


Studies comparing percutaneous and surgical methods for the treatment of the patent ductus arteriosus (PDA) are rare in the literature. This study aimed to perform a comparative analysis between both PDA treatment methods with emphasis on efficacy and morbidity.
MethodsObservational study with 2 cohorts of children and adolescents>5kg and<14 years of age with PDA, treated under a study protocol to assess the incorporation of novel technologies to the Brazilian Public Health System (Unified Health System−SUS) at an excellence hospital, in partnership with the Brazilian Ministry of Health. A prospective analysis was conducted for the percutaneous group from 2009 to 2011 and a retrospective analysis was performed for the surgical group between 2006 and 2011.
ResultsEighty patients were included in the percutaneous group (60% female) and 39 patients in the surgical group (51% female; P=0.37). The median age and weight of the percutaneous and surgical groups was 39.4months vs 25.5months (P=0.04) and 14kg vs 11.1kg (P=0.052), respectively. In the percutaneous group, 78 patients (92%) had type A PDA and the minimal ductal diameter at angiography was 2.5±1.2mm. Amplatzer®, Gianturco coils and Cera™ were the most commonly used devices. Clipping was the most commonly used surgical technique. The success rate of the procedure was 100% in both groups. The surgical group had higher complication rates, including chylothorax, infections, transfusions, systemic arterial hypertension, use of opioids and a greater need for intensive care. The median hospitalization time was 1.3days in the percutaneous group and 7.9days in the surgical group (P<0.01). Upon discharge, occlusion rates were similar in both groups (91% in the percutaneous group and 87% in the surgical group; P=0.71).
ConclusionsDue to the lower morbidity, the shorter hospitalization time and similar efficacy, percutaneous treatment of the PDA should be considered the modality of choice for selected patients.
Tratamento Percutâneo vs. Cirúrgico da Persistência do Canal Arterial em Crianças e Adolescentes
IntroduçãoEstudos comparando os métodos percutâneo e cirúrgico no tratamento da persistência do canal arterial (PCA) são raros na literatura. Nosso objetivo foi realizar análise comparativa entre os dois métodos de tratamento da PCA, enfatizando os aspectos de eficácia e morbidade.
MétodosEstudo observacional com 2 coortes de crianças e adolescentes>5kg e<14 anos, portadores de PCA, tratados durante um projeto de avaliação de incorporação de novas tecnologias ao Sistema Único de Saúde (SUS), realizado em um hospital cardiológico de excelência, em parceria com o Ministério da Saúde do Brasil. Foi feita análise prospectiva no grupo percutâneo entre 2009 e 2011 e retrospectiva no grupo cirúrgico entre 2006 e 2011.
ResultadosForam incluídos 80 pacientes no grupo percutâneo (60% do sexo feminino) e 39 no grupo cirúrgico (51% do sexo feminino; P=0,37). A mediana de idade e de peso dos grupos percutâneo e cirúrgico foi de 39,4 meses vs. 25,5 meses (P=0,04) e de 14kg vs. 11,1kg (P=0,052), respectivamente. No grupo percutâneo, 78 pa-cientes (92%) tinham PCA do tipo A e o diâmetro mínimo do canal à angiografia foi de 2,5±1,2mm. As próteses mais utilizadas foram Amplatzer®, molas de Gianturco e Cera™. A técnica cirúrgica mais utilizada foi a clipagem. A taxa de sucesso dos procedimentos foi de 100% nos dois grupos. O grupo cirúrgico apresentou maiores taxas de complicação, incluindo quilotórax, infecções, necessidade de hemoderivados, hipertensão arterial sistêmica e uso de opioides, como também maior necessidade de terapia intensiva. A mediana do tempo de internação foi de 1,3 dia no grupo percutâneo e de 7,9 dias no grupo cirúrgico (P<0,01). À alta hospitalar, as taxas de oclusão foram semelhantes nos dois grupos (91% no grupo percutâneo e 87% no grupo cirúrgico; P=0,71).
ConclusõesEm decorrência da menor morbidade, do menor tempo de internação e da igual eficácia, o tratamento percutâneo da PCA deve ser considerado a modalidade terapêutica de escolha para pacientes selecionados.
Patent ductus arteriosus (PDA) is one of the most frequent congenital cardiopathies, accounting for up to 7% of all congenital heart disease. 1,2 Its treatment is indicated in the first year of life in the presence of heart failure, or later when there are hemodynamic effects characterized by increased left ventricular dimensions on echocardiography. 3 The timely closure of PDA prevents the appearance of complications such as heart failure, pulmonary hypertension, arrhythmias, and possibly infectious endarteritis. 1,2
Surgical correction of PDA by lateral thoracotomy without the use of cardiopulmonary bypass was introduced in the late 1930s, and has been used with very good results. 4 However, this approach is associated with significant chest pain and a hospital stay of three to five days and results in a permanent chest scar. In the past 15 years, percutaneous treatment of PDA with latest-generation intracardiac prostheses has been performed with extreme safety and efficacy in various age groups, excluding newborns and young infants weighing less than 4 to 5kg.
