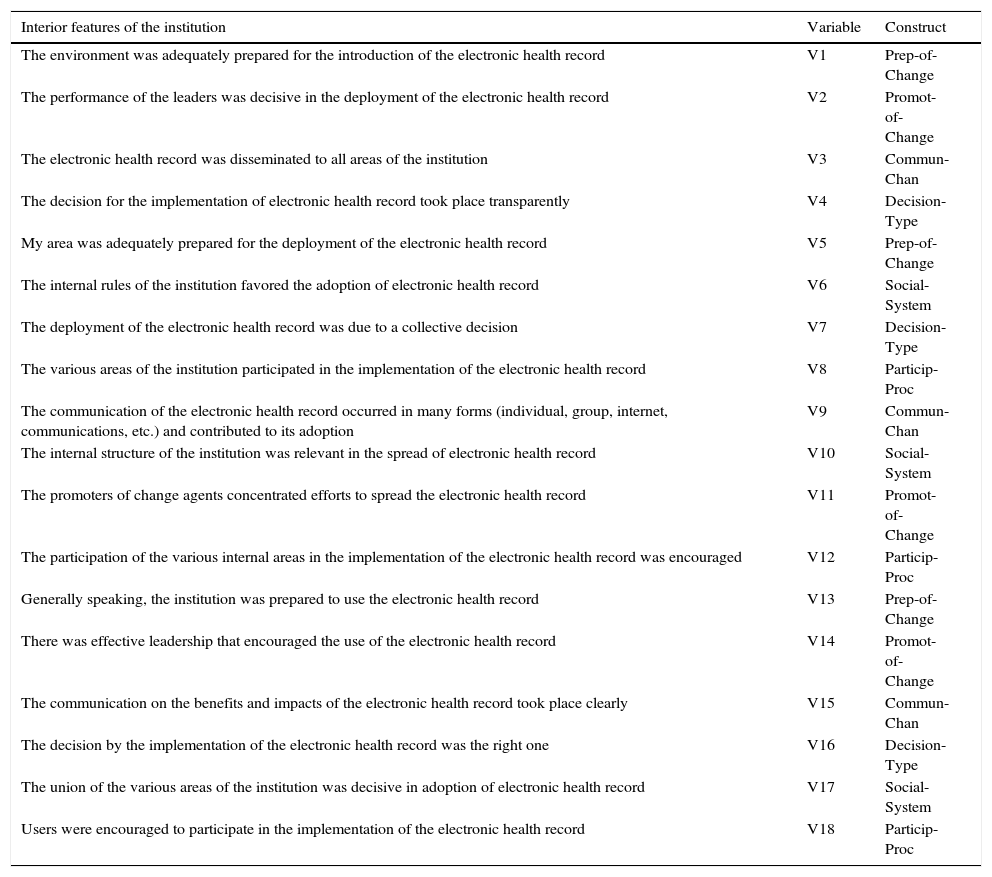
Procedures for quantitative analysis of the resultsThe pre-processing of the data gave us the ‘debugging’ (screening date), in order to treat omitted values, values outside of the expected range (outliers), and linearity of the data obtained. Then the analysis of the measurement model took place, which consisted of assessing the validity of the convergence of the structural equation model. Finally, the structural model validation was carried out. The variables used in the model were obtained by the measurement probes of the questionnaire used in the data collection. Such variables are identified in Tables 6–8.
Internal organizational environment variables.
