



We report the case of a neonate with ductus-dependent cyanotic congenital heart disease treated by stenting in the ductusarteriosus. A physician-modified stent angulation enabled the advance of the stent from the aorta to the ductus arteriosu and its subsequent implantation.
Angulação de Stent eImplante em Canal Arterial de Neonato com Baixo Peso
Relatamos o caso de um neonato portador de cardiopatia congênita cianótica canal-dependente com implante de stent no canal arterial. Uma modificação do stent realizada pelo intervencionista, criando-se um ângulo em seu corpo, possibilitou o avanço do stent da aorta até o canal arterial, e seu subsequente implante nesse sítio.
Neonates with ductus-dependent cyanotic congenital heart disease require, in addition to drug treatment (prostaglandin E1 infusion), measures to increase pulmonary blood flow, as well as surgical systemic-pulmonary shunt procedure (Blalock-Taussig).
The morbidity and mortality of this surgical procedure can be high, and in some cases, the stent implantation in the ductus arteriosus is a good alternative to surgical systemic-pulmonary shunt. The morphology of the ductus arteriosus in cyanotic congenital heart disease has great variability and may originate more proximally at the aortic arch, making it difficult, or even impossible, to advance the stent from the aorta to the ductus arteriosus through the usual percutaneous techniques.1
The authors report a case with physician-modified stent angulation, which enabled the stent to be advanced from the aorta up to the ductus arteriosus, and its implantation in a low-weight newborn with pulmonary atresia and ventricular septal defect, and contraindication for Blalock-Taussig shunt.
CASE REPORTA female neonate, born at term through normal delivery, weighing 2.1kg, with no prenatal diagnosis of heart disease, displayed central cyanosis (oxygen saturation of 80%) immediately after birth, systolic heart murmur at auscultation on the left sternal border ++/4+, single second heart sound, and normal peripheral pulses.
A transthoracic echocardiogram disclosed the presence of pulmonary atresia with ventricular septal defect (VSD) and patent ductus arteriosus (3-mm diameter). Endotracheal intubation and ventilation were started, as well as intravenous administration of prostaglandin E1.
The neonate developed peripheral oxygen saturation levels between 80% and 90%, renal failure (peak serum creatinine up to 2.3mg/dL), thrombocytopenia (40,000 platelets/mm3), pulmonary hemorrhage, and small intraventricular hemorrhage. She was evaluated by a heart surgery team, which contraindicated the performance of the systemic-pulmonary shunt due to high surgical risk (low weight, thrombocytopenia, and renal failure) and indicated stent implantation in the ductus arteriosus for initial palliation.
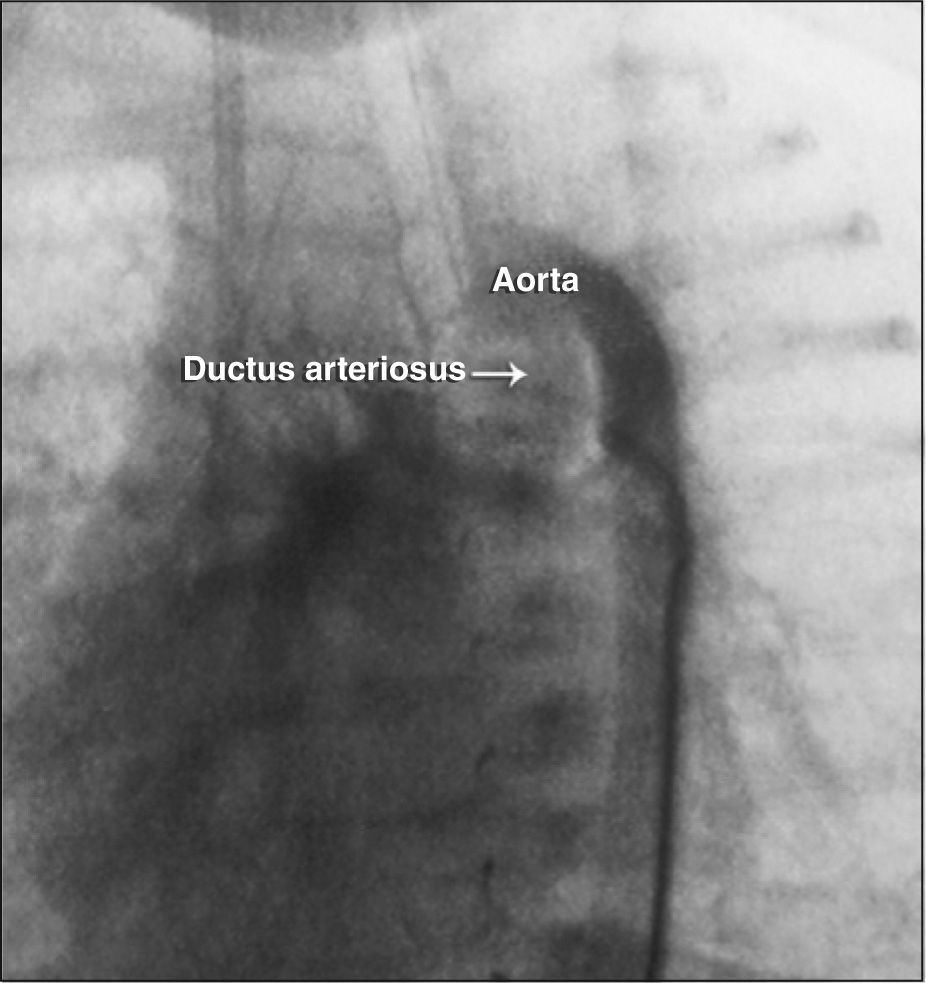
After the child showed clinical improvement, 15 days after birth, intravenous infusion of prostaglandin E1 was withdrawn two hours before the hemodynamic procedure was started, in order to reduce the ductus arteriosus size and facilitate stent implantation. Under general anesthesia, a puncture was performed in the right femoral artery and an 11-cm 4F valved sheath introducer (Cordis Corporation, NJ, United States) was inserted. Under fluoroscopy, thoracic aortography was performed using a Judkins right 4F catheter (Cordis Corporation, NJ, United States), which disclosed the presence of patent ductus arteriosus, originating from the aortic arch, with approximate diameter of 3mm and vertical trajectory (Figure 1). Aortopulmonary fistulas were not identified in this aortography.