There is a scarcity of comparative studies of percutaneous and surgical treatment of PDA. Although the few published studies have some methodological limitations, they unanimously demonstrate that the percutaneous approach has an efficacy similar to that of the surgical approach and is associated with a lower incidence of complications. 5,6 Thus, percutaneous treatment is becoming the method of choice for the treatment of congenital heart disease in most centers worldwide.
In Brazil, although there are several observational studies reporting excellent results of percutaneous treatment of PDA with different techniques, 3,7−9 studies comparing percutaneous treatment with surgical treatment are nonexistent. This study aimed to compare the safety and efficacy outcomes of percutaneous and surgical treatment of PDA. The study was performed in a cardiology hospital of excellence during the implementation of a project conducted together with the Ministry of Health to review the incorporation of new technologies within the Brazilian Unified Health System (Sistema Único de Saúde−SUS). 10
METHODSThe present study was an observational clinical trial in which two cohorts of children and adolescents with PDA with hemodynamic consequences were evaluated. The costs of hospitalisation and materials were subsidized by the government project.
For comparison purposes, the patients were divided into two groups: those who received percutaneous treatment with intracardiac prostheses (percutaneous group) and those who underwent conventional cardiac surgery (surgical group). After project approval by the Brazilian Ministry of Health in 2009, each patient was assigned to one of the two groups at the discretion of the attending physician.
Before 2009, the treatment offered to patients by the hospital philanthropic care project was exclusively surgical. The cohort of patients treated with the percutaneous procedure was evaluated prospectively, and the data were compared with data from a historical cohort of contemporary patients undergoing surgical treatment. Data from the latter cohort were retrospectively analysed after data collection from medical records covering the period between 2006 and 2011.
The study was approved by the research ethics committee of the hospital. The patients’ parents or tutors were adequately informed of the risks and benefits of the percutaneous procedure and signed an informed consent for the procedure.
Patients selected for this study weighed≥5kg, were≤14 years old, and had indication for PDA closure, i.e., left chamber overload at echocardiography. The percutaneous group included patients with PDA favorable to prosthesis implantation; these patients had no coexisting intracardiac disease that required surgical treatment. An exclusion criterion for the percutaneous group was PDA with unfavorable anatomy for percutaneous treatment. This was defined by the interventional professional after aortography using a view considered appropriate for assessment of PDA. Patients with low body weight (< 10.8kg) or with large PDA, in whom the placement of a device could lead to protrusion and obstruction of the left pulmonary artery and/or aorta, were considered as having unfavorable characteristics. Patients with PDA and normal left ventricular dimensions, except in the case of earlier endarteritis, were excluded from both groups.
The techniques used in both groups have been described in previous studies. 3,4 Patients in the percutaneous group received intravenous anaesthesia with orotracheal intubation, prophylactic antibiotic therapy (cefuroxime 30–50mg/kg, three doses) and heparin (100 units/kg), followed by left and right heart catheterisation. Angiograms were performed in left and/or left oblique view (100 to 110 degrees) with slight cranial angulation and/or right anterior oblique view to better define the anatomical defect.
The following types of prostheses were used: Amplatzer Ductal Occluder ® (St. Jude Medical, St. Paul, USA), 3,11 a device approved for clinical use by the Food and Drug Administration (FDA) of the United States; Amplatzer Ductal Occluder II ® (St. Jude Medical, St. Paul, USA), 12 a second-generation prosthesis, also designed for closure of PDA and approved by the FDA; it incorporates some structural changes to make it more flexible and suitable for specific types of PDA; Amplatzer Vascular Plug II (AVP II®, St. Jude Medical−St. Paul, USA), 8 a device designed to occlude peripheral vessels but also used in PDA occlusion in lower-weight infants; Nit-Occlud ® (PFM Medical−Cologne, Germany), 13 a controlled-release coil approved by the FDA; Cera™ PDA (Lifetech−Shenzen, China), 9 a nitinol-occluding prosthesis with a ceramic coating over metal mesh, designed for closure of PDA of diameter>2.5mm; and the Gianturco coil (Cook−Bloomington, USA), 7 a device that was initially applied in occlusion of peripheral vascular structures, which due to its high efficacy and safety, has been approved by the FDA for use in occlusion of PDA. All devices used in this study for the treatment of PDA have the approval of the National Health Surveillance Agency (Agência Nacional de Vigilância Sanitária−ANVISA).
