


Evaluate isokinetic muscle performance of the hamstring and quadriceps muscles in male handball players, as well as verify the effect of handball match on salivary cortisol and immunoglobulin A by Fourier transform infrared spectroscopy.
MethodThe isokinetic parameters evaluated were peak torque, fatigue index, and hamstring/quadriceps peak torque ratio. Saliva samples were collected before and after a simulated handball match, as well as after 2h of recovery. Analysis of saliva by Fourier transform infrared spectroscopy was based on infrared region of the pure substances (cortisol and human salivary cortisol and immunoglobulin A).
ResultsNo significant difference was found between the non-dominant and dominant lower limb at 60 and 180°/s, in extension and flexion for variables of peak torque and fatigue index. The hamstring/quadriceps ratio at 60°/s was lower than at 180°/s. The main absorption bands of cortisol are in the region (1180–955cm−1) and human salivary cortisol and immunoglobulin A bands in the region (1584–1489cm−1). The saliva samples collected before and after match showed no significant difference. The variation of cortisol per playing positions was positively correlated with session rate of perceived exertion.
ConclusionsThe handball players had good muscle performance of the lower limbs in the isokinetic evaluation. The Fourier transform infrared spectroscopy analysis identified the main absorption bands of cortisol and salivary cortisol and immunoglobulin A, as well as playing positions that demand higher stress levels, through changes of bands related to salivary cortisol.
Evaluar el rendimiento muscular isocinético de los isquiotibiales y los cuádriceps en jugadores de balonmano masculino, así como examinar el efecto de un partido de balonmano en el cortisol salival y la inmunoglobulina A por espectroscopia infrarroja con transformada de Fourier.
MétodoLos parámetros isocinéticos evaluados fueron el torque máximo, el índice de fatiga y la razón de torque máximo isquiotibial/cuádriceps. Las muestras de saliva se recogieron antes y después de un partido de balonmano simulado y tras 2h de recuperación. El análisis de la saliva por espectroscopia infrarroja con transformada de Fourier se basó en las regiones de infrarrojos de sustancias puras (cortisol, cortisol salival y la inmunoglobulina A humana).
ResultadosNo hubo diferencias significativas entre los miembros inferiores dominante y no dominante a 60 y 180°/s, en extensión y flexión para torque máximo e índice de fatiga. La razón isquiotibial/cuádriceps a 60°/s fue inferior que a 180°/s. Las principales bandas de absorción de cortisol se encuentran en la región (1180–955cm−1) y cortisol salival e inmunoglobulina A en la región (1584–1489cm−1). Las muestras de saliva recogidas antes y después del partido no muestran diferencias significativas. La variación de cortisol por la posición de juego se correlacionó positivamente con la tasa de esfuerzo percibido en la sesión.
ConclusionesLos jugadores de balonmano mostraron buen rendimiento muscular de los miembros inferiores en la evaluación isocinética. El análisis por espectroscopia infrarroja con transformada de Fourier identificó las principales bandas de cortisol y cortisol salival e inmunoglobulina A, así como las posiciones de juego que requieren mayores niveles de estrés, por medio de los cambios en las bandas relacionadas con el cortisol salival.
Avaliar o desempenho muscular isocinético dos flexores e extensores do joelho em jogadores de handebol do sexo masculino, bem como verificar o efeito da partida de handebol sobre o cortisol salivar e imunoglobulina A por espectroscopia no infravermelho.
MétodoOs seguintes parâmetros foram avaliados com dinamômetro isocinético: o torque máximo, índice de fadiga e razão agonista/antagonista. Amostras de saliva foram coletadas antes e depois de uma partida de handebol simulada, bem como depois de 2 horas de recuperação. Análise de saliva por espectroscopia no infravermelho foi baseada na região do infravermelho das substâncias puras (cortisol e imunoglobulina A humano).
ResultadosNão foi encontrada diferença significativa entre dos membros inferiores não-dominante e dominante em 60 e 180°/s, em extensão e flexão para variáveis do torque máximo e índice de fadiga. A relação flexores/extensores do joelho a 60°/s foi inferior a 180°/s. As principais bandas de absorção do cortisol estão na região (1180–955 cm-1) e bandas de imunoglobulina A humana na região (1584–1489cm-1). As amostras de saliva coletadas antes e depois do jogo não apresentaram diferenças significativas. A variação do cortisol por posições de jogo foi positivamente correlacionada com a taxa de percepção subjetiva de esforço da sessão.
ConclusõesOs jogadores de handebol tiveram bom desempenho muscular dos membros inferiores na avaliação isocinética. A análise espectroscopia no infravermelho identificou as principais bandas de absorção de cortisol e imunoglobulina A, bem como as posições de jogo que exigem níveis mais elevados de estresse, através de mudanças de bandas relacionadas com cortisol salivar.