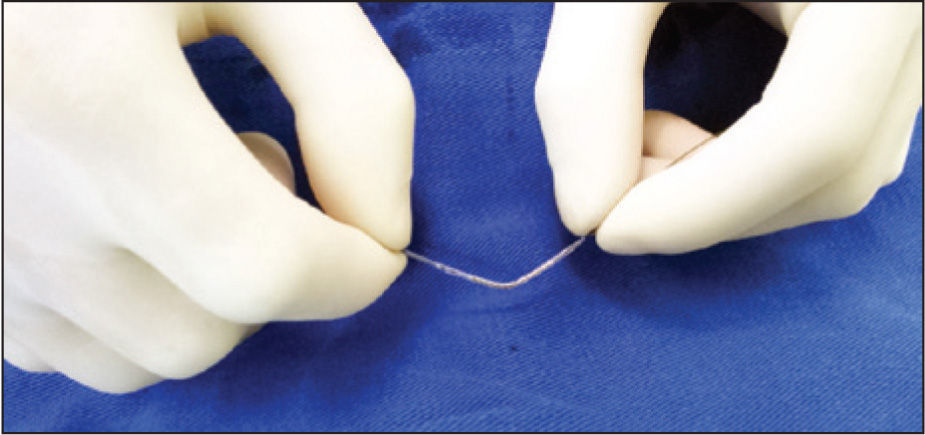
Subsequently, a pigtail 4F catheter (Cordis Corporation, NJ, United States) with its distal extremity cut, in order to obtain an “inverted J” catheter, was used to selectively catheterize the ductus arteriosus. A 0.014-inch Runthrough® NS guide wire (Terumo Corporation, Tokyo, Japan) was introduced through this catheter up to the ductus arteriosus, pulmonary trunk, and periphery of the pulmonary arterial bed. Without a diagnostic or therapeutic guide catheter, a 3.5×15mm Multi-Link Vision® coronary stent (Abbott Vascular, CA, United States) was introduced over the 0.014-inch guide wire. However, this first attempt at implantation was unsuccessful because of the 90° entry angle in the ductus arteriosus in relation to the aorta, which led the stent in the direction of the ascending aorta. It was decided to create a 45° angle in the mid-portion of the stent (Figure 2) to facilitate the passage of the stent from the aorta to the ductus arteriosus. The coronary stent with this angle was reintroduced over the guidewire and advanced from the aorta to the ductus arteriosus without resistance, without using a guide-catheter or long valved sheath introducer; the stent was implanted in the ductus arteriosus with a release pressure of 20atm. After the procedure, the aortography showed a well-positioned and expanded stent in the ductus arteriosus (Figure 3). It was administered 20mL of platelet concentrate and the valved sheath introducer was removed uneventfully. The child returned to the pediatric intensive care unit in stable clinical condition, with arterial oxygen saturation of 98%.
DISCUSSION
 in the ductus arteriosus.")
Neonates with ductus-dependent cyanotic congenital heart disease usually present with severe and complex clinical pictures and still represent a major diagnostic and therapeutic challenge.2
Stent implantation in the ductus arteriosus was originally described in 1992 by Gibbs et al.,3,4 with very encouraging initial results. Since then, several groups have published their experience, detailing the technique of stent implantation in the ductus arteriosus.1,5,6
Some exclude patients weighing less than 2.5kg, due to the risk of serious injury to the femoral arteries with use of long-valved 4F sheath introducers.1 For cases in which the ductus arteriosus originates more proximally in the aortic arch, as in pulmonary atresia with VSD, the intravenous route is the preferred approach for stent implantation in this group. They emphasize, however, the risk of total atrioventricular block, as the catheter rubs against the borders of the septal defect during its handling.
For cases of high surgical risk when undergoing a systemic-pulmonary shunt, as in this case, stent implantation in the ductus arteriosus is a good initial palliative measure. The stent modification, creating a 45° angle in its body was, in this case, decisive for the stent implantation in the ductus arteriosus, whose proximal origin of the aortic arch and peculiar trajectory make it also known as the “vertical” ductus arteriosus. This degree of stent angulation did not cause clinically detectable structural damage, nor did it result in modified behavior at insufflation or distortion at the implantation site.
The authors did not find in the medical literature a previously reported case of physician-modified stent angulation facilitating its implantation in the ductus arteriosus of a low-weight neonate with ductus-dependent cyanotic congenital heart disease. At the time of the writing of this report, three other neonates with ductusdependent congenital heart disease were successfully submitted to stent implantation in the ductus arteriosus using the technique described herein.
CONFLICTS OF INTERESTThe authors declare no conflicts of interest.