The choice of prosthesis took into account PDA size and anatomy at angiography. In small PDAs (up to 2.5mm) and in types A, D, or E, the choice was the Gianturco coil or Nit-Occlud® of the flexible type; these devices were implanted using a retrograde approach. The diameter of the coil was at least two times the minimum diameter of the duct, with sufficient length to form at least three loops. In the presence of larger PDAs (> 2.5mm), nitinol occluders (Amplatzer® or Cera™) or medium-sized Nit-Occlud® prostheses were used; these devices were inserted using the anterograde approach. In patients who received these devices, the ductus arteriosus was crossed from the pulmonary trunk to the aorta, and a therapeutic coronary angioplasty catheter (usually Judkins right) or a long sheath of adequate calibre was positioned for implantation of the chosen prosthesis. The diameter of the Amplatzer® or Cera™ device was 1 to 3mm greater than the minimum diameter of the duct. In PDA types B and C, occluder prostheses were also selected.
Following the procedure, patients were extubated in the catheterisation laboratory except in the presence of complications or difficulties. Patients weighing less 10kg were taken to the intensive care unit (ICU) for recovery from anaesthesia and later transferred to the room or ward. Other patients were sent directly to the room/ward after an observation period of approximately 30 minutes in the post-anaesthesia recovery room of the operating room.
On the day following the procedure, patients underwent clinical evaluation that included routine laboratory tests, electrocardiography, chest radiography, and transthoracic echocardiography to evaluate the positioning of the prosthesis and the presence of possible residual flow. Patients who were clinically stable and without complications were discharged and given instructions that recapitulated the classic advice for endocarditis prophylaxis. Echocardiography, electrocardiography, and chest radiography were performed before hospital discharge and at clinical follow-up after 30 days, six months, and, when necessary, annually. In cases of ductal occlusion and cases that showed absence of complications such as pulmonary artery stenosis or aortic coarctation after six months, the patient was discharged from the paediatric cardiology service.
In the surgical group, procedures were performed under intravenously administered general anaesthesia without the use of extracorporeal circulation and with surgical access through the lateral route using the extrapleural or classical approach. The choice of technique for PDA closure was at the surgeon’s discretion and ranged from section and suture to ligature with metal clips. Following the procedure, patients were transferred to the ICU for routine recovery. After hospital discharge, most of these patients were followed-up at the service that originally referred them.
Efficacy was assessed based on the fraction of total occlusion before discharge and/or during follow-up. Morbidity was assessed by rates of complication and hospital stay. The following were considered major complications: death, cerebral embolism, cardiac perforation with tamponade, endocarditis, need for reintervention (surgical or percutaneous), pleural or pericardial effusion with need for surgical drainage, and need for surgery due to device embolisation or arterial occlusion. Minor complications included prosthesis embolisation with percutaneous removal, local hematoma at the venous puncture site, and arterial occlusion that improved with anticoagulants. The following were also considered as minor complications: anaemia requiring blood products, non-cardiac infection (bronchopneumonia, urinary tract infection, acute gastroenteritis, surgical wound infection), hypertension requiring drug treatment and varied respiratory problems (pulmonary oedema, atelectasis, mechanical ventilation>24 hours, post-extubation laryngitis).
Statistical analysis was performed using Sigmastat Rankings v.2011. Data are presented as absolute values and frequency, mean and standard deviation, or median and range according to the sample distribution. The chi-squared test or Fisher’s exact test was used for comparing frequencies, and Student’s t-test or the Mann–Whitney test was used to compare means or medians, respectively. P-values≤0.05 were considered to be statistically significant.
RESULTSDuring the study, 80 percutaneous procedures were performed for the closure of PDA. A total of 39 patients were identified in the surgical group during the study period. The distribution between genders was similar between groups, with 48 female patients (60%) in the percutaneous group and 20 (51%) in the surgical group (P=0.37). The median age was 39.4months (8.5months to 170 months) and 25.5months (4.7months to 170 months) in patients treated percutaneously and surgically, respectively (P=0.04). The median patient weight was 14kg (5–52kg) in the percutaneous group and 11.1kg (5–59kg) in the surgical group (P=0.052).
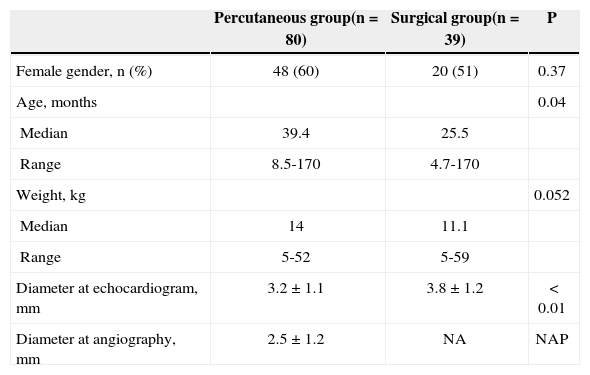
The diameter of the ductus arteriosus at echocardiography before the procedure was 3.2±1.1mm in the percutaneous group and 3.8±1.2mm in the surgical group (P<0.01). The angiographic characteristics of the PDA could only be obtained in the percutaneous group. In this group, 78 patients (92%) had PDA type A, and two were classified as type E, Krischenko. 14 The pulmonary end diameter in this group of patients was 2.5±1.2mm. Patients’ demographic data and PDA measurements are shown in Table 1.
