




Objetivos. Investigar los efectos del entrenamiento continuo versus el entrenamiento intermitente corriendo en piscina profunda para el control y la prevención de la acumulación excesiva de adipocitos sin restricción alimenticia, así como para una mejora del condicionamiento físico y de la calidad de vida.
Métodos. Estudio experimental con treinta mujeres entre 34 y 58 años de edad, con una duración de doce semanas, con tres sesiones semanales de 47 minutos de duración. Se verificó el porcentaje de grasa corporal, la condición cardiorrespiratoria y la calidad de vida mediante la evaluación de criterios del WHOQOLAbreviado. Se aplicaron la prueba estadística t de Student y la no paramétrica de Wilcoxon. Fue establecido un 5% como nivel de significación.
Resultados. Con la única excepción del dominio social de la calidad de vida, todas las variables investigadas reflejaron una mejora en ambos grupos, con predominio del grupo de entrenamiento intermitente sobre el de entrenamiento continuo.
Conclusión. Independientemente de la forma de entrenamiento utilizada, correr en piscina profunda contribuye a la reducción de la grasa corporal, la evolución de la aptitud física y la mejora de los índices contemplados en el WHOQOL-Abreviado.
Objectives. To search intermittent and continous trainning (IT and CT, respectively) effects through deep water running for the control and prevention of excessive body fat accumulation and improvement of quality of life.
Methods. Experimental study composed by 30 women, aged between 34 to 58 years old, during 12 weeks, three sessions per week, 47 minutes each. Body composition, cardiorespiratory condition and Quality of Life by WHOQOL-Brief were considered. Student´s and Wilcoxon´s non parametric tests were applied at 5% significance level.
Results. With the only exception for social domain of quality of life, all investigated variables revealed improvement in both groups for IT in comparison to CT.
Conclusion. Deep water running contributes to body fat reduction, physical fitness evolution and improvement of WHOQOL-Brief domains, regardless of the trainning type conducted.
Introduction
Nowadays, obesity is considered a major public health problem worldwide, as it is increasing at a very fast pace and is associated to diabetes mellitus type II, hypertension, endometrial and colorectal cancer, cardiovascular diseases, sleep apnea, degenerative articular processes and implications on quality of life (QL)1. Studies show an inverse relationship between the sedentarism rate and QL; the higher the weight, the lower the QL2. Systematic physical activities (SPA) cause significant changes in the cardiorespiratory, immunologic, endocrinologic systems, allowing the reduction of body fat, gain of muscle and bone mass, besides preventing chronic degenerative diseases3. Other contributions to QL should also be considered such as reduction of anxiety, improvement of sleep and self-esteem4.
Technically, there are two training types for SPA: the continuous (CT) which involves rhythmical exercises with 60-80% of VO2max intensity for extended time5 and the one with intervals (IT), which refers to repetition of exercise turns alternated with recovery periods6. The first is widely applied as a resource to improve health and to reduce body fat; the second is used for high sports performance. However, IT can be also recommended for those in search of health improvement and reduction of adypocites concentration. IT results in Vo2max. gains and reduction of fat percentage in a more significant way than CT, besides allowing weight maintenance and reduction of cholesterol levels6,7.
The practice of exercises in water environments may be interesting for obese people, as they increase energy consumption when compared to running training on land, besides reducing injury risks8. Among the SPAs performed in water, there is the deep water running (DWR). The practitioner uses a floater attached to the waist allowing the running movements without contacting the pool floor. It is an easy-to-learn activity as the practitioner does not need to know how to swim and there is no impact9-11.
Considering the SPA benefits for health and QL, the purpose of this study was to investigate the CT and IT effects through SPA for the control and prevention of excessive body fat accumulation and improvement of QL in 30 obese women, aged between 34 and 58 years for 12 weeks, with three 47-minute sessions per week.
Methods
Subjects
Initially, 35 women participated; 30 of them (85.71%) concluded the study in two groups (one with IT comprised 18 volunteers and the other with CT composed of 12) and five were excluded due to excess of absences. Mean age of 46.1±07.87 years (45.33±06.33 years for CT and 46.61±07.88 years for IT). Four (13.3%) were submitted to Menopausal Hormone Therapy, one (3.33%) had diabetes mellitus type II and two (6.66%), mild hypertension. No incidents were registered throughout the intervention.