Research on professional sports has examined parameters to establish muscle function,1,2 as well as the association between physical fitness level and overtraining biomarkers, such as cortisol, salivary cortisol and immunoglobulin A (SIgA), and α-amylase, among others.3,4 In collective sports, evaluation of the knee joint is very important due to the demand imposed on it during training and competition. Isokinetic testing enables precise assessment of athletes’ muscle strength; therefore, this method allows evaluation of quadriceps and hamstring muscle strength, to determine the magnitude of generated torque, as well as the hamstring to quadriceps (H/Q) strength ratio. This evaluation is also widely used in injury prevention programmers.1,5,6
In addition, the evaluation of athletes’ skeletal muscle, psychological and physiological stress levels, from training and sports competitions, has also been extensively studied by salivary biomarkers, which reflect the impact of stress and physical exercise on the most important body regulatory systems.3,4,7 Cortisol and SIgA are widely studied to investigate the response of the endocrine and immune systems, which are commonly analyzed by chromatographic and mass spectrometry techniques, as well as colorimetric and immunoassay methods.3,9–11 However, these laboratory tests are relatively expensive and laborious to be routinely applied in teams without financial support.
In this context, new analysis tools have been studied in order to reduce expenditure. Fourier transform infrared spectroscopy (FT-IR) technique has great potential for analysis of body fluids,12,13 to quantify the biochemical components of a biological sample. This quantification is done by the absorption bands of the vibrational modes of molecular radicals in the infrared spectral region of 4000–700cm−1.14 The main advantages of FT-IR are the small quantity of sample required and the real-time information provided without the use of reagents.15–17 Several studies have shown the effect of acute stress and the impact of sustained periods of stress on salivary cortisol concentrations and SIgA in athletes.3 To the best of our knowledge, there are no records in the literature about the effects of a handball match on immune-endocrine system using FT-IR for diagnosis. Monitoring these responses could help coaches to plan appropriate training loads and recovery time, to reduce health risks and increase athletic performance. Thus, the purpose of this study was to evaluated isokinetic parameters of the hamstring and quadriceps muscles of male handball players, as well as changes in salivary cortisol and SIgA by FT-IR, during a simulated handball match.
MethodThis study was approved by the Research Ethics Committee of the Universidade do Vale do Paraiba (No. 255.474) and is in accordance with the ethical standards of the Helsinki Declaration and Brazilian resolution 466/12. All subjects provided written informed consent before participation.
SubjectsThe sample comprised 14 male handball players (Age: 22.41±2.27 years; height: 1.84±0.06cm; body mass: 87.28±10.11kg), who had experience with this sport for approximately five years. All players were trained twice a day (90–120min per session), five days per week (depending on the number of matches per week). The training sessions consisted of specific conditioning work, weight training, handball drills, sprints, tactics, and intermittent running exercises.
The exclusion criteria were use of drugs/tobacco, existence of oral disease and any type of physical injury. Thus, the saliva samples of one athlete and isokinetic evaluation of two athletes were properly excluded, because one player had an oral injury during the match, and two players were injured one day before the isokinetic test.
Experimental designThe experiment was divided in two phases. In the first stage, the participants’ isokinetic concentric strength of the dominant and non-dominant lower limb was assessed on the isokinetic dynamometer (Biodex Medical Systems Inc., NY, USA). After they performed a 5min warm-up on a treadmill (Movement LX 150), the athletes were positioned seated on the isokinetic dynamometer with their hips flexed at approximately 85°, and trunk and thigh stabilized, to avoid compensatory movements. The dynamometer axis was visually aligned with lateral femoral condyle, while the knees were flexed at 90°. The length of the lever arm was individually determined using the length of each athlete's lower leg. The knee was tested on a range of motion from 0° to 90° of knee flexion, with full knee extension considered 0°. As part of the familiarization process, the athletes performed three repetitions in the equipment before starting the test.2,18
The test protocol was based on concentric isokinetic repetition of flexion and extension with 60s recovery between sets, which were at angular velocity of 60°/s (five repetitions) and 180°/s (30 repetitions). The evaluated isokinetic parameters were peak torque (PT) of the hamstring (H) and quadriceps (Q) muscles normalized by body mass, fatigue index (FI), and H/Q peak torque ratio (H/Q ratio).1,2,18
The second phase started after 48h, where the biochemical changes of saliva were verified in response to a simulated handball match. First, the athletes performed a 20min warm-up, which included stretching, running, and sport-specific exercises. The match was composed of two halves of 30min with 5min interval for recovering and hydration ad libitum. In addition, all official rules were maintained and no player was substituted during the match.
The match intensity was assessed by exercise duration (minutes) multiplied by training load, using the Borg CR-10 scale,19 recorded 30min after match. The players answered a simple question: “How was your workout?”, and for this, a chart was shown that outlined the full RPE scale with the appropriate explanations.