Demographic data and measures of the ductus arteriosus
| Percutaneous group(n=80) | Surgical group(n=39) | P | |
|---|---|---|---|
| Female gender, n (%) | 48 (60) | 20 (51) | 0.37 |
| Age, months | 0.04 | ||
| Median | 39.4 | 25.5 | |
| Range | 8.5-170 | 4.7-170 | |
| Weight, kg | 0.052 | ||
| Median | 14 | 11.1 | |
| Range | 5-52 | 5-59 | |
| Diameter at echocardiogram, mm | 3.2±1.1 | 3.8±1.2 | < 0.01 |
| Diameter at angiography, mm | 2.5±1.2 | NA | NAP |
n=number of patients; NA=not available; NAP=not applicable.
Patients in the surgical group were referred for treatment without the need for catheterisation and angiograms; therefore, invasive assessment of pulmonary pressure was not performed. None of the patients had evidence of associated pulmonary hypertension. In the percutaneous group, the systolic pressures in the aorta and pulmonary trunk were 82.8±11.1mmHg and 28.8±7.8mmHg, respectively.
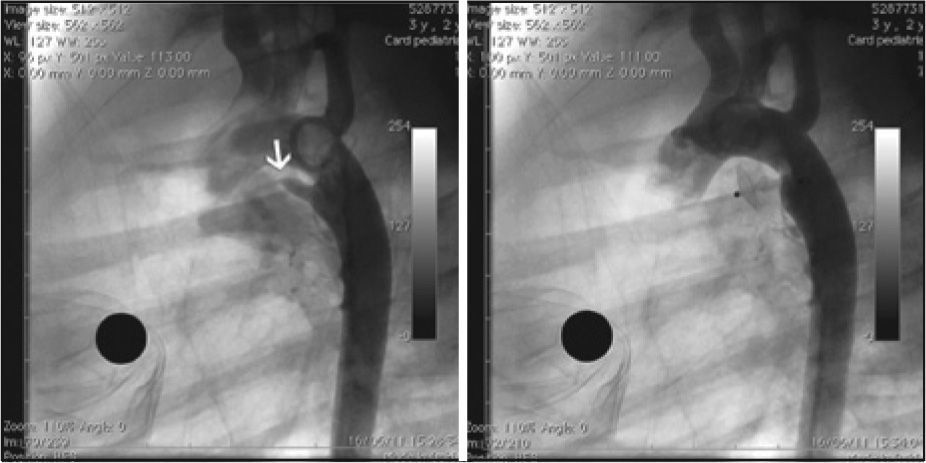
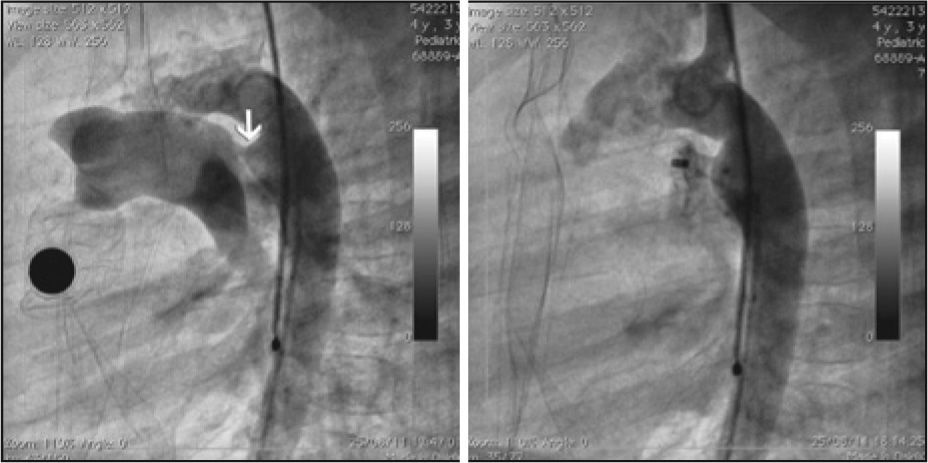
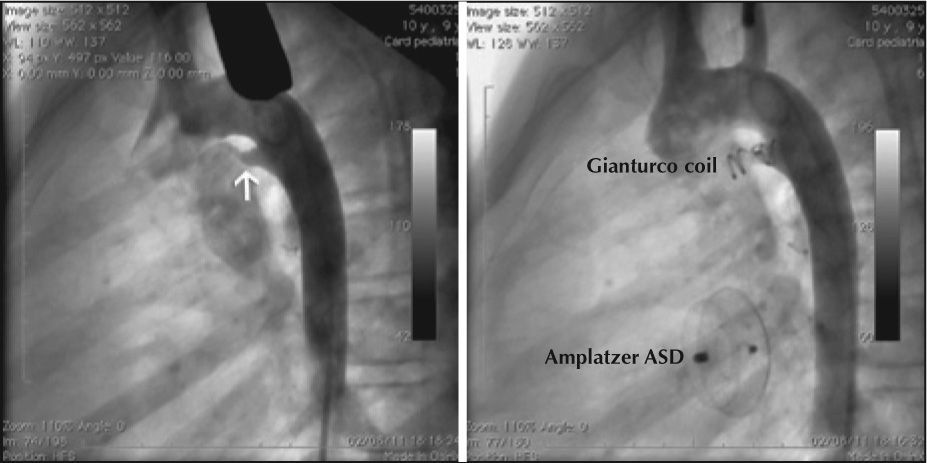
The percutaneous occlusion procedure was feasible in all patients taken to the catheterisation lab. Amplatzer® I or II prostheses for PDA were used in 28 patients (35%), the Gianturco coil was used in 24 patients (30%), and the Cera™ was used in 19 patients (24%). Nit-Occlud ® was used in seven patients, and the AVP prosthesis II was used in two other patients (Figures 1 and 2). Implantation was successful in all patients. One patient who received a Gianturco coil for PDA closure also underwent a 12-mm atrial septal defect repair with an Amplatzer ® device in the same procedure, without complications. The echocardiogram of this patient, performed 24 hours later, showed no residual flow (Figure 3).