| Interior features of the institution | Variable | Construct |
|---|---|---|
| The environment was adequately prepared for the introduction of the electronic health record | V1 | Prep-of-Change |
| The performance of the leaders was decisive in the deployment of the electronic health record | V2 | Promot-of-Change |
| The electronic health record was disseminated to all areas of the institution | V3 | Commun-Chan |
| The decision for the implementation of electronic health record took place transparently | V4 | Decision-Type |
| My area was adequately prepared for the deployment of the electronic health record | V5 | Prep-of-Change |
| The internal rules of the institution favored the adoption of electronic health record | V6 | Social-System |
| The deployment of the electronic health record was due to a collective decision | V7 | Decision-Type |
| The various areas of the institution participated in the implementation of the electronic health record | V8 | Particip-Proc |
| The communication of the electronic health record occurred in many forms (individual, group, internet, communications, etc.) and contributed to its adoption | V9 | Commun-Chan |
| The internal structure of the institution was relevant in the spread of electronic health record | V10 | Social-System |
| The promoters of change agents concentrated efforts to spread the electronic health record | V11 | Promot-of-Change |
| The participation of the various internal areas in the implementation of the electronic health record was encouraged | V12 | Particip-Proc |
| Generally speaking, the institution was prepared to use the electronic health record | V13 | Prep-of-Change |
| There was effective leadership that encouraged the use of the electronic health record | V14 | Promot-of-Change |
| The communication on the benefits and impacts of the electronic health record took place clearly | V15 | Commun-Chan |
| The decision by the implementation of the electronic health record was the right one | V16 | Decision-Type |
| The union of the various areas of the institution was decisive in adoption of electronic health record | V17 | Social-System |
| Users were encouraged to participate in the implementation of the electronic health record | V18 | Particip-Proc |
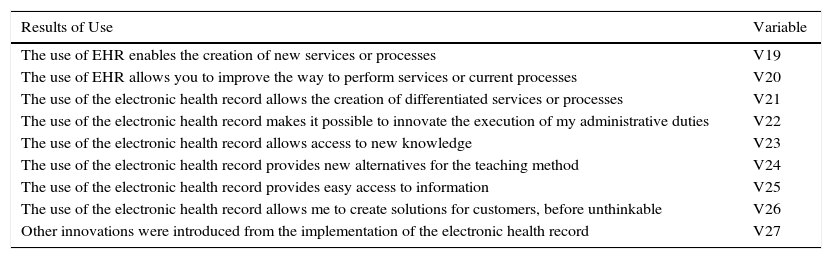
Variables related to the results of use.
| Results of Use | Variable |
|---|---|
| The use of EHR enables the creation of new services or processes | V19 |
| The use of EHR allows you to improve the way to perform services or current processes | V20 |
| The use of the electronic health record allows the creation of differentiated services or processes | V21 |
| The use of the electronic health record makes it possible to innovate the execution of my administrative duties | V22 |
| The use of the electronic health record allows access to new knowledge | V23 |
| The use of the electronic health record provides new alternatives for the teaching method | V24 |
| The use of the electronic health record provides easy access to information | V25 |
| The use of the electronic health record allows me to create solutions for customers, before unthinkable | V26 |
| Other innovations were introduced from the implementation of the electronic health record | V27 |
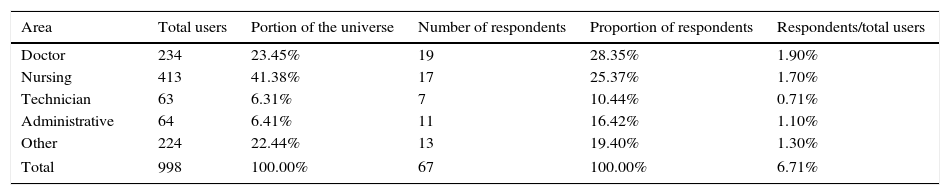
Data collection took place during the second half of 2011 and the first half of 2012. A total of 75 questionnaires were gathered, of which 67 were considered valid. The sample met the requirements singled out by Hair et al. (2010), which recommend at least eight respondents for each construct studied (Fig. 2). The profile of the universe to which the questionnaire was sent and the total number of respondents is presented in Table 9.

