






The conformability of the stent, defined as the adaptation of the prosthesis to the natural shape of the vessel, is the major cause of geometrical changes after stenting and is influenced by the stent material and design. It may be assessed by measuring changes in the curvature and the angulation of the treated segment after stent implantation. The objective of this study was to compare changes in coronary angulation after implantation of the bioresorbable vascular scaffold (BVS) and cobalt-chromium and stainless steel metal platforms used in second-generation drug-eluting stents.
MethodsIn this retrospective analysis, 50 patients with single de novo lesions in native coronary arteries and diameter between 2.5 and 3.5mm and length up to 23mm were included. Twenty-five patients were treated with BVS and 25 patients were treated with cobalt-chromium (n=12) or stainless steel (n=13) platforms. Angulation was measured using a dedicated quantitative angiography analysis software.
ResultsVessel angulation significantly changed after device implantation. In the group submitted to the implantation of metal platforms there was greater coronary angulation change when compared to the group treated with BVS (41.6% vs. 14.9%; P<0.01). When we analyzed the performance of the BVS and the different metal platforms, coronary angulation change was greater for the stainless steel platforms, followed by cobalt-chromium platforms and the BVS (53.7% vs. 28.5% vs. 14.9%; P<0.01).
ConclusionsIn this preliminary assessment, the BVS produced a smaller coronary angulation change. The clinical impact of this finding must be prospectively investigated in a larger and more complex cohort.
Modificações na Angulação Coronária Após Implantede Suporte Vascular Bioabsorvível e de Stents de Cromo-Cobalto e Aço Inoxidável
IntroduçãoA conformabilidade do stent, definida como a adaptação da prótese à forma natural do vaso, é a principal responsável pelas alterações geométricas produzidas após o implante do dispositivo, sendo influenciada pelo material e pelo desenho do stent. Ela pode ser a ferida medindo-se as modificações da curvatura e a angulação do segmento tratado após o implante do stent. O objetivo deste estudo foi comparar as mudanças na angulação coronária após implante do suporte vascular bioabsorvível (SVB) e das plataformas metálicas de cromo-cobalto e aço inoxidável, utilizada sem stents farmacológicos de segunda geração.
MétodosForam incluídos, nesta análise retrospectiva, 50 pacientes com lesões únicas, de novo, em coronárias nativas, com diâmetro entre 2,5 e 3,5mm e extensão de até 23mm. Vinte e cinco pacientes foram tratados com SVB e 25 pacientes com plataformas metálicas de cromo-cobalto (n=12) ou de aço inoxidável (n=13). A angulação foi medida usando um software de angiografia coronária quantitativa dedicada.
ResultadosA angulação do vaso modificou-se significativamente após o implante dos dispositivos. No grupo submetido ao implante de plataformas metálicas, houve maior modificação do ângulo coronário quando comparado ao tratado com SVB (41,6% vs. 14,9%; P<0,01). Quando observado o comportamento do SVB e das diferentes plataformas metálicas, a alteração do ângulo coronário foi maior para as plataformas de aço inoxidável, seguida das plataformas de cromo-cobalto e os SVB (53,7% vs. 28,5% vs. 14,9%; P<0,01).
ConclusõesNesta avaliação preliminar, o SVB produziu uma menor mudança da angulação coronária. O impacto clínico deste achado necessita ser investigado prospectivamente em uma coorte maior e mais complexa.
The rectification of a curved segment of a vessel after stenting can modify the dynamics of blood flow and of the shear stress, and may be responsible for changes in the distribution of intra-stent intimal hyperplasia.1,2
The conformability of the stent, defined as its adaptation to the natural shape of the vessel, is the main responsible for the geometrical changes produced after stenting,3 and the two main determinants of conformability are the material and the design of the stent.4,5 This factor can be gauged by measuring the curvature and angulation of the target segment after stent implantation. A previous trial demonstrated that bioresorbable vascular scaffolds (BVS) have better conformability than that stents with metal platforms.6
The present study aimed to compare the changes in coronary angulation with a specific methodology for patients treated with three different devices: BVS and metal platforms of cobalt-chrome and stainless steel, used in second-generation drug-eluting stents.