, showing type A ductus arteriosus (arrow). On the right, control aortography showing ductus arteriosus occluded with an Amplatzer ® ADO II device, 4×4mm.")
 showing type A ductus arteriosus (arrow). On the right, control aortography showing ductus arteriosus occluded with a Cera™ prosthesis, 8×6mm.")
 showing ductus arteriosus type E (arrow). On the right, control aortography showing ductus arteriosus occluded with a Gianturco coil. An Amplatzer ® ASD device was used in the closure of the atrial septal defect in this patient.")
– On the left, aortography in left profile (90 degrees) showing ductus arteriosus type E (arrow). On the right, control aortography showing ductus arteriosus occluded with a Gianturco coil. An Amplatzer ® ASD device was used in the closure of the atrial septal defect in this patient.
There were no episodes of prosthesis embolisation. However, three patients who received the Gianturco coil had to undergo removal with a snare loop catheter soon after implantation due to initial inappropriate placement caused by the anomalous appearance of the device, most likely due to a manufacturing defect. New same-dimension coils were successfully implanted in two of the patients, and a smaller coil was used in the third patient at the same procedure, with excellent final positioning. In two procedures that used the Nit-Occlud ® device, immediate highvelocity residual flow was observed, and additional Gianturco coils were implanted, with significant flow reduction (Figure 4).
 showing type A ductus arteriosus (arrow). On the right, control aortography showing ductus arteriosus occluded with Nit-Occlud ® and Gianturco coil.")
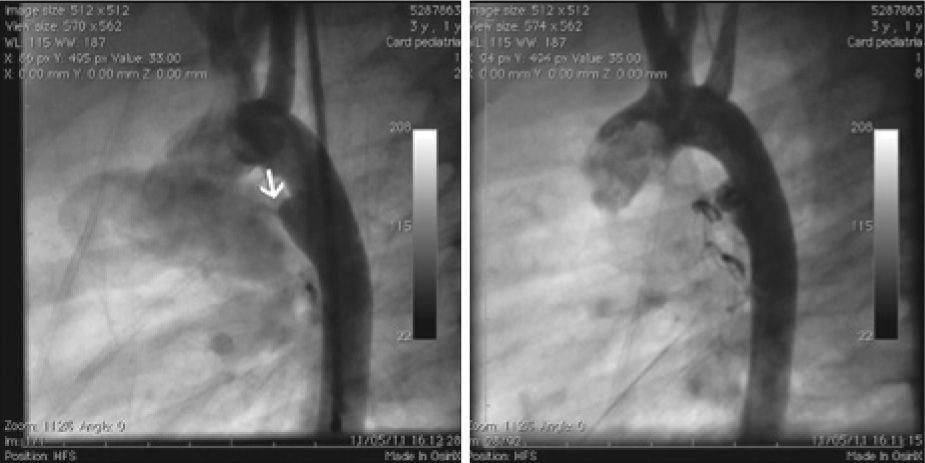
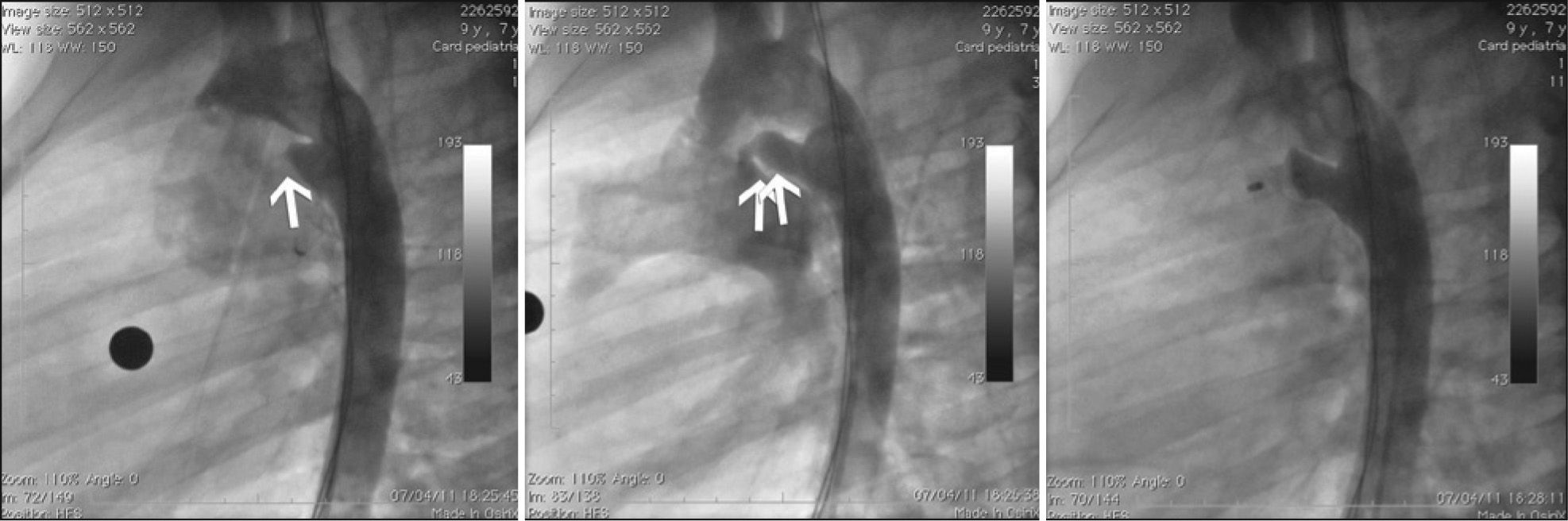
