


Objetivo. Investigar la asociación entre el desempeño motor y actividad física habitual (AFH) en individuos en los grados leve y moderado de la enfermedad de Parkinson (EP).
Método. El estudio contó con individuos con EP, entre los grados 0 - 3 de la escala modificada de Hoehn y Yahr. Las pruebas de desempeño motor utilizados fueron: fuerza de la mano, evaluada por el dinamómetro (kg) y la prueba de "sentarse y levantarse" (segundos). El cuestionario Baecke analizó las puntuaciones de AFH en los últimos 12 meses (actividad física laboral - AFL; ejercicios físicos de ocio EFO; actividades de ocio y locomoción - AOL, y puntaje total - PT).
Resultados. Treinta y seis personas con EP participaron en el estudio (13 mujeres). El tiempo medio de diagnóstico fue mayor en los individuos clasificados en el grado moderado de la EP (2 - 3), comparado con los individuos en el grado leve (0 - 1,5) (p = 0,04). En los individuos con grado leve de la enfermedad, la regresión lineal mostró la asociación entre: a) fuerza de mano y el puntaje de EFO (R2 = 0,31; p = 0,013) y PT (R2 = 0,34; p = 0,009) de AFH; b) desempeño en la prueba "sentarse y levantarse" y PT (R2 = 0,46; p = 0,003) de la actividad física habitual.
Conclusión. Existe asociación entre el desempeño motor y PT de la AFH, en individuos en el grado leve de la EP. Los resultados sugieren que cuanto mayor es el PT de la AFH, mejor es la fuerza de mano y, más reducido es el tiempo de ejecución en la prueba de "sentarse y levantarse".
Objetive. To investigate the association between motor performance and habitual physical activity in individuals of mild and moderate stage of the Parkinson's disease (PD).
Method. This cross-sectional study involved subjects with PD, between stages 0 to 3 of the modified scale of Hoehn and Yahr. Motor performance tests used were: handgrip strength, evaluated by dynamometer (kg) and the test "chair stand" (seconds) (sit and standing test). The Baecke questionnaire analyzed the scores of habitual physical activity in the last 12 months (occupational physical activity - OPA; leisure time exercise - LTE; leisure and locomotion activity - LLA; and total score - TS).
Results. Thirty-six individuals with PD took part in the study (13 women). The time of the disease diagnosis was higher in individuals classified in moderate stage of PD (2-3) than in individuals on mild stage (0 -1.5) (p = 0.04). In individuals in the mild stage of the disease, the linear regression showed the association between: handgrip strength and the scores LTE (R2 = 0.31, p = 0.013) and TS (R2= 0.34, p = 0.009) of habitual physical activity; and performance in the "chair stand" test and TS (R2 = 0.46, p = 0.003) of habitual physical activity.
Conclusion. There is an association between the motor performance and total score of habitual physical activity in individuals with mild stage of the PD. The results suggest that the higher total habitual physical activity score, the better is the handgrip strength, and lesser is the runtime of "chair stand" test.
IntRODuCtIOn
Parkinson's disease (PD) is a chronic, progressive and neurodegenerative disorder of the central nervous system. It is characterized mainly by movement disorders, which in addition to the impairment of the motor performance, are responsible for the decreased physical activity1-3.
The severity and progression of PD symptoms differ among individuals4, and during the evolutionary process of the disease, individuals can present physical disabilities. Physical activity has been used and recommended as an important addition to the treatment of PD5-7, in order to prolong independence and improve the physical performance and activities of daily living. However, information on the physical activity patterns of individuals with PD are still scarce8,9.
The combination of some features of PD, such as decreased muscle strength and increased weakness, can lead individuals to restrict several daily activities and limit them to carry out strictly necessary activities, which can contribute to greater muscle atrophy and consequent decrease in functional capacity10.
The evaluation of the functional capacity can be accomplished by using measures of motor performance, with objective tests, analyzing individuals in standardized tasks according to predetermined criteria11-13. Tests such as the handgrip strength test and the "chair stand" test have been used in several studies examining the motor performance in individuals with PD14-17, primarily for its advantages such as convenience, low cost, reproducibility, and as markers for functional limitations; however, they do not associate performance to habitual physical activity.
Thus, the objective of this study was to investigate the association of motor performance and physical activity in individuals of mild and moderate stage of the PD.