Participants of the sample – HO-RS.
| Area | Total users | Portion of the universe | Number of respondents | Proportion of respondents | Respondents/total users |
|---|---|---|---|---|---|
| Doctor | 234 | 23.45% | 19 | 28.35% | 1.90% |
| Nursing | 413 | 41.38% | 17 | 25.37% | 1.70% |
| Technician | 63 | 6.31% | 7 | 10.44% | 0.71% |
| Administrative | 64 | 6.41% | 11 | 16.42% | 1.10% |
| Other | 224 | 22.44% | 13 | 19.40% | 1.30% |
| Total | 998 | 100.00% | 67 | 100.00% | 6.71% |
We decided not to carry out a separate study of the different functional areas in view of the small number of respondents (67 or 6.71%). In light of this limitation, there is an imbalance between the respondents: 28.35% from the medical field; 25.37% from nursing, and 10.44% from the technical area. However, it is necessary to observe that the first two areas had the larger number of users.
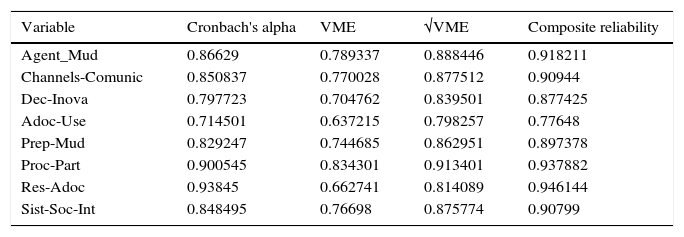
Analysis of the measurement model – internal organizational environment – HO-RSIn Table 10, it can be observed that the values obtained of Cronbach's alpha is greater than 0.7, which is the value of cut recommended by the literature (Hair et al., 2010). Satisfactory values have also been found to the average variance explained (VME>0.5) and composite reliability, which had values greater than 0.6, as recommended by Tenenhaus, Vinzi, Chatelin, and Lauro (2004).
PLS processing indicators – internal organizational environment – HO-RS.
| Variable | Cronbach's alpha | VME | √VME | Composite reliability |
|---|---|---|---|---|
| Agent_Mud | 0.86629 | 0.789337 | 0.888446 | 0.918211 |
| Channels-Comunic | 0.850837 | 0.770028 | 0.877512 | 0.90944 |
| Dec-Inova | 0.797723 | 0.704762 | 0.839501 | 0.877425 |
| Adoc-Use | 0.714501 | 0.637215 | 0.798257 | 0.77648 |
| Prep-Mud | 0.829247 | 0.744685 | 0.862951 | 0.897378 |
| Proc-Part | 0.900545 | 0.834301 | 0.913401 | 0.937882 |
| Res-Adoc | 0.93845 | 0.662741 | 0.814089 | 0.946144 |
| Sist-Soc-Int | 0.848495 | 0.76698 | 0.875774 | 0.90799 |
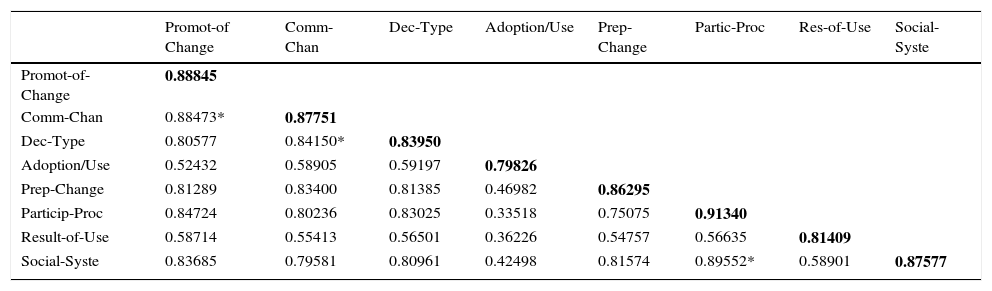
For a better explanation of the results obtained by the structural equation modeling, we placed them on the diagonal from Table 11 (the correlation between the latent variables), the values of the square root of the VME of Table 10. Tenenhaus et al. (2004) recommend that the value of the square root of VME must be greater than the correlations between variables (all the values of the rows and columns) in which they are located. This procedure, called discriminant validity, aims to test whether the studied variables should be grouped or not.