METHODSThis is a retrospective, single-center trial conducted at the Department of Invasive Cardiology of Institute Dante Pazzanese de Cardiologia, São Paulo, Brazil. The population included patients consecutively treated at different moments, with ABSORB® BVS (Abbott Vascular – Santa Clara, United States), BioMatrix® stent (Biosensors Inc. – Newport Beach, United States), and Xience V® stent (Abbott Vascular – Santa Clara, United States), as part of local protocols.
In general, the patients included had stable or unstable angina, or were asymptomatic with objective signs of ischemia, with single de novo lesions in native coronary arteries with stenosis is between 70 and 90% (visual estimate) and reference diameters (RDs) between 2.5 and 3.5mm. The maximum permitted length of the lesion was 23mm. Patients with acute myocardial infarction <72 hours, lesions in left main coronary artery, ostial lesions, lesions with thrombi, lesions with excessive calcification that required atheroablative techniques before device implantation, and bifurcation lesions with lateral branch >2.0mm were excluded.
Study devicesABSORB® BVS is a balloon-expandable device comprising a polymeric scaffold of poly-L-lactic acid (PPLA), covered by a thin layer of amorphous matrix of poli-D, L-lactic acid containing 100μm2 of everolimus. The rods of this device are 150μm thick, and its cells have a zigzag format, interconnected by three longitudinal bridges. Although radio transparent, this BVS has a tag of platinum on each end, which allows for the angiographic viewing of its boundaries. Xience V® stent consists of a platform of cobalt-chrome with biocompatible fluoropolymer and with everolimus at a concentration of 100μm2, with a rod thickness of 81μm, associated with a polymer thickness of 7.6μm. Otherwise, BioMatrix® stent has a stainless steel platform and rods with a thickness of 112μm covered with a biodegradable polymer of polylactic acid (PLA) containing biolimus A9 (15.6μg/cm).
ProcedureThe lesions were treated with standard intervention techniques, which included an obligatory pre-dilation with a shorter balloon and with a diameter 0.5mm smaller than the device used. The post-dilation, which was carried out at the discretion of the surgeon, should be performed with noncompliant balloons at least 30% shorter than the implanted stent or BVS.
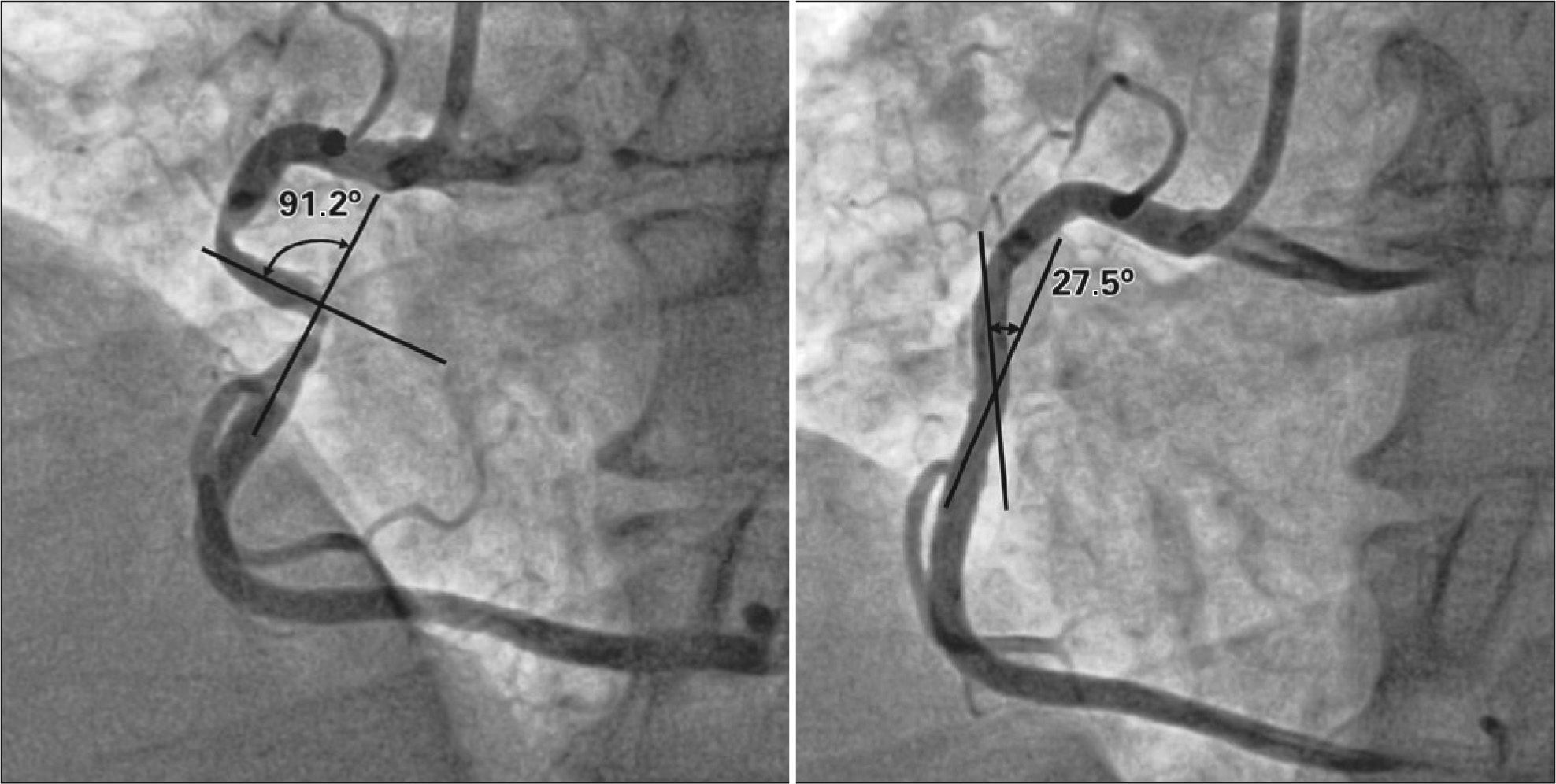