MethODs
This cross-sectional study was conducted with 36 non-institutionalized volunteers (both sexes) with PD. Individuals diagnosed with Parkinson's disease (PD) between stages 0 to 3 (0 - 1.5, mild/2 - 3, moderate) of Hohen and Yahr's modified scale18, under treatment with L-Dopa and/or other medications (dopamine agonist or dopamine antagonist), were included in the study. In addition, individuals should present results > 24 on Mini Mental Evaluation (Mini Mental State Evaluation - MMSE)19.
These individuals were identified by their registration at Parkinson's Association of Santa Catarina (APASC), Santa Catarina state, southern Brazil. From this registration 75 individuals were contacted. Of these, thirty-one consented to undergo the evaluation, twenty-five refused, fifteen had contact error, four had died. In addition, five individuals with PD were contacted through the information of students at the University.
The study protocol was approved by an Ethics Committee and all participants provided informed consent.
Physical testing
The strength of the upper limbs was observed for maximum grip, measured by mechanical dynamometer (Takei Kiki Kogyio TK 1201, Japan). The test was performed using the dominant arm. During the test, the subject sat with his arms outstretched to the side, leaving the display of force directed outwardly. The individual should exercise the greatest possible strength. This procedure was performed twice with a short interval between executions (one minute), and the highest value (kg) was computed. The intraclass correlation coefficients of .91.
The test called "chair stand" (test-retest intraclass correlations of .88) was used to verify the strength of the lower limbs20,21. Prior to testing, the respondent was asked if he felt confident to rise quickly from a chair five times, without the help of the arms. In case of an affirmative answer, the subjects were asked to stay seated with the arms crossed over the chest, and get up five times as fast as possible, without any pause. The test was considered successful when performed in ≤ 60 seconds.
Habitual physical activity
The questionnaire of Baecke et al22, translated and validated in Brazil (intraclass correlation coefficients ≥ 0.69)23, verified the habitual physical activity in the last 12 months. To determine the total habitual physical activity score, the scores for occupational physical activity (OPA), leisure time exercise (LTE), leisure and locomotion activity (LLA) were summed. For questions left unanswered on the scales we adopted the average value of all questions of each respective score. In this questionnaire, the points of each score (OPA, LTE, LLA) can vary from 1 to 5, so the total score of habitual physical activity has minimum score of 3 and a maximum of 15. Where that the higher the score, the higher the level of habitual physical activity.
Although the questionnaire was originally standardized to be self-administered, in this study, it was applied in the form of an interview because of the characteristics of the disease that could hinder the filling.
Statistical analysis
Descriptive statistics procedures were performed (mean, standard deviation, median and minimum and maximum values) for determining the values related to handgrip strength, lower limb strength and habitual physical activity scores (OPA, LTE, LLA, and TE) of the last 12 months. After descriptive statistics, data normality was confirmed using the Shapiro-Wilk's test. To compare the statistical difference between the mean values of individuals diagnosed with PD, according to disease stage, we used the "t" Student test (independent samples), adopting the significance level of 5% (p < 0.05).
The linear regression technique was used to determine the association between the following: a) handgrip strength and habitual physical activity scores, according to the stage of the disease; and b) the performance on the "chair stand" test with habitual physical activity scores, according to the stage of the disease. The statistical significance level of 5% (p < 0.05) and CI 95% was adopted. Data analysis was performed with SPSS®, version 16.0.
Results
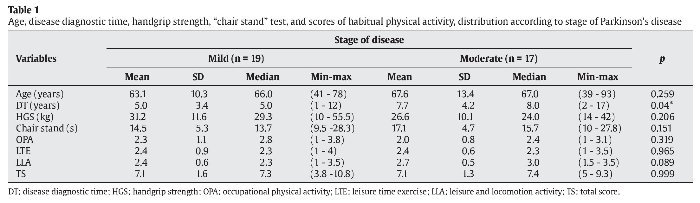
Thirty-six individuals with PD took part in the study (13 women). The age of the individuals varied from 39 to 93 years, with an mean of 65.2 ± 11.9 years. In relation to the stage of the disease of individuals, a variation of 0 to 3 was observed, in according to the modified scale of Hoehn and Yahr18, and the time of diagnosis of the disease ranged from 1 to 17 (6.22 ± 4.0) years.
Nineteen individuals were classified in the mild stage (0 to 1.5) and 17 in the moderate stage (2 to 3) of the disease. For the individuals in the mild PD stage, the period of diagnosis varied from 1 to 12 years, whereas for those in the moderate stage, it ranged from 2 to 17 years.