Correlations between latent variables – internal organizational environment – HO-RS.
| Promot-of Change | Comm-Chan | Dec-Type | Adoption/Use | Prep-Change | Partic-Proc | Res-of-Use | Social-Syste | |
|---|---|---|---|---|---|---|---|---|
| Promot-of-Change | 0.88845 | |||||||
| Comm-Chan | 0.88473* | 0.87751 | ||||||
| Dec-Type | 0.80577 | 0.84150* | 0.83950 | |||||
| Adoption/Use | 0.52432 | 0.58905 | 0.59197 | 0.79826 | ||||
| Prep-Change | 0.81289 | 0.83400 | 0.81385 | 0.46982 | 0.86295 | |||
| Particip-Proc | 0.84724 | 0.80236 | 0.83025 | 0.33518 | 0.75075 | 0.91340 | ||
| Result-of-Use | 0.58714 | 0.55413 | 0.56501 | 0.36226 | 0.54757 | 0.56635 | 0.81409 | |
| Social-Syste | 0.83685 | 0.79581 | 0.80961 | 0.42498 | 0.81574 | 0.89552* | 0.58901 | 0.87577 |
The values assigned (*) in Table 11, note three cases (rows) in which the correlation between the variables showed slightly higher results (0.82%, 0.24% and 2.20%) to the value of the square root of VME. As the differences identified are small, we decided to keep the template without modification, however, without compromising the rigor of validity. An alternative to the refinement of validation would be removing the observable variables (one by one) that present values of high correlations in the two constructs (latent variables).
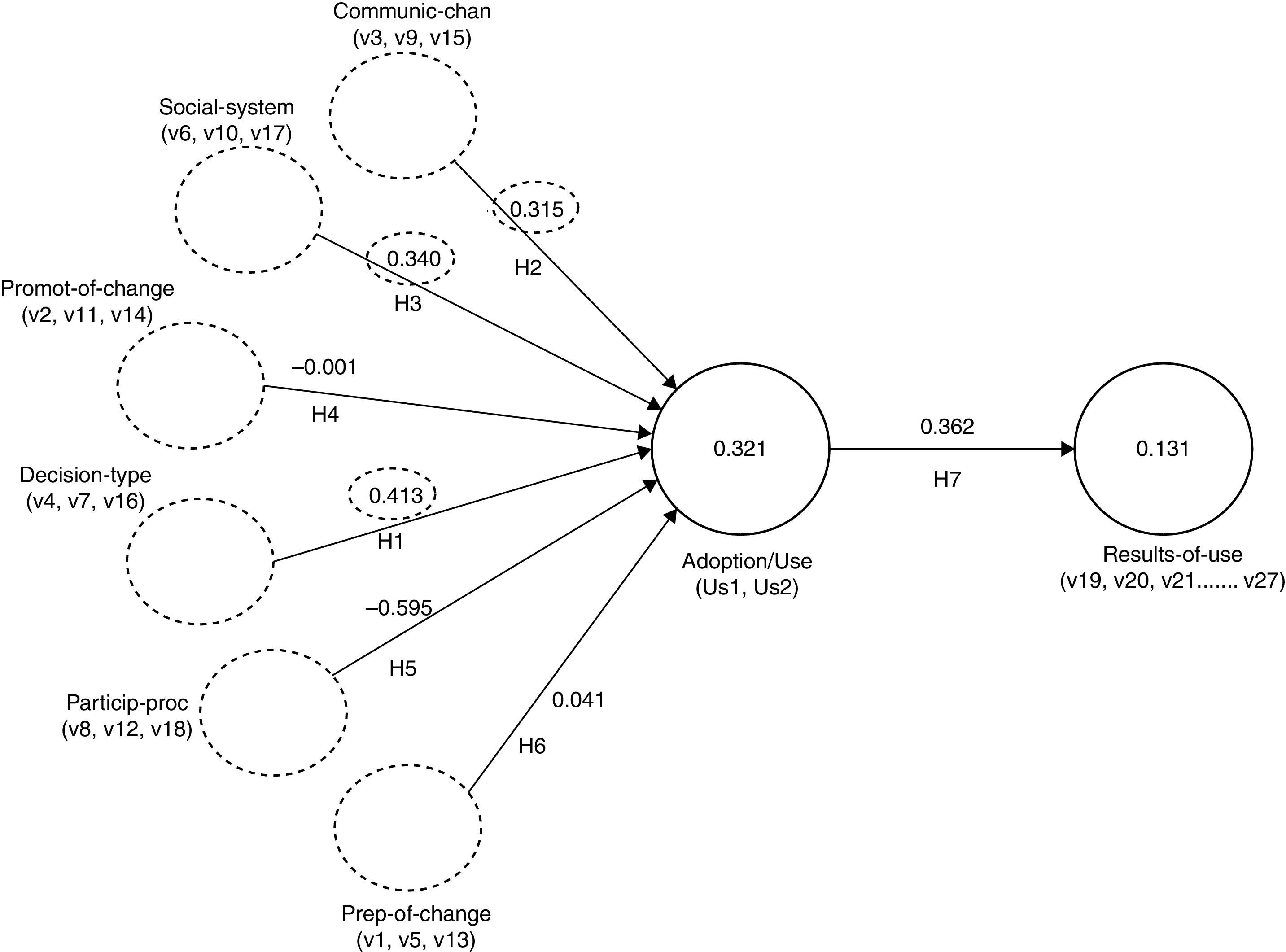
The calculated values are in Fig. 2 in the processing of the model proposed by the research, for the variables related to factors of internal organizational environment, using the PLS technique.
Validation of the structural model – internal organizational environment – HO-RSIn Fig. 2 it can be seen that the associated regression coefficients between the latent variables (Promot-of-Change, Communic-Chan, Decision-Type, Prep-of-Change, Particip-Proc, Social-System) and how they impact on the latent variable Adoption/Use, as well as how this affects the latent variable, adoption results (Result-of-Use). The standardized regression coefficients indicate how much each construct affects latent variables, when these increase by one unit. Outstanding latent variables are marked with a dashed ellipse in Fig. 2. The decision by innovation variable presents the greater coefficient of regression (0.413), that is, when the usage variable increases by one unit, the largest contribution to that change comes from the decision by innovation variable. In turn, the Adoption/Use presents a regression coefficient equal to 0.362 in relation to the adoption results variable (Result-of-Use).