All subjects were informed by an information document in advance to abstain from food and caffeine products for at least 2h prior to the saliva collection. The athletes were required to rinse out their mouths with distilled water, then remained seated with eyes open, head tilted slightly forward, and avoiding orofacial movements.3,8 The collection was performed approximately 10min before the pre-match warm-up (∼16:00h) and post-match at 5 and 120min.
Unstimulated saliva was collected into a 2ml sterile tube for approximately 10min per athlete. The samples were immediately cooled down at 18°C and centrifuged at 6500rpm for 30min. The supernatant was stored at −20°C.
Defrosted samples were centrifuged again for 5min at 6500rpm. After this process, 15μl of salivary supernatant was deposited on a calcium fluoride (CaF2) window and dehydrated for 30min (Eppendorf Concentrator 5301).
Identification of the infrared bands of cortisol and SIgA was done by the acquisition of the spectra of pure substances, purchased from Sigma–Aldrich® and In vivogen companies, respectively. For this, 15μl of cortisol in methanol (0.015mg/μl) and 15μl of human SIgA in saline (0.015mg/μl) were deposited on CaF2 window and lyophilized.
Infrared spectra were collected by a Spectrum 400 spectrophotometer coupled to a microscope (Perkin–Elmer, Spotlight 400, USA), controlled by a computer using Spotlight 400 Software. Spectra were recorded in the spectral region 4000 to 750cm1, with 32 scans and a resolution of 4cm−1. The measurements were performed along the thin film in eight random points, formed on the CaF2 surface.20 The total spectra collected were 312 for saliva samples.
Statistical analysesThe means and standard deviation of the data were calculated. The distribution of the areas calculated was assumed to be Gaussian, and this assumption/hypothesis was verified using the Kolmogorov–Smirnov test for normal distributions. The one-way ANOVA test was used to compare the group means (Spectra of the saliva sample collected pre-match, post-match and two hours post-match).21,22 The significance level was set at 0.05. Pearson's coefficient was used for data correlation.
The FT-IR spectra of saliva sample and pure substances (cortisol and human SIgA) were standardized, baseline correction, and normalization (0–1). Then, the areas were calculated by integration of spectral region as follows: region 1 (1180–955cm−1), region 2 (1484–1191cm−1), and region 3 (1584–1489cm−1). For this procedure, the software Excel 2007, Origin V8.5, and OPUS V4.2 was used.
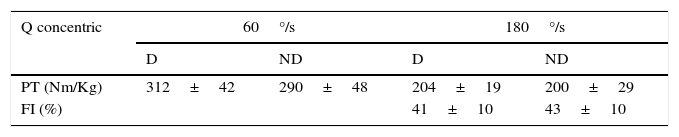
ResultsIsokinetic muscle performanceThe results from isokinetic tests are in Table 1. The statistics analysis showed no significant difference between the non-dominant (ND) and dominant (D) lower limb from 60°/s and 180°/s, in both extension and flexion, for variables of PT and FI. As expected, the H/Q ratio at 60°/s was lower than at 180°/s.
Peak Torque values normalized by body mass, Fatiguez Index and Hamstrings Muscles Quadriceps Muscles Peak Torque Ratio ratio to 60 and 180°/s non-dominant and dominant lower limb of athletes (n=12).
| Q concentric | 60°/s | 180°/s | ||
|---|---|---|---|---|
| D | ND | D | ND | |
| PT (Nm/Kg) | 312±42 | 290±48 | 204±19 | 200±29 |
| FI (%) | 41±10 | 43±10 | ||
| H concentric | 60°/s | 180°/s | ||
|---|---|---|---|---|
| D | ND | D | ND | |
| PT (Nm/Kg) | 163±33 | 160±36 | 126±19 | 137±27 |
| FI (%) | 35±8 | 39±10 | ||
| H/Q ratio (%) | 55±13 | 55±14 | 65±14 | 66±12 |
Values are presented as mean±SD;
PT=peak torque normalized by body mass; H=hamstrings muscles; Q=quadriceps muscles; FI=fatigue index; and H/Q ratio=H/Q peak torque ratio.
