


To evaluate the effectiveness of an educational intervention with empowerment for patients with epilepsy in a Spanish reference hospital for epilepsy.
MethodsA nonrandomized clinical trial was designed in an epilepsy center. An empowerment group intervention program was conducted in which volunteers were recruited. The education contained common topics in health education in epilepsy, which was adapted to the demands of the patients. Patients were empowered to apply their knowledge and skills, using the nurse as a facilitator. Questionnaires were administered before and after the intervention to assess anxiety and depression, quality of life, and satisfaction with epilepsy care in patients with epilepsy.
Results33 patients completed the sessions and study. Satisfaction with the information improved significantly after the intervention (p < 0.005). The information items with significant improvements were satisfaction with information about epilepsy, treatment, provision of aid and treatment of the impact of epilepsy (p < 0.005) Satisfaction with communication decreased (p < 0.005), being the items with the most changes, the “time to answer the questions” and “consideration with their individual needs”. No significant changes were shown in depression and anxiety, quality of life and satisfaction with the organization.
ConclusionsEmpowerment interventions demonstrated benefits to improve satisfaction with information in patients with epilepsy. The educational intervention designed allows sharing knowledge, solving problems and improving skills, empowering the patient in a new concept of education, which the nurse is a facilitator who collaborates with the demands of the patients. More studies are needed to increase the sample and demonstrate benefits in quality of life and anxiety and depression.
Evaluar la efectividad de una intervención educativa con empoderamiento para pacientes con epilepsia en un hospital español de referencia en epilepsia.
MétodosSe diseñó un ensayo clínico no aleatorizado en un centro de epilepsia. Se llevó a cabo un programa de intervención grupal con empoderamiento en el que se reclutaron voluntarios en consultas externas. Contenía temas comunes en la educación sanitaria en epilepsia, como conocer su enfermedad, los tipos de crisis, el tratamiento, cómo actuar en caso de crisis, los factores precipitantes de crisis, el estilo de vida y el manejo de la medicación, además de adaptarse a las demandas de información de los pacientes. Los pacientes fueron empoderados al aplicar sus conocimientos y habilidades, utilizando a la enfermera como facilitadora. Se administraron cuestionarios antes y después de la intervención para evaluar la ansiedad y la depresión, la calidad de vida y la satisfacción con la atención y los cuidados a los pacientes con epilepsia.
ResultadosCompletaron las sesiones y estudio 33 pacientes. La satisfacción con la información mejoró significativamente después de la intervención (p < 0,005). Los ítems de información con mejoras significativas fueron la satisfacción con la información sobre la epilepsia, el tratamiento, la provisión de ayudas y el tratamiento del impacto de la epilepsia (p < 0,005) La satisfacción con la comunicación disminuyó (p < 0,005), siendo los ítems con más cambios, el “tiempo a responder a las preguntas” y “consideración con sus necesidades individuales”. No se demostraron cambios significativos en la depresión y ansiedad, la calidad de vida y satisfacción con la organización.
ConclusionesLas intervenciones de empoderamiento demostraron beneficios para mejorar la satisfacción con la información en pacientes con epilepsia. La intervención educativa diseñada permite compartir conocimientos, resolver problemas y mejorar habilidades, empoderando al paciente en un nuevo concepto de educación en el que la enfermera es un elemento facilitador que colabora con las demandas de los pacientes. Se precisan más estudios que permitan aumentar la muestra y demostrar beneficios en calidad de vida y ansiedad y depresión.