Fig. 2 also shows that the standardized regression coefficients of the change agent (Promot-of-Change) and participatory process (Particip-Proc) variables present negative values (−0.001 and −0.595). These results are evidence that, apparently, in the implementation of EHR in HO-RS, there was no RS concern to appoint agents of change in the involvement of future users of the system, a counterpoint to Gabris et al. (2001), Rogers (2003) and Perez (2006). There are also the values of the coefficients of determination of the variance (R2 inside the circles) of dependent variables (Adoption/Use and Result-of-Use), denoting the percentage of variance of the dependent variable that is explained by the independent variables.
For the variable Adoption/Use, the value of the variance coefficient of determination (R2) was 32.1%, in agreement with Rogers (2003), which draws attention to the fact that context variables also contribute to the adoption of a technological innovation. The other perceived attributes in an innovation of 50% to explain 80% (Perez & Zwicker, 2010; Rogers, 2003).
In the case of the result of the use variable, the value of the variance coefficient of determination (R2) obtained was 13.1%, indicating that, as users adopt/use an innovation, this usage is producing results in the processes of the everyday life of an organization, as defined by Tidd and Bessant (2015). In this case, the results are represented by the variables v19–v27. For the institution studied, the most significant results concern new processes and services created by the adoption of the EHR, as well as the improvement in administrative processes and access to new knowledge (Pennings, 1998; Turban et al., 2013). It was noted also that other innovations were introduced from the implementation of the EHR. The results underscore the importance of the adoption of this technology in the area of health, which has the purpose of saving lives.