In one patient, there was an attempted use of a Nit-Occlud ® 4 x 4mm prosthesis via the retrograde approach because of the small size of the ductus arteriosus at the initial angiography. After several attempts without obtaining good positioning, it was observed that the ductus had larger dimensions than initially estimated. The Nit-Occlud ® device was replaced by a Cera™ 8 x 6mm device, which was implanted by the anterograde approach with excellent final results (Figure 5). The surgical approach was the classical lateral route in 17 (43%) patients and the extrapleural route in the other 22 patients (57%). Ligation of the ductus arteriosus with metal clips was used in 37 of 39 procedures (95%).
 showing a small type A ductus arteriosus (arrow). In the middle, subsequent aortography showing a larger diameter of the same ductus arteriosus (arrows). On the right, post-procedural angiography showing totally occluded ductus arteriosus with Cera™ prosthesis, 8×6mm.")
– On the left, aortography in left profile (90 degrees) showing a small type A ductus arteriosus (arrow). In the middle, subsequent aortography showing a larger diameter of the same ductus arteriosus (arrows). On the right, post-procedural angiography showing totally occluded ductus arteriosus with Cera™ prosthesis, 8×6mm.
The need for intensive care during post-procedural recovery occurred in all 39 patients in the surgical group and in 13 patients in the percutaneous group (P<0.01). The 13 percutaneous patients who recovered in the ICU were those weighing less than 10kg (mean of 9.2±5.6kg) with the exception of one, who had pneumothorax during anaesthetic induction. The pneumothorax was punctured and emptied at the hemodynamics lab without need for drainage. The patients’ ICU length of stay was 12 hours, and all patients’ ICU stays were uneventful.