Epilepsy is a disorder of the brain characterised by an enduring tendency to seizures, and by its neurobiological, cognitive, psychological, and social consequences.1
The impact of epilepsy is multifaceted, and its effects are extensive. Seizures are unpredictable and often dangerous, increasing the risk of injury, hospitalisation, disability, and mortality.2 However, the impact of epilepsy extends beyond the effects of seizures; it correlates strongly with psychiatric comorbidity, such as depression and anxiety, above that of the general population, and this is often neglected in care and treatment.3 Seizures can lead to stigmatisation and social exclusion, and have detrimental effects on an individual's confidence and self-esteem. Therefore, the first goal of treatment is to control seizures, but it should also include the detection and management of comorbidities to improve quality of life.4
Women with epilepsy require more attention: hormonal disturbances caused by seizures and epilepsy can lead to sexual dysfunction, menstrual irregularity, infertility, and premature termination of reproductive status.5 In addition, some antiepileptic drugs may interfere with hormonal contraception, and the teratogenic effects of antiepileptic drugs require vigilance in pregnant women to minimise side effects on the foetus and ensure the safety of mothers.6
Nurse-led interventions have shown good results in patient satisfaction.7 However, therapeutic education in epilepsy must target all personal dimensions, which requires comprehensive, evidence-based, and patient-centred self-management approaches that can be scaled widely in clinical and community settings.8
Empowerment, as an educational tool, is defined as a process in which patients understand their disease and are given the knowledge and skills by their healthcare provider to perform a task in an environment that foments patient participation.9 Four steps in patient empowerment have been described: patient understanding of their role, knowledge acquisition, skills acquired by the patient, and a facilitating environment.10 Other authors, however, have described the dimensions of empowerment as: patient participation in decision-making, patient self-management of the illness, knowledge acquisition, coping skills, engagement, patients' sense of meaning of their experience of the illness, motivation, confidence, self-care, and sharing and enabling others.11 Other authors describe these elements more simply as decision-making, active role in care activities, and partnership.12
Education, in this case, focuses not only on medical aspects, but also on empowering knowledge: biopsychological, functional, experiential, ethical, social, and economic.13
In epilepsy nursing interventions, recent specialisation, and the emergence of advanced practice epilepsy nurses around the world have fomented changes within services, education, and the continued advancement of epilepsy care.14 Epilepsy nurses have reported outcomes in the care of patients with chronic epilepsy, of improved satisfaction, quality of life, and benefiting patient satisfaction.15,16
Empowerment has been used in many nursing education interventions, especially in chronic diseases. Results have been demonstrated in terms of knowledge and self-care,17 and in other personal dimensions, such as resilience and post-traumatic growth levels.18
Empowerment is now seen as an integral component of holistic practice and service design in healthcare, particularly with regard to improvements in the quality of life of people with epilepsy,19 but few empowerment programmes in epilepsy have been published. One study in children with epilepsy and their parents showed improvements in epilepsy knowledge, self-efficacy, and quality of life with empowerment methods,20 and another study using self-care education has also shown benefits.21 Overall, there is a lack of clarity in patient empowerment research studies, which should be conducted operationalising and measuring patient empowerment.22
In epilepsy, there is a need to explore new and well-detailed interventions that focus on patient empowerment and expectations rather than just knowledge acquisition. The challenge is how to implement and develop an intervention programme that engages all the theoretical concepts of empowerment. The key point is how to facilitate a positive environment that motivates patients to acquire skills, confidence, to share experiences, and to empower each other.
Therefore, our aim in this study is to evaluate the effectiveness of an educational empowerment intervention in patients with epilepsy in a Spanish referral hospital for epilepsy.
MethodologyDesignA quasi-experimental non-randomised clinical trial design was used administering a pre- and post-intervention questionnaire. This study was designed following the TREND Statement Checklist (Transparent Reporting of Evaluation with Nonrandomized Designs).23
Study population and scopeThe study was conducted in the Hospital Clinic of Barcelona, a tertiary hospital specialising in epilepsy, and data were collected between June 2019 and June 2020. Therefore, the population will primarily be patients with drug-resistant or difficult-to-control epilepsies. Inclusion criteria were patients with a history of epilepsy of less than 10 years. Exclusion criteria were non-epileptic paroxysmal disorders, psychiatric disorders, and cognitive and/or functional disorders that prevented attendance at the scheduled study sessions. Voluntary study participants were recruited from outpatient epilepsy clinic visits.