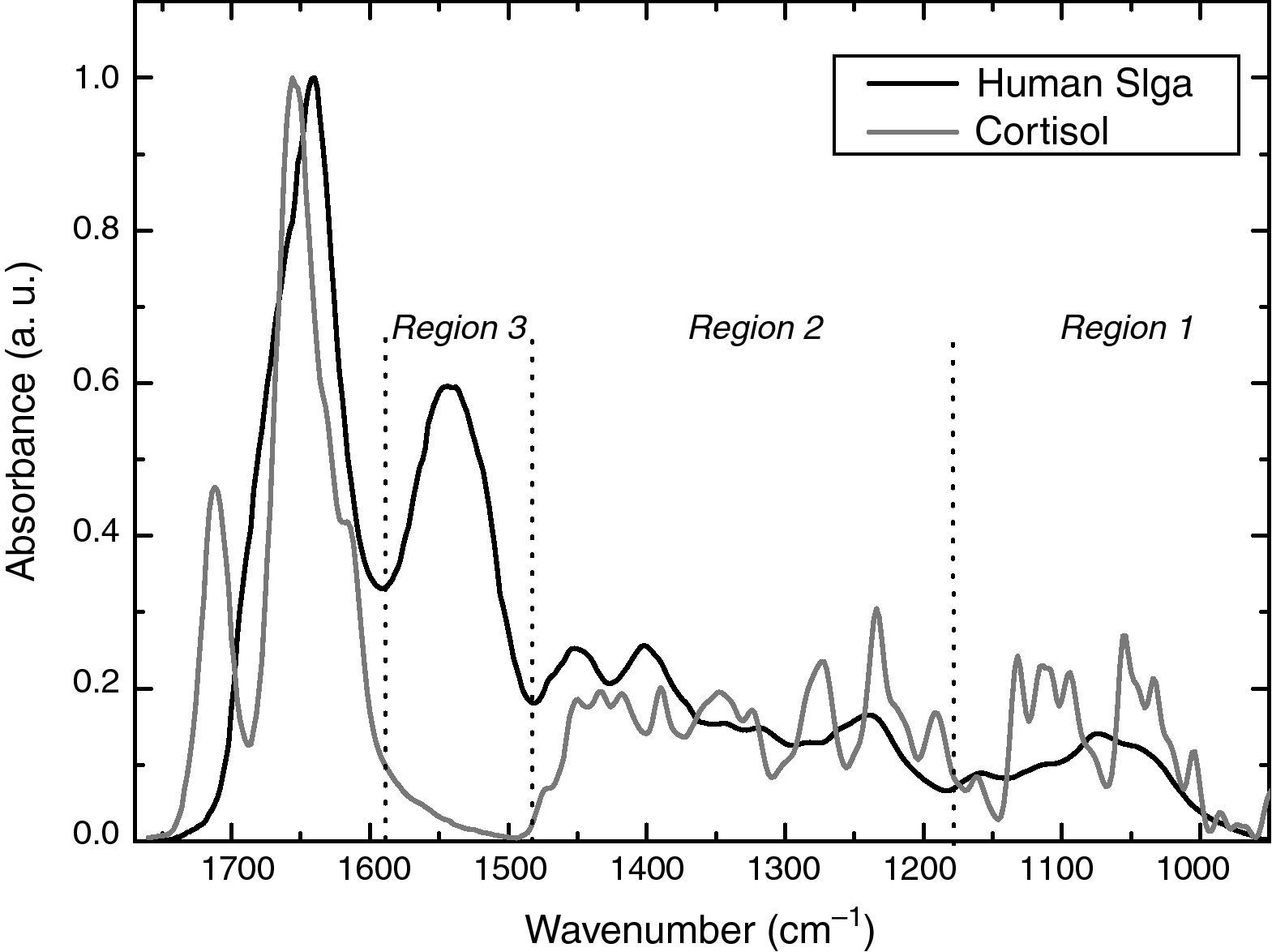
Analysis of pure substances of cortisol and human SIgA by FT-IR.
The average FT-IR spectra of pure substances of cortisol and human SIgA are shown in Fig. 1. The spectra were spread in three regions: (1) 1180–955cm−1, the bands are assignment mostly for cortisol; (2) 1484–1191cm−1, cortisol and human SIgA have similar contribution; and (3) 1584–1489cm−1 has strong contribution of SIgA compared to cortisol.
Training load and salivary immune-endocrine responses in handball players by FT-IR.")
The training load reported by the athletes was 15%, very difficult; 62%, difficult; and 23%, moderate, respectively. Then physical effort of the game was considerably intense.