The selected women met the following criteria: be obese (28 to 35% of body fat), aged between 34-58 years old, having not practiced SPA over the last three months, and have medical authorization or recommendation for physical exercise practice. Training participation was not allowed for women who showed: consumptive, hepatic or endocrine disorders, unbalanced renal function or severe dysfunction, chronic obstructive pulmonary disease; pregnancy, neurological or psychiatric problems, abnormal or atypical cardiac response during SPA, use of beta-blockers or anti-obesity drugs, severe hypertension and decompensated diabetes mellitus.
Procedures
The study, characterized as being experimental with two groups, had initial and final assessments and was approved by the Research Ethics Committee of the School of Medicine Science from the University of Campinas (UNICAMP), under the number 640/2005. As dependent variables, physical fitness, reduction of body fat and improvement of QL were considered; the systematic and guided DWR practice was considered as independent variable.
The volunteers' perception of QL was evaluated by using the WHOQOL-Brief (Portuguese version) from the World Health Organization. This tool has 26 standard and closed questions with five response levels, whose answers should be the most appropriate response for the assessments regarding physical, psychological, social relations and environment domains12. These are considered as a set of subjective perceptions from the participation in the production, circulation and goods consumption processes13.
After the WHOQOL-Brief had been filled out, the assessment of the body composition (BC) was started on an individual and systematized basis, which met the following sequence:
a) Body mass (kg), the volunteers being weighted in the standing position, barefoot and wearing a bathing suit; and the balance was calibrated before each weighing.
b) Skinfold (mm), measured in three consecutive times (tricipital, supra-iliac and mid-thigh) all on the right side14.
Data obtained in item ii) were used to find body density, a necessary variable to determine body fat percentage (BFP) by using Siri equation14:
Body Density = 1.099421 - 0.0009929 (X1) + 0.0000023 (X1)2 - 0.0001392 (X2) %GC = [495/ Body Density] - 450
where X1 is the average sum of the tricipital, suprailiac and mid-thigh skinfolds, and X2, is the individual's age in years.
After these assessments, a period for adaptation to get used to the float and to learn DWR training took place. The training occurs in pool with two meter deph and water in shoulder level. In such conditions the center of gravity is changed when compared to same exercise on land, and is transferred from S1 or S2 sacral vertebra to the thorax (pleural cavity), which renders a more difficult body equilibrium during DWR15.
For this reason, postural and motor re-learning is necessary16.
This step lasted three sessions, and the last session was dedicated to a specific cardiorespiratory test for DWR17: whose objective was to estimate the duration time, test heart rate (HRpeak) and movements rhythm achieved by the volunteer during the stationary running. It comprises a 4-minute warming with 48 rhythmic elevations of the right leg per minute followed by eleven 2-minute periods without interval. The first starts with 66 elevations per minute which are added by three or four for the others.
The physical conditioning program started after examining the results obtained from the effort test; the prescription for DWR being based on the method proposed by Karvonen18, which determines the heart rate reserve (HRR).
In each team, the volunteers were allocated to one of the two groups, CT and IT, randomized by simple draw, repeated at each new insertion. This step lasted 12 weeks for both training, totaling 36 sessions.
The sequence for CT group was:
a) First week: assessments, adaptation to a liquid environment and DWR learning.
b) Second and third week: training performed between 65 and 70% HRR.
c) Fourth to sixth week: intensity from 70 to 75 % HRR.
d) Seventh to ninth week: 75 to 80% HRR.
e) Tenth to twelfth week: 80 to 85% of HRR.