Angiographic analysisAfter administration of intracoronary nitroglycerin, serial angiographic studies were obtained in two corresponding orthogonal projections, at pre- and postprocedure. An angiographic analysis was performed off-line by experienced operators at Instituto Dante Pazzanesede Cardiologia, using validated software for quantitative coronary analysis (QAngio XA version 7.3; Medis – Leiden, the Netherlands). The minimal lumen diameter (MLD) and the RD, obtained from an average of the proximal and distal 5mm to the target lesion, were used to calculate the stenosis diameter [SD=(1 – MLD/RD)×100]. The acute gain was obtained from the difference between MLDs before and after the procedure. For the evaluation of angulation, the angiographic projection with the least shortening of the vessel and the least overlapping of images was used. The angles were obtained using a specific tool, a digital compass, attached to the quantitative analysis system, which was positioned within the target segment at the level of pre-procedure MLD. Then, the angle was determined by measuring the inner angle between the centered lines drawn on the proximal and distal coronary segments adjacent to MLD. The angles of the lesions were measured during diastole on the same projections before and after the procedure. (Figure)
Statistical analysis
Categorical variables were presented as absolute numbers and percentages, whereas continuous variables were described as means and standard deviations. Quantitative variables were analyzed by the nonparametric Mann-Whitney test (two groups) or the Kruskal-Wallis test (three groups). The association between categorical variables was evaluated by chi-squared or Fisher’s exact test. The Spearman correlation was used to determine whether there was a correlation between the pre-treatment angiographic variables (MLD, RD, SD, lesion length, and angle of the lesion) and the relative change between the angles before and after the procedure.
RESULTSThe present study evaluated 50 patients undergoing elective angioplasty, 25 treated with ABSORB® BVS, 12 with cobalt-chrome stent (Xience V®), and 13 with a stainless steel stent (BioMatrix®). The clinical characteristics are summarized in Table 1. There was no significant difference among groups regarding clinical characteristics, except for a higher prevalence of prior myocardial infarction among those treated with bare-metal stents.