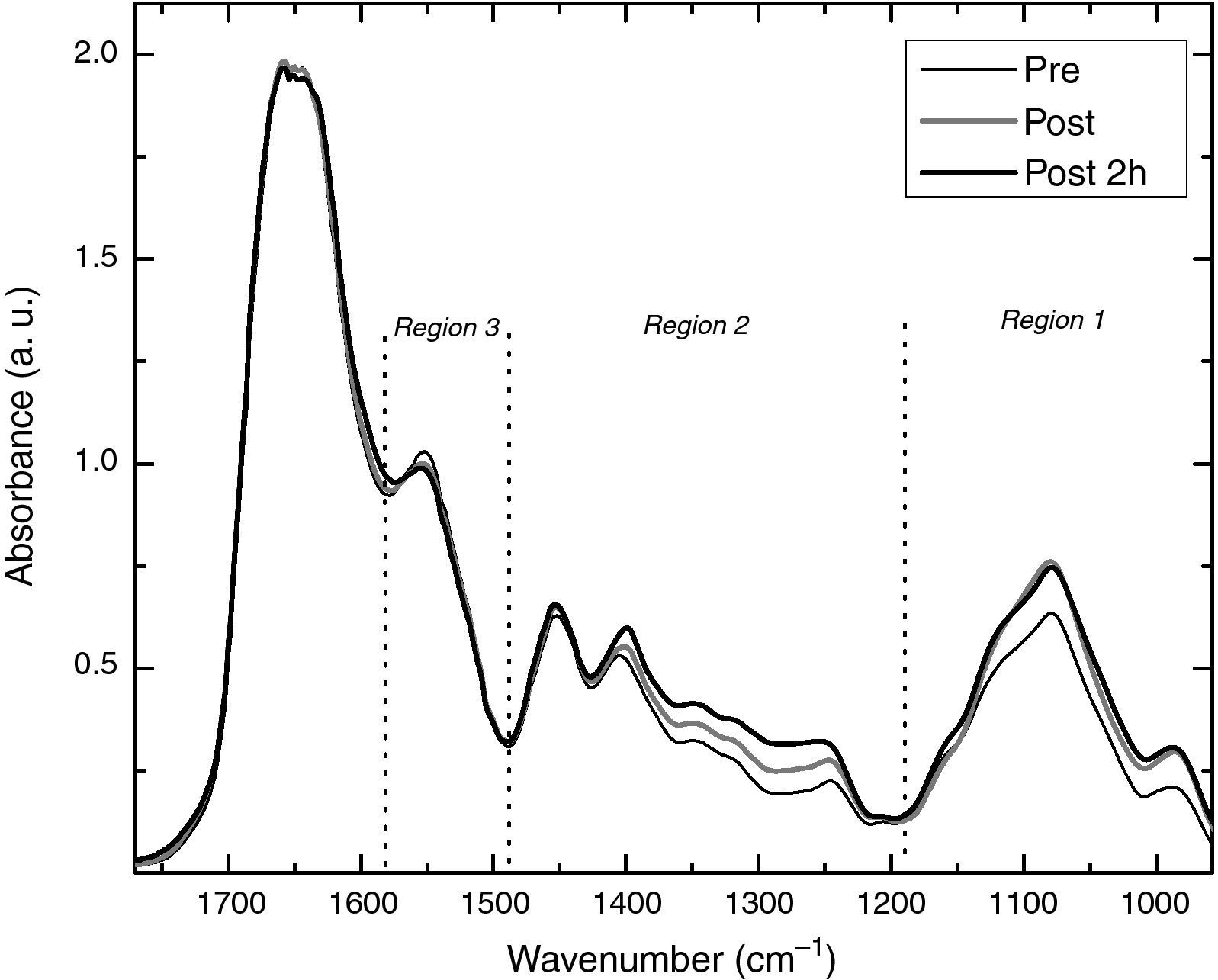
Fig. 2 shows the average FT-IR spectra of the saliva sample collected pre-match (Pre), post-match (Post), and two hours post-match (Post 2h). The results showed difference after exercise that could be attributed by biochemical changes in saliva, especially in region 1.

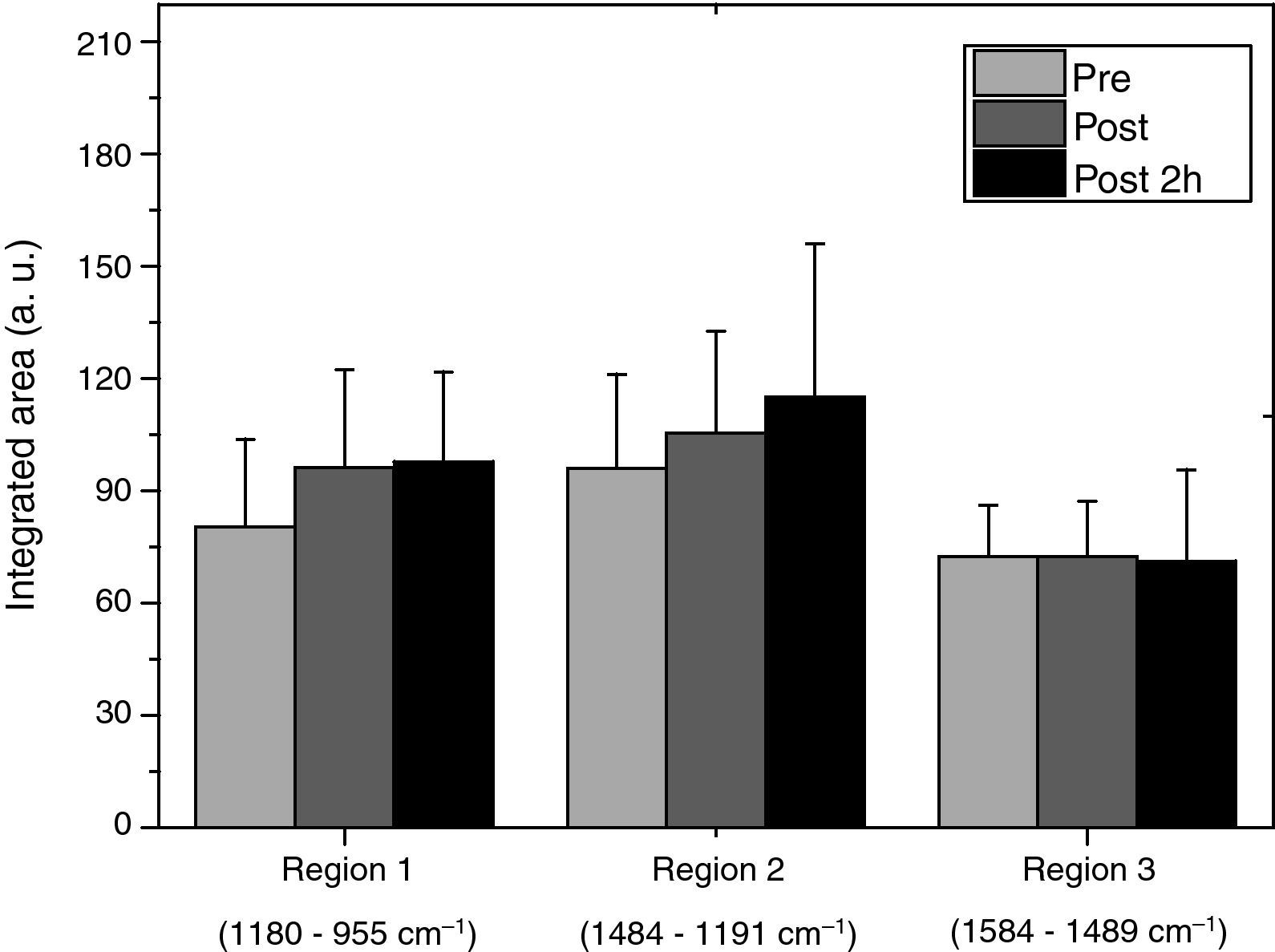
In order to visualize these differences statistically, the integration area was performed in the three regions (Fig. 3). There was no significant difference between the saliva sample collected before, after match, and after two h of recovery, but an increase of bands intensities in regions 1 and 2 was observed as a function of physical effort.
.")
Region 1 had the highest variation of intensity after the match although without statistic relevance. These results could be explained by the player position due to difference in physiological demands during the handball match,23 increasing SD of the area.
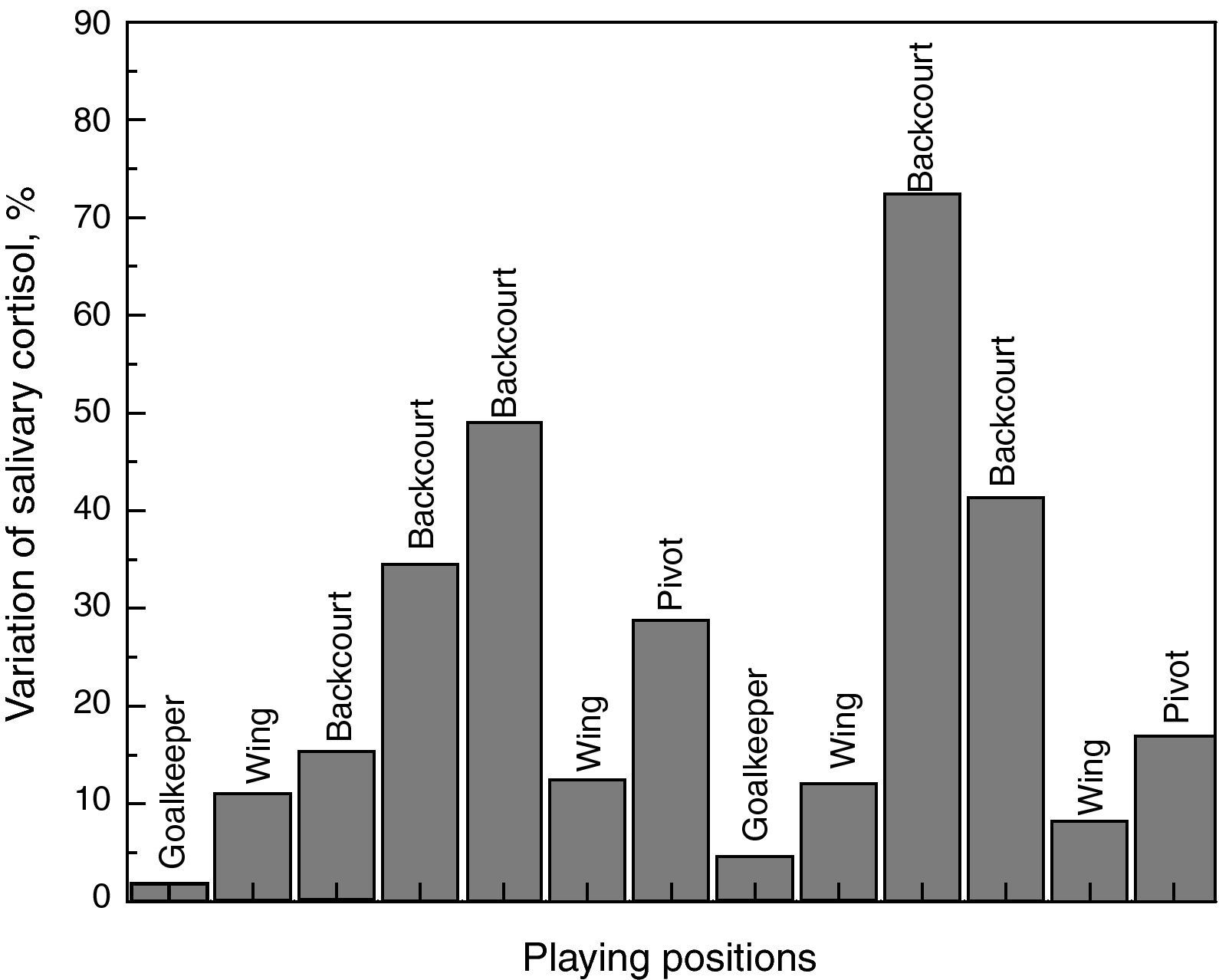
In order to take into account the player position and the results of region 1 assigned to cortisol, Fig. 4 shows the differences between pre and post-match as function of the position, such as backcourt, goalkeeper, pivot, and wings. Wings and backcourts had the highest percentages of variation compared to goalkeepers and pivots (Fig. 4).
Discussion
Scientific knowledge about the influence of the exercise on muscle performance and high intensity training on stress biomarkers is very important to sport medicine. Thus, this study was to show isokinetic parameters in handball players and the effects of a handball match on the immune-endocrine system. Salivary biomarkers were analyzed using a new laboratory diagnostic tool.