In the test "chair stand", two individuals of mild stage and three of moderate stage were unable to perform the test. Individuals in moderate stage present longer duration of the disease in relation to individuals on the mild stage (p = 0.04). There were no statistically significant difference in habitual physical activity scores (OPA, LTE, LLA, and TS), handgrip strength, "chair stand" test and age, according to the disease stage (table 1).

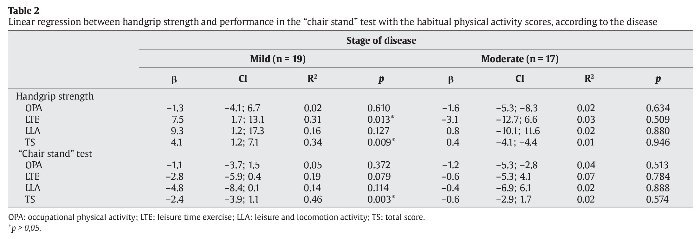
The results of simple linear regression analysis between the handgrip strength with each score of habitual physical activity (OPA, LTE, LLA, and TS), according to the disease stage are presented in table 2. Linear relationship was observed between handgrip strength and the LTE score (R2 = 0.31, p = 0.013) and TS (R2 = 0.34, p = 0.009) of habitual physical activity in individuals in the mild stage of the PD.

In terms of association between performance on test "chair stand" with each score of habitual physical activity (OPA, LTE, LLA, and TS), according to the stage of the disease (table 2), the results of simple linear regression analysis show association only between "chair stand" test with the TS (R2 = 0.46, p = 0.003) of habitual physical activity in individuals in the mild stage of the PD.
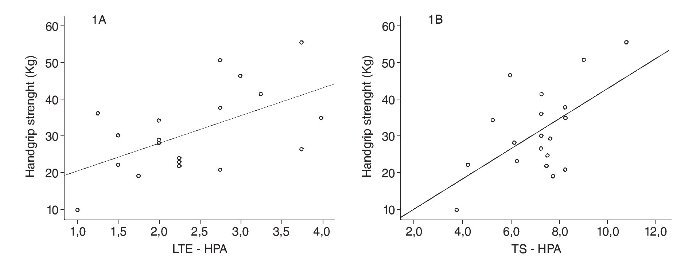
According to the results of the linear regression between the stages of the disease, there is growing trend among the handgrip strength with LTE score and with TS in individuals with mild stage of the PD, showing that the higher the value of the handgrip strength, the greater is the LTE score (fig. 1A) and the greater is the TS (fig. 1B). No significant association was observed between any score of habitual physical activity with the handgrip strength in individuals of moderate stage of the disease.

Fig. 1. A. Relation between the handgrip strength and leisure time exercise (LTE - HPA), in individuals in the mild stage of disease. B. Relation between the handgrip strength and total score of habitual physical activity (TS - HPA), in individuals with mild stage of disease.
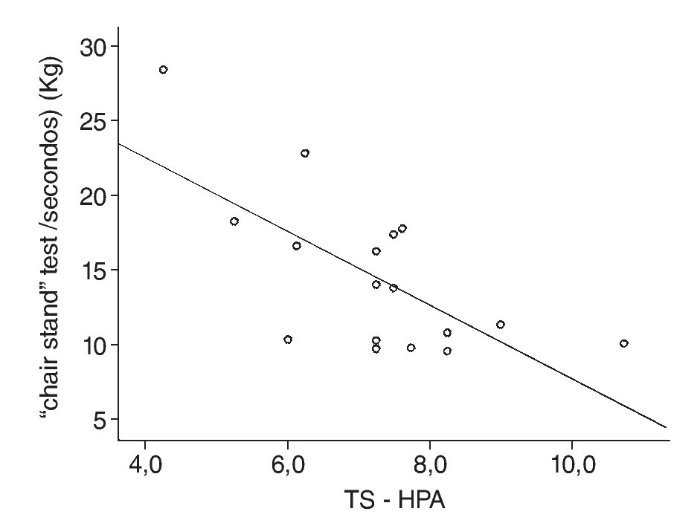
Figure 2 shows that when there is increase in the value of the total score of habitual physical activity, the run time of "chair stand" test in individuals with mild stage of the PD (negative trend) tends to be less. No significant association no was found between any score of habitual physical activity with performance testing "chair stand".

Fig. 2. Relation between the performance "chair stand" test and total score of habitual physical activity (TS - HPA), in individuals with mild stage of disease.