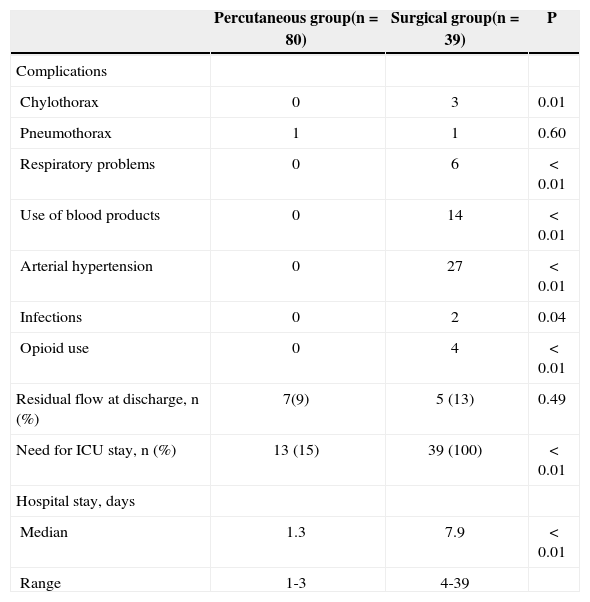
There were no deaths in either group. Several major and minor complications were observed more frequently in the surgical group (Table 2). In this group, hypertension requiring medication treatment occurred in 27 patients (68%), and blood transfusions were required in 14 patients (36%). No patients in the percutaneous group had hypertension or a need for blood transfusion (P<0.01 for both comparisons). In the surgical group, three (7.5%) patients developed chylothorax requiring prolonged fasting and parenteral nutrition. One of these patients, aged one year and weighing 7.8kg, was the patient with the longest hospital stay in this group (39days); in addition to chylothorax, this patient had a Staphylococcus aureus infection that was confirmed by positive blood culture. Pneumothorax requiring surgical drainage occurred in 1 patient, and one patient had a bilateral granuloma wound requiring two reoperations for treatment. The latter patient later developed a cutaneous fistula that spontaneously closed in the follow-up period.
In-hospital outcomes
| Percutaneous group(n=80) | Surgical group(n=39) | P | |
|---|---|---|---|
| Complications | |||
| Chylothorax | 0 | 3 | 0.01 |
| Pneumothorax | 1 | 1 | 0.60 |
| Respiratory problems | 0 | 6 | < 0.01 |
| Use of blood products | 0 | 14 | < 0.01 |
| Arterial hypertension | 0 | 27 | < 0.01 |
| Infections | 0 | 2 | 0.04 |
| Opioid use | 0 | 4 | < 0.01 |
| Residual flow at discharge, n (%) | 7(9) | 5 (13) | 0.49 |
| Need for ICU stay, n (%) | 13 (15) | 39 (100) | < 0.01 |
| Hospital stay, days | |||
| Median | 1.3 | 7.9 | < 0.01 |
| Range | 1-3 | 4-39 |
n=number of patients; ICU=intensive care unit.
The in-hospital effectiveness was similar between the two groups. Minimal residual flow at hospital discharge was found in 9% of the patients in the percutaneous group and in 13% of the patients in the surgical group (P=0.49).
The length of stay was significantly higher in the surgical group, with a median of 7.9days (four to 39 days) compared to 1.3days (one to three days) in the percutaneous group (P<0.01). During follow-up, complete PDA occlusion was observed in all patients in the percutaneous group, with no changes in aortic or pulmonary artery flow at echocardiography. Most patients treated in the surgical group were followed-up at the services from which they were referred; thus, it was not possible to obtain reliable follow-up data for these patients.
DISCUSSIONIn this non-randomized study of two contemporary cohorts of patients treated in the same center, percutaneous closure of PDA in infants>5kg, children, and adolescents was proven to be safer than and as effective as surgical treatment for this condition. It is unlikely that the younger mean age of the surgical group impacted the incidence and severity of observed complications, because the median weight of the patients in both groups was similar (14kg vs. 11.1kg; P=0.052). Furthermore, the median age of approximately 2 years and weight of 11kg of the surgical group patients are not usually considered risk factors for contemporary paediatric cardiac surgery, especially because closure of PDA is a technically simple surgery that does not require cardiopulmonary bypass. Conversely, the relatively lower weight of the children in the percutaneous group (14kg for children aged approximately 3 years) may reflect the greater hemodynamic effect of PDA in this group. A confounding factor in the present study was the larger mean diameter of the ductus arteriosus found in the surgical group on echocardiography. The authors believe that the best way to evaluate the ductus arteriosus is through angiography, and this procedure was performed only in the percutaneous group, precluding an accurate comparison between groups. However, it is likely that the higher incidence and greater severity of complications observed in the surgical group are associated with the invasive nature of cardiac surgery, which requires thoracotomy, rather than with the difference in mean diameter of the ductus arteriosus in the two groups.
The low morbidity observed in the percutaneous group reflects the use of a less invasive method and the team’s experience with this type of procedure, especially with regard to the selection of patients and the choice of size and type of device for the patient’s anatomy. The authors believe that the extremely low morbidity associated with the use of percutaneous treatment makes the use of an outpatient treatment system for patients with PDA feasible; typically, these patients do not require additional laboratory tests and can be discharged from the hospital after a brief rest and observation period of six to 12 hours. Wider use of the percutaneous procedure would result in significant savings of resources and would release hospital beds for other patients with more complex heart diseases that require intensive care and surgical correction.