Isokinetic muscle performanceThere are few studies reporting isokinetic parameters of handball players’ knees. Thus, the results presented in this studied can serve for future comparisons between athletes from the same sport.
The peak torque comparison between D and ND lower limb of athletes were not statistically relevant. Similar results were found in volleyball and soccer players, where the athletes also did not present a difference between D and ND limb.2 These results can be explained by training specificity, because the athletes are submitted to training programs involving strength, resistance, balance, and flexibility, which could correct some muscular deficit. This training program is important to improve sport performance and prevent injury.24,25
Isokinetic evaluation of the H/Q ratio provides a quantitative measurement of torque from agonist and antagonist muscle contraction surrounding the knee joint. The athletes had values of H/Q ratio at 60°/s and 180°/s for D and ND limb in the range described in the literature.26,27 Although it is not specific for handball athletes, H/Q ratio is typically in the range of 50–80% with an increased values at faster speeds.26,27 According to Andrade et al.,1 H/Q ratio higher than 60% at 180°/s is a good marker because only at high test speed are the similar results to sport tasks.
The FI values for agonist/antagonist musculature of D and ND lower limb were not significantly different. All results were below 50%, which represents the ability of the muscle to maintain at least 50% of job generation, during 30 repetitions.28 This reduces injury risks in periods of training and competition, because there is a similarity between flexor and extensor musculature to resist fatigue.