For IT, the activities for the first week were the same as for the CT group. Once this phase ended, a sequence with DWR was started at 70-75% HRR associated with the intensive interval training, i.e, high intense stimulus, "sprints", which lasted fifteen seconds with 30 for active recovery, or in terms of weeks (fig. 1):
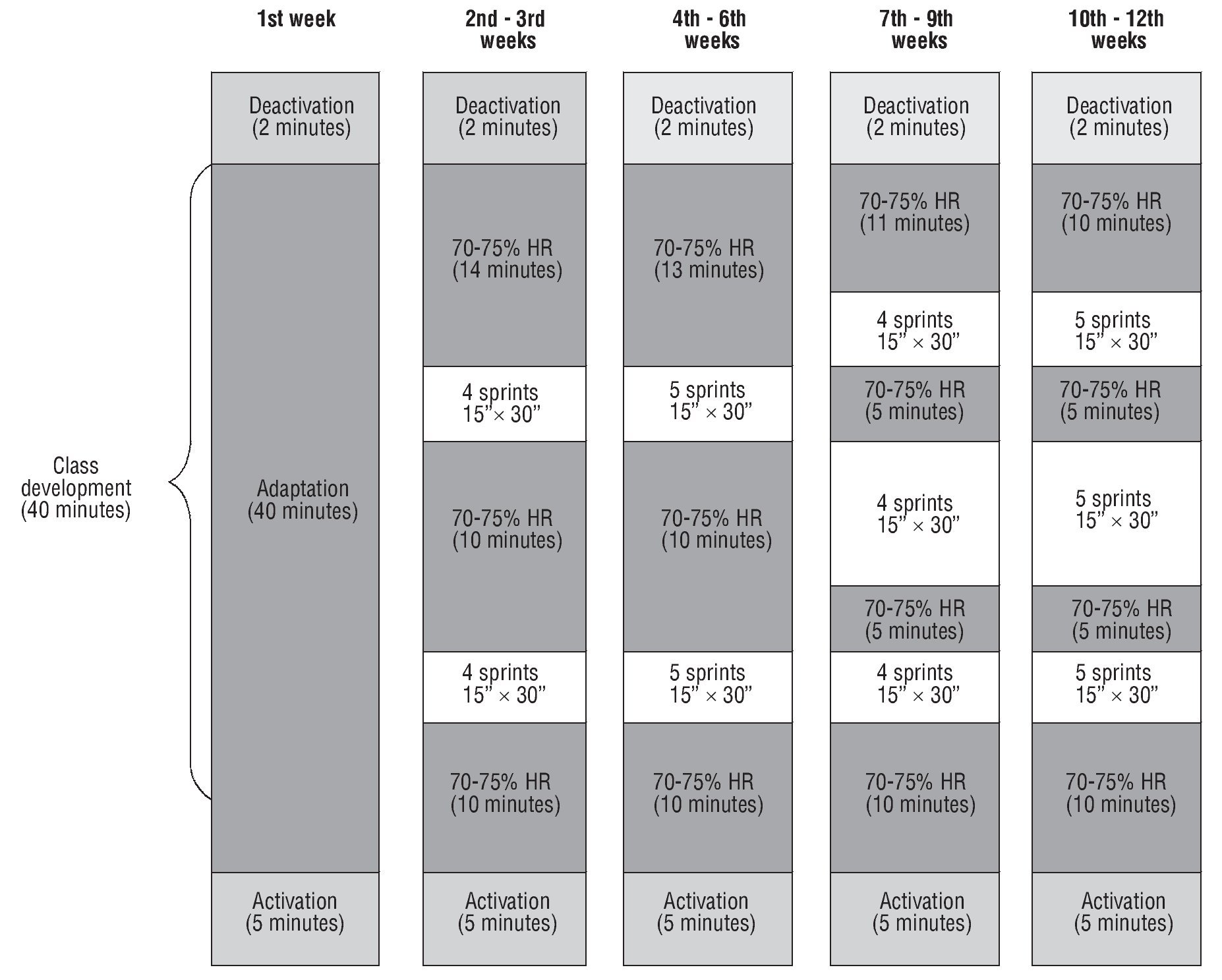
Fig. 1. Periodization scheme of the interval training group.
a) Second to third: eight sprints, allocated in two moments.
b) Fourth to sixth: ten sprints, distributed in three sequences.
c) Seventh to ninth: twelve at top intensity repetitions, available in three series.
d) Tenth to twelfth: fifteen repetitions in three series.
The interval exercises, always considering motion, were distributed into two or three stimuli sets specifically numbered. After checking the initial heart rate (HRIn), the evaluated women practiced the exercises in the proposed intensity, i. e. 70-75% HRR for 10 minutes and immediately after they started the first of maximum effort activities, and later returned to the defined target effort.