Clinical characteristics
| Characteristics | BVS(n=25) | Metal platforms(n=25) | Cobalt-chromium platform(n=12) | Stainless steel platform(n=13) | P value* | P value** |
|---|---|---|---|---|---|---|
| Age, years | 56.8±7.0 | 60.4±8.1 | 59.8 (10.3) | 61 (4.8) | 0.16 | 0.33 |
| Male, n (%) | 15 (60) | 15 (60) | 6 (50.0) | 9 (69.2) | >0.99 | 0.39 |
| Hypertension, n (%) | 19 (76) | 20 (80) | 9 (75) | 11 (84.6) | >0.99 | 0.82 |
| Diabetes mellitus, n (%) | 5 (20) | 1 (4) | 0 | 1 (7.7) | 0.19 | 0.28 |
| Smoking, n (%) | 3 (12) | 4 (16) | 1 (8.3) | 3 (23.1) | >0.99 | 0.57 |
| Dyslipidemia, n (%) | 19 (76) | 16 (64) | 8 (66.7) | 8 (61.5) | 0.54 | 0.66 |
| Previous infarction, n (%) | 5 (20) | 15 (60) | 7 (58.3) | 8 (61.5) | <0.01 | 0.01 |
BVS=bioresorbable vascular scaffold.
The most often approached target vessel in the group treated with BVS was the left anterior descending artery, while in the groups treated with metal stents, the most often approached vessel was the left circumflex artery (P=0.09). Pre-procedural angiographic analyses showed no difference among the groups regarding the variables analyzed, including the RD of the target vessel and the lesion length. After the procedure, patients treated with BVS showed smaller MLD and acute gain compared to bare-metal stents (Table 2).
Angiographic and procedural characteristics
| Characteristics | BVS(n=25) | Metal platforms(n=25) | Cobalt-chromium platform(n=12) | Stainless steel platform(n=13) | P value* | P value** |
|---|---|---|---|---|---|---|
| Target vessel, n (%) | 0.09 | 0.24 | ||||
| LADA | 13 (52) | 7 (28) | 3 (25) | 4 (30.8) | ||
| LCx | 4 (16) | 11 (44) | 5 (41.7) | 6 (46.2) | ||
| RCA | 8 (32) | 7 (28) | 4 (33.3) | 3 (23.1) | ||
| Pre-procedure | ||||||
| Lesion length, mm | 11.7±4.0 | 11.6±5.0 | 10.1±3.4 | 12.9±5.9 | 0.54 | 0.31 |
| Reference diameter, mm | 2.62±0.45 | 2.60±0.41 | 2.73±0.36 | 2.49±0.44 | 0.79 | 0.34 |
| Minimum luminal diameter, mm | 0.87±0.32 | 0.84±0.36 | 0.90±0.25 | 0.78±0.44 | 0.73 | 0.52 |
| Stenosis diameter, % | 66.7±10.5 | 68.5±11.2 | 67.0±9.2 | 70.0±13.0 | 0.53 | 0.79 |
| Post-procedure | ||||||
| Minimum luminal diameter, mm | 2.39±0.31 | 2.68±0.36 | 2.66±0.26 | 2.69±0.45 | <0.01 | 0.03 |
| Stenosis diameter, % | 8.4±4.0 | 6.9±3.6 | 8.2±4.2 | 5.6±2.5 | 0.17 | 0.58 |
| Acute gain, mm | 1.51±0.41 | 1.83±0.36 | 1.76±0.28 | 1.9±0.42 | <0.01 | 0.02 |
BVS=bioresorbable vascular scaffold; LADA=left anterior descending artery; LCx=left circumflex artery; RCA=right coronary artery.
The angulation of the vessel changed significantly after implantation of the devices (Table 3). In the groups undergoing implantation of metal platforms, there was a greater relative modification of coronary angle when compared to those treated with BVS (41.6% vs. 14.9%; P<0.01). When observed the behavior of BVS and of the different metal platforms, the change of the coronary angle was greater for the stainless steel platform, followed by the cobalt-chromium platform and BVS (53.7% vs. 28.5% vs. 14.9%; P<0.01).