DIsCussIOn
The results of this study showed that the time of the disease diagnosis was higher in individuals classified in moderate stage in relation to individuals on mild stage of the PD, as expected. However, independent of stage of the disease, the habitual physical activity scores (OPA, LTE, LLA, and TS), were similar. Individuals in mild stage presented greater handgrip strength and best performance in the "chair stand" test, but without significant difference. Some studies show that changes in physical activity pattern8 and in muscle strength17,24 in individuals with PD, would occur only in advanced stages of the disease, and would not be easily identified among individuals in the early stages.
We observed linear relationship between the handgrip strength and LTE and TS scores of habitual physical activity and, between performance in the "chair stand" test and the total score of habitual physical activity in individuals with mild stage of the disease. The higher of total habitual physical activity score, the better the motor performance of individuals with mild stage of the PD. Handgrip strength (isometric) may not be sensitive enough to detect reduced power in subjects with PD, in the presence of bradykinesia25, since they present problem in the regulation of force and time parameters26. Furthermore, subjects with PD can present difficulties in simultaneous coordination of two or more motor tasks27 and difficulties of fine motor coordination28,29 in the upper limbs.
Individuals in mild and moderate stages of PD, may present greater difficulty in the functions of the lower limbs, for muscle strength and coordination, in relation to the upper limbs19. Because, while upper limbs are innervated only by brachial plexus, whereas the lower limbs are innervated by the lumbar and sacral plexus, involving largest amount of muscles. This can generate changes and problem of contraction between the muscles, muscle shortening, and increased muscle weakness30,31. In addition, individuals with PD may have greater recruitment in the number of motor units in low thresholds of muscle contraction, increasing co-activation of muscles antagonists, restricting the action of muscles agonists, which can reduce the force output of the lower limbs32.
In individuals with PD, the smallest muscle strength of lower limbs is associated with difficulty in making the move to sit and stand15,33, which can adversely affect the performance of daily activities and increase the risk of falls16,17. The study of Allen et al.10, involving 40 individuals with PD in mild and moderate stages, showed that the smallest muscle strength of lower limbs was associated with the decrease in speed of the walk and with the history of the falls.
Available information about on the physical activity for specific patterns of movements in the individuals with PD is still scarce. However, some studies9,34,35 pointed out that the combination of some features of PD, especially, reduction of muscular strength, fatigue, and changes in motion, are associated with less practice of physical activity at leisure, lower frequency of vigorous physical activity and less time on motor activity and performing daily tasks. However, limitations arising from the disease can be worked through regular practice of physical activities, mainly for prolonging the independence of individuals1-3,10.
In addition, it is known that the decreased levels of physical activity are associated with physiological changes that can result in decreased motor performance36. These physiological changes also are related to the increased vulnerability of cardiovascular conditions, metabolic disorders, skeletal muscles disorders and cerebrovascular disease, in addition to cognitive deficits and depression3,36.
There are some strengths and limitations that should be cited. This appears to be the first Brazilian survey to describe the habitual physical activity and its association with motor performance in individuals with PD. In the international literature, we found only one study8 that investigated differences in physical activity among individuals with and without PD, analyzing the pattern of sedentary behavior by accelerometer. Some studies investigated the performance motor of individuals with PD24,26,27,31, although, without associating the habitual physical activity. The habitual physical activity was assessed by indirect measurement using a questionnaire16, the unique way to assess physical activity in the past23. The study design does not establish cause and effect. Although the results show consistency in the associations and biological plausibility. Another limitation is the mean age of the participants.
In conclusion, there is an association between the motor performance and total score of habitual physical activity in individuals with mild stage of the PD. The results suggest that the higher total habitual physical activity score, the better is the handgrip strength, and lesser is the runtime of "chair stand" test. It is recommended that individuals with PD, increase their physical activity patterns, because they can maintain or improve motor performance, especially in the early stages of the disease.
ACknOwleDgMents
The authors would like to acknowledge to the Coordination of Improvement of Higher Education (Capes), for the master's scholarship grant to Guimarães, A.V., and participants on this research.
COnFlICt OF InteRest
The authors declare that they have no conflict of interest.
Correspondence:
A. Rodrigues Barbosa.
Departamento de Educação Física. Universidade Federal de Santa Catarina.
Campus Trindade - Florianópolis. Santa Catarina. Brasil - CEP 88040-900.
E-mail: aline.r.barbosa@ufsc.br; alinerb13@yahoo.com.br