For the validation of the structural model, the bootstrapping algorithm of the software SmartPLS® was run with 300 parameters for the number of cases and samples, with the objective of realizing 300 simulations with the dataset to obtain the test results of Student's t distribution. The t test results depend on the number of questionnaires answered. For a sample of 67 respondents (or degrees of freedom), the value of the distribution t of Student is 1.99 for a confidence interval of 95% and 0.05 significance, as can be verified in Bussab and Morettin (2003). The results of the t test were obtained in respect of the implementation of the bootstrapping algorithm in the SmartPLS®.
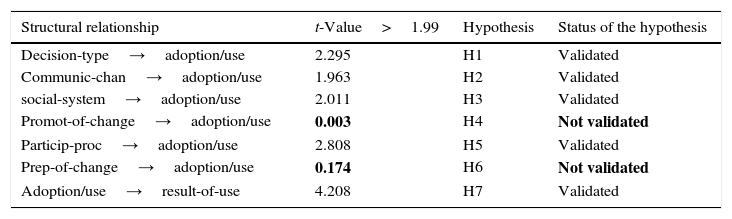
Student's t test is used to test the hypothesis that the correlation/regression coefficients are equal to zero. If the result of the t test is equal to or greater than 1.99, the hypothesis is rejected, that is, the correlation/regression is significant. It was noted (Table 12) that the Promot-of-Change and Prep-of-Change presented values for the t test much lower than 1.99, so they should be removed from the initial model. The other variables showed values close to or exceeding 1.99 and were kept in the model. A new process without Promot-of-Change and Prep-of-Change affected very little (third decimal place) the new coefficients calculated for the remaining variables.
Validation of assumptions – internal organizational environment – HO-RS.
| Structural relationship | t-Value>1.99 | Hypothesis | Status of the hypothesis |
|---|---|---|---|
| Decision-type→adoption/use | 2.295 | H1 | Validated |
| Communic-chan→adoption/use | 1.963 | H2 | Validated |
| social-system→adoption/use | 2.011 | H3 | Validated |
| Promot-of-change→adoption/use | 0.003 | H4 | Not validated |
| Particip-proc→adoption/use | 2.808 | H5 | Validated |
| Prep-of-change→adoption/use | 0.174 | H6 | Not validated |
| Adoption/use→result-of-use | 4.208 | H7 | Validated |
The construct variables Promot-of-Change (v2, v11 and v14) concerning the participation of the promoter of change, or team leader, who should act in the implementation of a technological innovation, in this case, the EHR. The construct variables Prep-of-Change (v1, v5 and v13) concern the preparation of the environment for the introduction of change. The results show evidence that, in the case of HO-RS, the necessary care has not been observed in the introduction of changes triggered by the implementation of EHR in the institution.
The studies of Rogers (2003) and Perez and Zwicker (2010) indicate that different professionals involved with the use of IS must be prepared for this new system. Similarly, the deployment process of innovation must be led until acceptance by users, at risk of rejection. Because of the sample size, it has not been possible to evaluate the difference in perception of the various types of users. However, in general, the sample studied could assess the perception of the different participants, since each area (medical, nursing, administrative, etc.) uses the system to aid its activities, which are typical.
In the case of the adoption of the EHR, the variables (Communic-Chan, Decision-Type, Particip-Proc, Social-System) validated the model and significantly affected adoption/use, with emphasis on Decision-Type. According to the theory, the way to decide on innovation is defined by the performance of one or more actors with the power of decision and, by a process more flexible or more rigid (Perez, 2006; Rogers, 2003). The way to communicate innovation and a participatory process also encourages adoption. In Table 12 is the validation of the hypothesis.
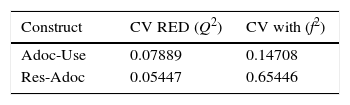
Finally, the evaluation of quality indicators of adjustment model: relevance or predictive validity (Stone-Hari-indicator Q2) and effect size (Cohen-indicator f2). Q2 evaluates the quality of prediction model and f2 indicates how each construct is useful for adjusting the model. The values of the quality indicators calculated with blindfolding of SmartPLS® are indicated in Table 13.