Two sets of sprints were carried out between the second and sixth training weeks. For other sessions, high intensity stimuli were allocated in three stages, with a five-minute interval between them.
The participants included in the CT and IT groups were monitored during all classes, regarding the heart rate at three-minute intervals, from the end of warm-up up to two minutes after stopping the activity, in to order to follow the effort HR individually established for each session. At the end of the 12-week program, new assessments were made in order to compare the data obtained between the beginning and the end of this study.
Absences were allowed, provided they would not be higher than 20% of total sessions (seven absences); if higher, the volunteer was automatically excluded from the study. For other cases, the classes were replaced following the same schedules of the regular period, and the participant should train observing the session target she missed.
Statistical analysis
As per the analytical assessment, Student's t test and Wilcoxon's non-parametric test were applied19. Data normality was assessed through the Kolmogorov Smirnov test19. Statistical significance was set at p < 0.05 and values were given as mean ± standard deviation20.
Results
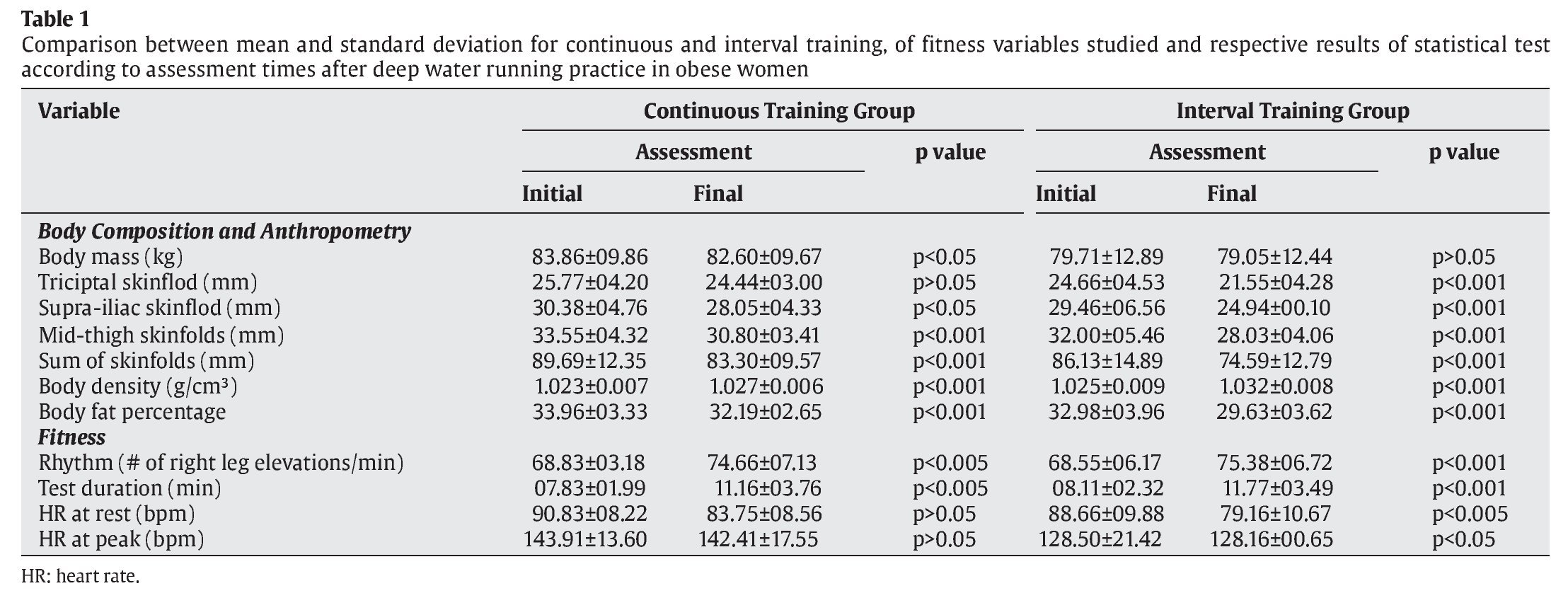
Table 1 shows results for BC and physical fitness, considering the initial and final times, according to the training type. The reduction of body mass, in spite of having occurred in CT and IT, was significant for only CT (p<0.05), while the sum of skinfolds (p≤0.05) expressed this behavior in both groups.