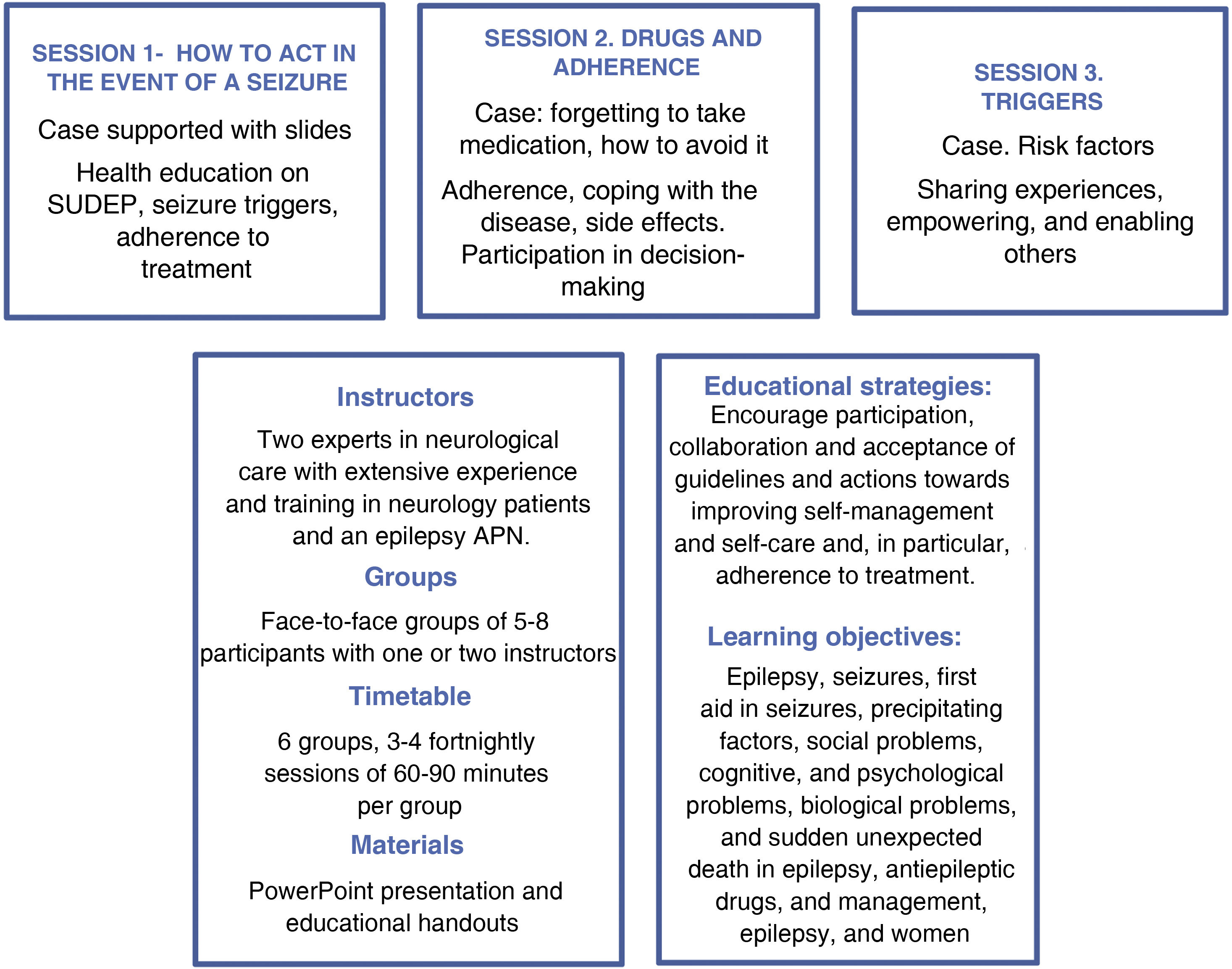
InterventionThe educational intervention is explained in more detail in Fig. 1, according to the guide for reporting educational interventions (GREET checklist).24 The intervention was based on the dimensions of empowerment11: participation in decision-making, gaining control, knowledge acquisition, coping skills, engagement, patients’ sense of meaning of their experience of the illness, motivation, self-care and sharing, confidence, and the development of skills.

The health intervention was designed in collaboration with a psychologist specialising in epilepsy and was conducted by nurses. The programme consisted of 3 health education sessions plus an optional session to address the specific problems of women with epilepsy, thus addressing the gender perspective. In the first session, patients were asked about their expectations of health education to tailor the training to the patients' demands. The 3 sessions were structured around specific topics related to epilepsy: knowledge of the disease, types of seizures, treatment, how to act in the event of a seizure, seizure triggers, lifestyle, and medication management. The dynamics of the sessions involved presenting the topics through pictures and asking a question to encourage participation and empowerment among the patients.