The literature indicates that Q2 must present values greater than zero and, for f2, values of 0.02, 0.15 and 0.35 are considered small, medium and large, respectively (Hair, Hult, Ringle, & Sarstedt, 2014). From Table 13, it should be noted that the values obtained for the quality indicators of adjustment model are consistent with the theory.
ConclusionThis research was developed in order to identify key internal factors that favor the adoption of technological innovation set by the EHR in the area of health. To achieve this, a structural model (Fig. 1) was created, which was submitted to the analysis technique of structural equations, systems with the SmartPLS® statistical software. The results of the survey indicated that most of the internal variables satisfactorily explained the quantitative model proposed by the research, using structural equation modeling. This can be considered a theoretical breakthrough, since the study included few variables studied in adopting innovations (Rogers, 2003).
In the study, the variables highlighted are represented by the promoter of change and preparation for change features which, in the case of the institution studied, had no proper contribution to the adoption, which is at odds with previous studies of Gabris et al. (2001) and Perez (2006). This result points to evidence of flaws in the involvement of leaders and also in preparation for the change in the organization. Studies in other areas can confirm the importance of these two factors.
It was noted that internal organizational environment variables contributed to 32.1% of EHR adoption; this result was provided by Rogers (2003) and the study of Perez (2006). It is important to remember that, according to these authors, the variables related to perceived features on technological innovation of 50% to explain an 80% variance in the adoption rate. In this way, despite the lowest percentage, internal organizational environment variables also help to improve the explanation of the adoption rate of an innovation. A theoretical contribution would be the proposal of studies aimed at assessing the organizational internal variables in conjunction with the variables perceived in the use of an innovation.
The involvement of users with individuals or teams that have developed or introduced the EHR improves the acceptance of the new system, as well as identifying new opportunities to correct and expand functions in that system. Another indicator of user behavior is reflected in the identification of obstacles imposed by the adoption of innovations. Participation in development and the environment preparation showed as being determinants of adoption.
With respect to the goal of identifying the results achieved by the adoption of the EHR, we could see multiple results arising from the adoption of this system in HO-RS, and also the gains made by its introduction. The respondents demonstrated that the institution was able to offer a better service to its patients improve existing processes and services; create new processes and services, in administrative, intra and inter-organizational terms (v19–v26). The results also indicated that other innovations were introduced from the innovation studied (v27), which aimed to keep pace with the rapid development of healthcare (Shortliffe & Blois, 2014).
Another important aspect of the research was the realization that equally or more important than the application of structural equation analysis technique, was a judicious data collection instrument. It was possible to develop and validate a quantitative questionnaire based on Gabris et al. (2001), Rogers (2003) and Perez (2006), which enabled the collection of necessary information. The questionnaire was reviewed by a group of five experts and subsequently underwent a pre-test, before being sent to potential respondents. However, the questionnaire can still be refined and applied to other types of organizations, to test other innovations.
The survey results concern the institution studied, the HO-RS and innovation of EHR, therefore, they cannot be generalized and extended to other institutions. However, such results can serve as guidelines for other healthcare institutions, which are planning to deploy the EHR or other IS.
It is considered that this research was conducted satisfactorily, because the research problem was answered positively, i.e., it was possible to identify the internal factors in a healthcare organization that promote the adoption of IS. In addition, it was possible to develop a structural model to evaluate the contribution generated by the adoption of IS/ICT for improving processes, products and services in the area of health. Finally, it is recommended that the survey be continued, through new studies contemplating other innovations in the area of health, the evaluation of innovations in institutions in other sectors, as well as other technological innovations.
Conflicts of interestThe authors declare no conflicts of interest.
Peer Review under the responsibility of Departamento de Administração, Faculdade de Economia, Administração e Contabilidade da Universidade de São Paulo – FEA/USP.