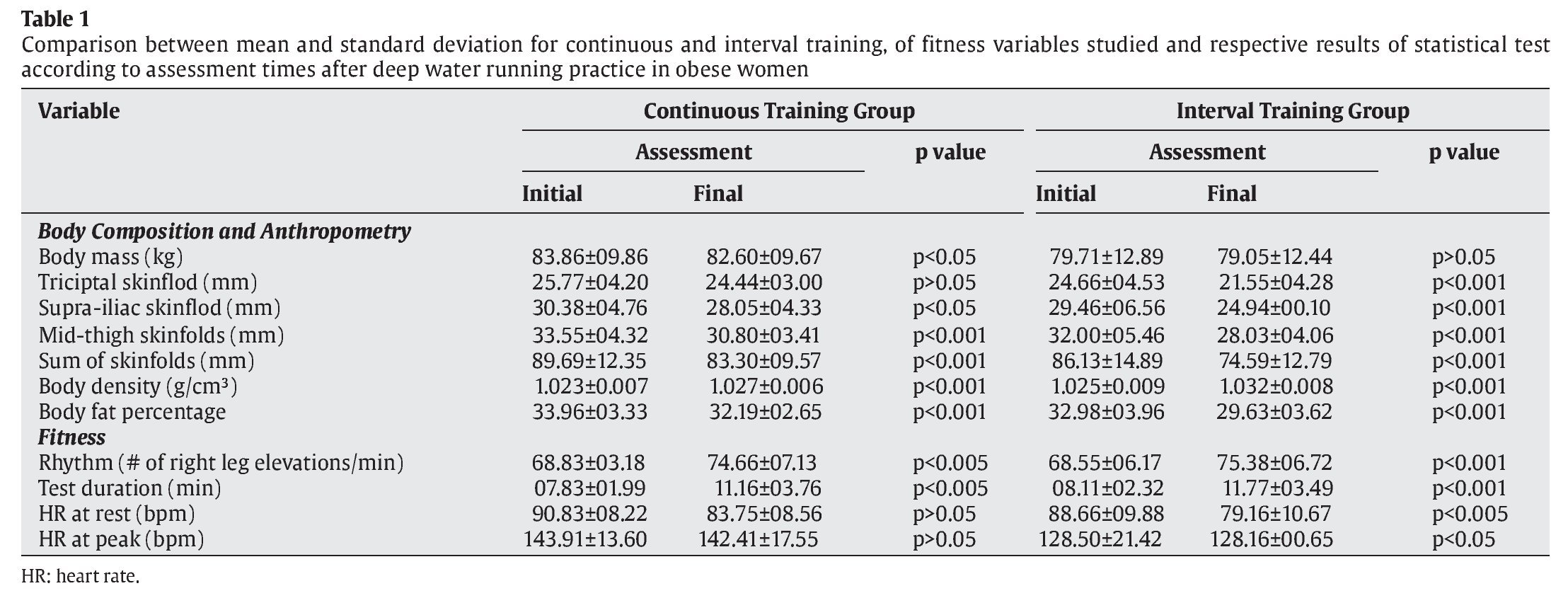
Body density of p<0.001 indicates improvement in IC and CT; as for the benefits of the continuous and intermittent effort for changes in body composition, it is noticeable that IT has produced twice as much fat reduction as CT (p<0.01).
The increase in rhythm (p≤0.005) indicates the cardiorespiratory fitness level improved in both groups, being more significant in the IT (p<0.001).