Modification of angles within and among groups
| Device | Pre-treatment (grades) | Post-treatment (grades) | Absolute change (grades) | Relative change (%) | P value* |
|---|---|---|---|---|---|
| BVS | 16.5±15.5 | 13.0±10.0 | 3.6±10.8 | 14.9 | 0.02 |
| Metal platforms | 20.2±15.6 | 11.4±12.7 | 8.9±9.6 | 41.6 | <0.01 |
| P value** | 0.22 | 0.32 | <0.01 | <0.01 | |
| BVS | 16.5±15.6 | 13.0±10.0 | 3.6±10.8 | 14.9 | 0.02 |
| Cobalt-chromium platform | 17.2±17.1 | 9.8±11.7 | 7.5±11.7 | 28.5 | 0.03 |
| Stainless steel platform | 23.0±14.2 | 12.9±13.9 | 10.1±7.4 | 53.7 | <0.01 |
| P valueb | 0.14 | 0.49 | <0.01 | <0.01 |
BVS=bioresorbable vascular scaffold.
The only pre-intervention angiographic variable associated with the relative change between angles before and after the procedure was the angle of the lesion before the intervention (P<0.01), as shown in Table 4.
Correlation between angiographic variables pretreatment and relative change between the angles before and after the procedure
| Variable | Correlation | P value |
|---|---|---|
| Lesion length | 0.13 | 0.38 |
| Reference diameter | 0.24 | 0.88 |
| Minimal luminal diameter | 0.12 | 0.43 |
| Stenosis diameter | 0.04 | 0.77 |
| Angle of the lesion | 0.68 | <0.01 |
In the present study, it was observed that both the metal platforms as BVS significantly changed the angle of the lesion after the procedure. In addition, the smallest angle modification occurs with BVS, followed by cobalt-chrome and stainless steel platforms. The only angiographic variable associated with a relative change between the angles was the angle of the lesion before the intervention.
The efficacy and safety of stents depend, in part, on their mechanical characteristics. A previous trial, which evaluated the mechanical properties of 17 metal stents analyzed the traction force between tortuosities, flexibility and conformability, and demonstrated that these properties depend on the design and material of the stent.7 The comparison of the mechanical performance of seven stents showed differences among the various platforms, with BioMatrix® stent showing less flexibility than Xience V® stent (30.06N/mm2 and 25.78N/mm2, respectively).4 Another trial evaluating the conformability of BVS and Xience V® stents observed that the bioresorbable platform is more advantageous, because the curvature and angle of the treated vessel are less altered.
Curved vessels have a greater association with turbulent flow and non-uniform distributions of shear stress, and the outer curvature of the vessel is subjected to stress greater than the inner curvature. Regions with low shear stress have been associated with the development of a thicker neointimal hyperplasia in both bare stainless steel stents2 and drug-eluting stents.8 A one-year follow-up of BVS stents showed a restoration of coronary anatomy close to that observed before the procedure, and with a probable restoration of a more physiological pattern of blood flow and of shear stress.9
A study on patients treated with bare-metal stents demonstrated that the location of the target lesion in a coronary segment with angle >33.5°, as well as a change in coronary angulations >9.1° after the device implantation, were independent predictors of greater cardiac events and of restenosis.10 Conversely, a study with 289 patients treated with drug-eluting metal stents failed to demonstrate an association between coronary angulation or vascular geometry modification with the occurrence of adverse events (target vessel failure, target vessel revascularization, or in-hospital infarction), after one year of follow-up.11
The new generations of drug-eluting stents, with more flexible alloys, thinner platforms, and better conformability, have the ability to change less intensely the coronary geometry, compared with older stents. Although BVS are superior to current metal stents in terms of conformability, and considering that these differences are very subtle, studies with more cases and with long-term follow-ups are needed to confirm the clinical benefits of these findings.
LimitationsAs the main limitations of this trial, the authors highlight its nonrandomized design, the small population included in each group, and the limited complexity profile of the lesions.
CONCLUSIONSIn this preliminary evaluation, the implantation of everolimus-eluting BVS showed a lesser change in the coronary angulation compared to cobalt-chromium and stainless steel platforms. For now, the clinical impact of this finding is unclear and needs to be prospectively investigated in a larger and more complex cohort.
CONFLICTS OF INTERESTThe authors declare no conflicts of interest.