Analysis of pure substances of cortisol and human SIgA by FT-IRThe infrared spectra of pure substance of cortisol and human SIgA were performed in order to show the main bands in the infrared region. These biomarkers are widely used to investigate different physiological responses in collective sports modalities.3,29 Thus, the immune-endocrine response in handball players was examined by these two salivary biomarkers.
Region 1 (1180–955cm−1), referring to stretching of CO (carbonoxygen bond), CC (carboncarbon bond), angular bending of COH (carbonoxygenhydrogen bond), COC (carbon-oxygen-carbon bond) and symmetric stretching vibrations of the PO (phosphoroxygen double bond) for phosphate group, is largely attributed to the cortisol molecule. This hormone is formed by C21H30O5 containing three six-membered rings and one cyclopentane ring with ketone oxygens at C-3 (carbon-3) and C-20 (carbon-20), the double bond between C-4 (carbon-4) and C-5 (carbon-5), the b-hydroxyl group at C-11 (carbon-11), the two-carbon chain in b-orientation, the hydroxyl group in at C-17 (carbon-17), and b-methyl groups at C-18 (carbon-18) and C-19 (carbon-19).15
Region 2 (1484–1191cm−1), which corresponds to vibrational modes of CH2/CH3, CO (carbonoxygen double bond) of COO− (carboxyl group) symmetric (stretching), amide III (protein), and asymmetric stretching bond (PO) of phosphate group, showed bands of pure substances of cortisol and human SIgA.