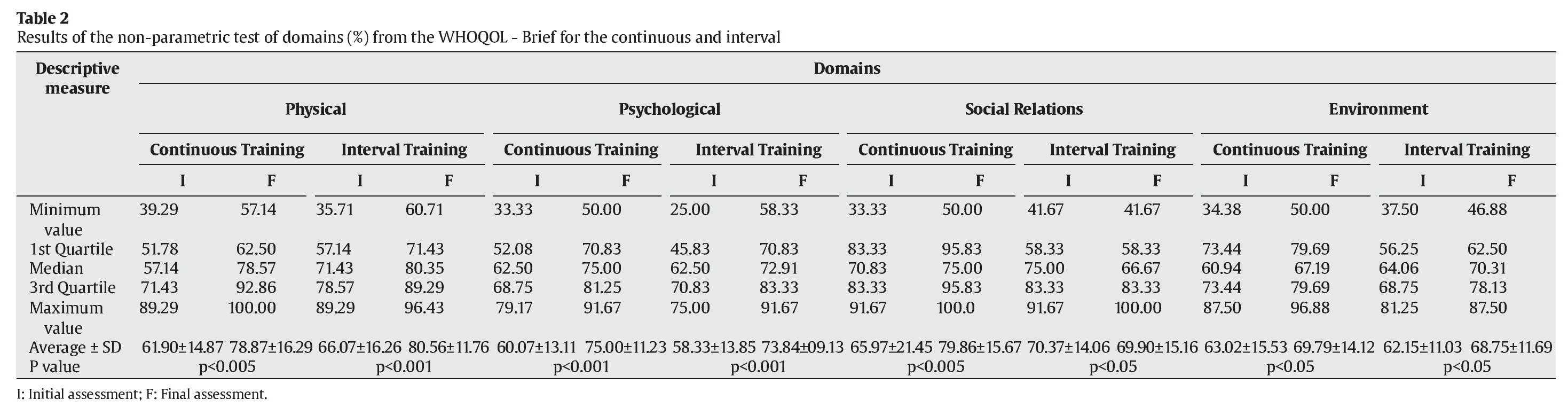
The results in table 2 show the contributions of both training types for improvement of QL DWR contributed similarly for the evolution of women's subjective perception regardless of the proposed interval characteristic.
Discussion
When evaluating the obtained data, one peculiar situation calls the attention related to the compliance with the proposed program, as five volunteers were excluded due to the excessive number of absences and all belonged to the CT group. According to the participants, the high intensity stimuli were more interesting and motivating than those of the CT, regarded as more monotonous, and this could be the reason for the training interruption.
Considering this, it is well known that exercise practice aiming at weight loss contributes to the favorable evolution of emotional aspects such as humor, self-esteem and body image21. In fact, behavior changes towards physical activities and personal relationships were reported in a six-month study on food control and seven weekly 30 to 40-minute long, especially regarding those submitted to high intensity efforts sessions22.
When considering BC, the deep water running practice allowed the reduction of concentrations of localized and general fat, as Assis23 had already reported in a 15-week study on women with fibromyalgia submitted to stationary DWR.
Body density as well as rhythm were improved, showing respectively increase in body mass24 and cardiorespiratory evolution.
The physical domain in the World Health Organization questionnaire shows improvement and further possibility to be improved with physical activity practice25. The second domain, which involves psychological aspects, includes positive feelings, body image, self-esteem and appearance positively favoring the BC changes26. Probably, people socialization with similar characteristics promoted exchange of experiences and stories with consequent influence on the evolution of social relationships by obese women after DWR27.
Data related to the environment domain call our attention, since they are associated with the essentially economic reality of nature28 as opportunities for recreation and leisure, education, residence, physical environment and satisfaction at work29, on which SPA has little direct interference30. It is believable that such responses are somewhat related with the growing economic trend in Brazil at the time of this intervention. On the other hand, these results were not affected in a similar study conducted by Pasetti; Gonçalves; Padovani11, in a period when the country was beginning to change with a strong social proposal, originating great positive personal expectations.
Studies emphasize that continuous resistance or aerobic exercises are beneficial to QL of different populations as, for instance, those with fibromyalgia23 or cardiopathy31,32 and people with chronicle renal problems33. Data obtained with DWR confirm these findings and indicate that interval training can also contribute to the increase of expressive body fat reduction, besides improving QL of obese women.
In conclusion deep water running has been shown to contribute to body fat reduction, physical fitness evolution and improvement of WHOQOL-Brief domains, regardless of the training type conducted.
Correspondencia:
S.R. Pasetti.
Rua Renato Reis, 56.
Jardim America, Campinas, SP, Brasil
E-mail: srpasetti@hotmail.com
History of the article:
Received August 1, 2011
Accepted December 3, 2011