In the sessions, the patients discuss and compare their problems and try to find potential solutions to manage their illness. The education focuses on patients' priorities and fears, and information on their expectations and demands.25
VariablesThe demographic variables of the study subjects were age and sex. The clinical variables were age at onset of epilepsy, number of seizures (annual, monthly, weekly, or daily) and number of antiepileptic drugs were recorded.
The primary dependent variable was satisfaction with epilepsy care. Secondary dependent variables were quality of life, anxiety, and depression.
Instruments: the data were collected using an online questionnaire via the LimeSurvey survey, which included an ad hoc questionnaire and the following validated questionnaires:
- •
Quality of life in epilepsy inventory (QOLIE-31): a validated questionnaire widely used in epilepsy research.26 Its 31 questions assess, scoring from 0 to 100, 2 dimensions: the emotional and psychological effects of seizures (seizure worry, overall quality of life, emotional well-being, and energy/fatigue) and medical and social effects (medication effects, work-driving-social limits, and cognitive functioning effects).
- •
Satisfaction with epilepsy care questionnaire (SEC-E), originally in German15 and recently validated in Spanish27 which measures satisfaction with organisation (7 items), communication (4 items) and information received (12 items) in epilepsy care. It assesses satisfaction on a Likert scale, ranging from very dissatisfied (0 points) to very satisfied (5 points), with an average for each subscale.
- •
Hospital Anxiety and Depression Scale (HADS): validated and useful in neurology,28 comprising 2 subscales: Depression and Anxiety, each with 7 items scored between 0 and 21 (each item is scored between 0 and 3. The higher the score, the greater the severity of the symptoms.
Patients with epilepsy visiting outpatient clinics were informed about the study and invited to participate. Data were collected using the LimeSurvey platform, which ensures data confidentiality. Signed informed consent was obtained before the start of the study. The respondents were sent pre-intervention questionnaires and completed a questionnaire 2 weeks after the end of the last programme session.
Statistical analysisData are presented as means and standard deviation for continuous variables and as numbers and percentages (%) for categorical variables. Quantitative variables were compared using the t-test for independent samples. The χ2 test was used to compare categorical variables. Radar plots were used to visualise differences before and after the intervention. All significance tests were 2-tailed and p-values of <.05 were considered significant. All analyses were performed using R version 3.6.3 for Windows statistical software.
Ethical considerationsThe local Institutional Review Board Ethics Committee, HCB/2017/0008, approved the study. Patients were given information about the study, were asked to participate, and signed their informed consent.
The present study was conducted in accordance with the Declaration of Helsinki and complied with the protocol and legal requirements as per the Biomedical Research Act14/2007.
ResultsSeven group sessions were conducted with 54 participants, of whom 10 (18.5%) did not complete the sessions, 9 (16.7%) did not complete the questionnaires, and 2 were excluded due to psychiatric disorders. An eighth group with 8 patients had to be discontinued due to the COVID-19 pandemic. Therefore, 33 participants were analysed.