Region 3 (1584–1489cm−1), assigned to tyrosine band, amide II and α-helix (amino acids and proteins), showed only one band of SIgA. This protein consists of four heavy chains and two light chains, adopting a characteristic “immunoglobulin fold”, comprised of various amino acid residues of β antiparallel-sheet, around an internal disulfide bridge.30
Training load and salivary immune-endocrine responses in handball players by FT-IRTraining load was used as an indicator of exercise intensity. This method has largely been used as a useful tool for prescribing exercise intensity based on its relationship with physiological indicators of exercise stress. In addition, it does not appear to be affected by exercise modality or training state.31
In this study, the players indicated that the match intensity was difficult or very difficult. The goalkeepers reported the physical effort intensity as moderate, which can be explained by faster recovery intervals of this position.23
The effects of a handball match on immune-endocrine system by infrared analysis of the salivary biomarkers (cortisol and human SIgA) were examined. The results showed differences in band intensities for spectra of saliva sample collected before, after match, and after 2h of recovery, especially in regions 1 and 2. However, the comparison of the mean values of the area of region 1 was not statistically relevant.
This shows that the stress imposed by the match was not enough to significantly increase cortisol levels. Handball is considered a complex and highly demanding intermittent sport, because it involves multiple high-intensity and low-intensity activities, such as turns, stops, jumps, throws, changes of direction, and one-on-one situations in offensive and defensive play.23 Thus, the recovery periods during the handball match and physiological adaptations resulting from physical training avoid high stress levels.32 These finding corroborate with Moreira et al.33 who did not observe any significant differences in salivary cortisol by enzyme-linked immunosorbent assays (ELISA), after a competitive training match in male professional soccer players.
In addition, cortisol is a glucocorticoid produced in the adrenal glands that are controlled by the hypothalamus-pituitary-adrenal axis in response to stress, which could be related to emotional, physiological, and behavioral dimensions.34 In this sense, the psychological factor as an additional stressor in sports also helps to explain the results. Some studies, for example, showed that levels of cortisol after an official match are considerably higher compared to a simulated match.3,35
The individual variation of salivary cortisol showed that backcourt players have higher stress levels than other playing positions. Póvoas et al.23 showed that these player positions require more physically demanding play per game than other positions. This variation of the cortisol values as function of playing positions was correlated with the training load (r=0.73, p<0.05).
For the mucosal parameters, there were no differences in band intensities in the region assigned to SIgA for saliva samples collected before, after match, and after 2h of recovery. These results suggest that the simulated match also did not change SIgA levels in handball players.
As previously discussion, the physical demands (intermittent nature) of a handball match, which includes periods of recovery between efforts and relatively short durations of action,23 could explain these findings in mucosal parameters. In addition, the psychological factor helps to explain this immune response because it was a simulated match.3
Some authors report that the influence of exercise on the immune response depends on exercise intensity and duration.36,37 However, the lack of information about the physiological parameters during the match challenge the statement, for example, heart rate and lactate. In addition, time motion analysis could reveal differences in the number and intensity of actions and distance covered by the players, which could help to explain the results obtained. However, some of these measurements are expensive and difficult to monitor during a handball match.
It is noteworthy that the main limitation of this study is the lack of measurements of cortisol and SIgA concentrations using ELISA. These measurements are important to confirm the infrared results because the bands observed in this infrared region are not exclusively for cortisol and SIgA, because other salivary biomarkers can change in response to stress and could have similar chemical structure, showing similar bands in regions of SIgA and cortisol (e.g., α-amylase and testosterone). Despite these limitations, FT-IR spectroscopy produced promising results with quantitative analysis of stress biomarkers and provided real-time information without the use of any reagents. This decreases the price of the analyses and precise monitoring of players that belong to teams without financial support, to help them avoid excessive training loads during the preparation to decisive matches.
In summary, the results of this study showed that the handball players had good performance of the lower limb muscles with balanced H/Q, no strength difference between D and ND limbs, and appropriate IF percentage. The results of infrared analysis showed the main absorption bands for cortisol in region 1180–955cm−1 and for human SIgA in region 1584–1489cm−1. There were no significant spectral differences to saliva sample collected pre and post-match, as well as after 2h of recovery. In addition, the playing position as function of cortisol absorption band could be positively correlated to the training load, showing the playing position that require higher degrees of stress during a simulated handball match.
Ethical disclosuresProtection of human subjects and animals in researchThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors wish to thanks the financial support given by Coordination for the Improvement of Higher Education Personnel (CAPES) and Vale Paraibana Teaching Foundation (FVE).