Although a high implant success rate and a low incidence of complications were observed in this study, some qualifications should be noted. Device embolisation, although not observed in this series, is a complication that can occur during the practitioner’s learning curve and/or in patients who were not properly selected. The use of coils in PDAs with minimum diameters larger than 2.5-3mm and in PDA types B and C is often associated with embolisation and/or malapposition. 15 The need for removal of coils that were inadequately positioned in three patients of this series was due to manufacturing defects, which were rectified, and not to technical errors by the surgeons or inappropriate patient selection. In cases of embolisation, prosthesis recovery in the catheterisation lab is usually possible, as observed in previous studies. 7 Left pulmonary artery stenosis or coarctation of the aorta secondary to device protrusion is sometimes observed in small infants with large-diameter ductus arteriosus that requires the use of larger prostheses. 16 Although this team has not managed patients with these characteristics, they would have been referred for surgical treatment in this study. The occurrence of pneumothorax in a patient from the percutaneous group can be considered a case of an anaesthetic complication not directly associated with the catheterisation procedure. In the patient in whom it was necessary to exchange the device for a larger one, ductal spasm most likely occurred prior to implantation. This phenomenon can occur spontaneously or secondary to manipulation of the ductus arteriosus with a catheter or guidewire prior to angiography.
The occurrence of chylothorax requiring drainage and prolonged hospitalisation is occasionally observed after surgical correction of persistent ductus arteriosus, as observed in three patients in this study. Such complications, as well as the other respiratory problems found in six patients in this series, result from the need for thoracotomy with dissection of vascular structures and displacement of the left lung for ligation or section and PDA suture. Chylothorax, which was observed in one patient in this series, also increases postoperative morbidity through its association with infection secondary to immunosuppression and because it necessitates prolonged parenteral nutrition. In this study, a significant number of patients required blood transfusion after surgery, leading to increased indirect costs related to the use of blood products (blood typing, serology). Moreover, more than half of the patients in this study had hypertension after surgery. This is most likely due to manipulation of the aorta resulting in adrenergic discharge and pain associated with lateral thoracotomy and the stretching of nerve fibres, occasionally requiring the use of opioids, as observed in four patients in this series. Moreover, a longer hospital stay and a need for intensive care were observed in the surgical group, showing its greater morbidity. These needs increase hospital costs and limit the use of beds in the ICU and the surgical center by patients with complex heart diseases that require surgical correction. The burden imposed on healthcare systems by the exclusive use of surgical treatment of PDA becomes even more striking when the comparison is made in countries considered poor. 17
This study found high rates of in-hospital occlusion of PDA in both the percutaneous and surgically treated groups. Due to the progressive endothelialisation of the device, patients in the percutaneous group who were discharged with minimal residual flow showed complete occlusion during follow-up. This study observed high occlusion rates with the use of a variety of prostheses, suggesting that physicians are generally successful in choosing the appropriate size and type of prosthesis for the underlying anatomy. The planning of this study and the small number of patients involved did not allow for the comparison of the performance of each available type of prosthesis. Additionally, follow-up data on the patients who were treated surgically and were discharged with minimal residual flow was not available; however, the finding of late residual flow after ligation of the ductus is not infrequent. 18
Study limitationsThe most serious limitation of the present study is its non-randomized design. There are no non-randomized studies of this subject in the literature, and the performance of such a study is extremely unlikely. Currently, the percutaneous approach is so well established, standardized, and disseminated in the major world centers that recruitment of patients to a surgical group after randomization would be difficult to justify. It appears that the surgical approach should be reserved for premature and small infants (< 4–5kg) with large PDAs. Even in this subgroup of patients, percutaneous treatment has shown initial promising results. 19,20
Another limitation of the current study is that it did not include patients with type B, C, or D PDAs, which are rare. In addition, the mean minimum diameter of the ductus arteriosus in the patients in this study was relatively small, restricting the ability to extrapolate the results to other types of anatomy and defect sizes. Treatment of patients with type B or C PDAs is more challenging and may require alternative and unusual techniques. 21−25
The lack of outpatient follow-up of the patients in the surgical group, which is due to the retrospective nature of data collection in this group, is another limitation of this study. Conversely, although it was not randomized and thus introduced biases in patient selection, this study’s strong point is that it involved two practically contemporaneous cohorts, treated in a single hospital of excellence by experienced and relatively homogeneous teams, using well-established and standardized surgical and percutaneous techniques. The experience shown here most likely reflects one of the best clinical practices found in Brazil.
CONCLUSIONSBased on the data presented in this paper and on the existing evidence in the literature regarding its safety and efficacy, we believe that percutaneous closure of PDA should be considered the treatment of choice for selected patients with this condition. Because the cost of using Gianturco coils is already covered by the SUS, in Brazil it seems reasonable, relevant, and urgent to initiate studies to evaluate the cost-effectiveness of using nitinol occluders (Amplatzer®, Cera™, Lepu, Coccon, and Nit-Occlud®) in patients with PDAs greater than 2.5mm and of types B and C.
CONFLICTS OF INTERESTCarlos A. C. Stone is a consultant for St. Jude Medical, Inc. (St. Paul, MN, USA) and for Lifetech (Shenzhen, China). The other authors declare no conflicts of interest.