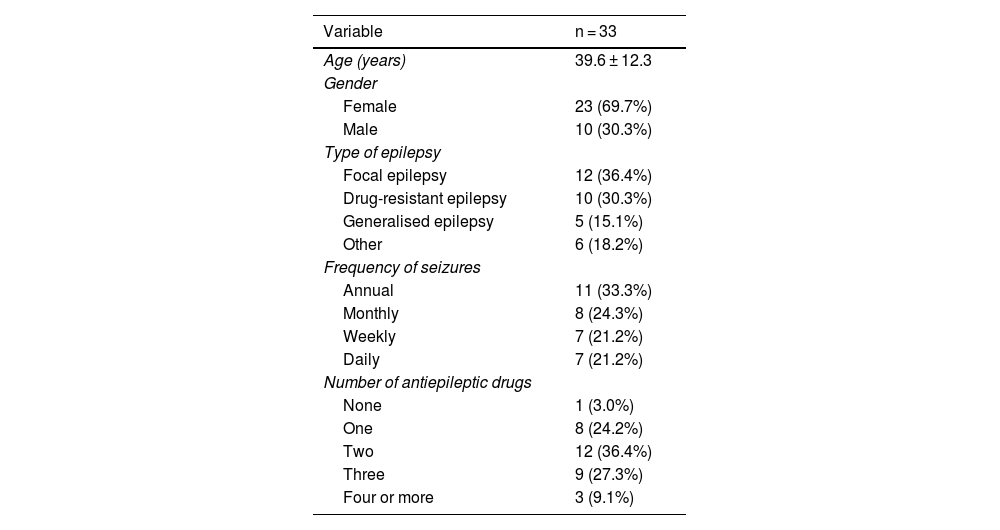
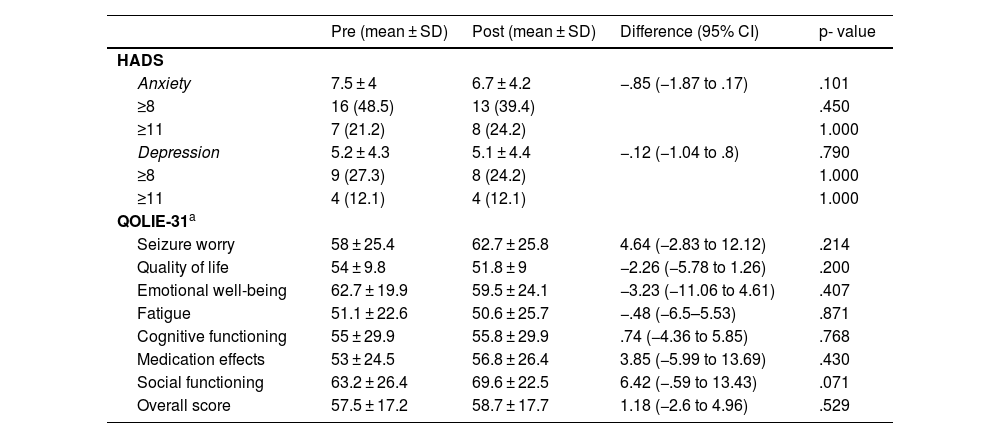
The characteristics of the patients are shown in Table 1. The mean age was 39.6 years and 69.7% were female. The type of epilepsy was predominantly focal (36.4%) or drug-resistant (30.3%). Seizure frequency varied widely, and most of the participants were on between one and three drugs. Table 2 shows the results of the pre- and post-intervention scales on quality of life and anxiety and depression. The respondents' quality of life showed no significant changes after the intervention. Only the dimension of social relationships showed a non-significant trend towards improvement. There were no significant changes in anxiety or depression.
Sociodemographic and clinical variables.
| Variable | n = 33 |
|---|---|
| Age (years) | 39.6 ± 12.3 |
| Gender | |
| Female | 23 (69.7%) |
| Male | 10 (30.3%) |
| Type of epilepsy | |
| Focal epilepsy | 12 (36.4%) |
| Drug-resistant epilepsy | 10 (30.3%) |
| Generalised epilepsy | 5 (15.1%) |
| Other | 6 (18.2%) |
| Frequency of seizures | |
| Annual | 11 (33.3%) |
| Monthly | 8 (24.3%) |
| Weekly | 7 (21.2%) |
| Daily | 7 (21.2%) |
| Number of antiepileptic drugs | |
| None | 1 (3.0%) |
| One | 8 (24.2%) |
| Two | 12 (36.4%) |
| Three | 9 (27.3%) |
| Four or more | 3 (9.1%) |
Anxiety, depression, and quality of life before and after the intervention.
| Pre (mean ± SD) | Post (mean ± SD) | Difference (95% CI) | p- value | |
|---|---|---|---|---|
| HADS | ||||
| Anxiety | 7.5 ± 4 | 6.7 ± 4.2 | −.85 (−1.87 to .17) | .101 |
| ≥8 | 16 (48.5) | 13 (39.4) | .450 | |
| ≥11 | 7 (21.2) | 8 (24.2) | 1.000 | |
| Depression | 5.2 ± 4.3 | 5.1 ± 4.4 | −.12 (−1.04 to .8) | .790 |
| ≥8 | 9 (27.3) | 8 (24.2) | 1.000 | |
| ≥11 | 4 (12.1) | 4 (12.1) | 1.000 | |
| QOLIE-31a | ||||
| Seizure worry | 58 ± 25.4 | 62.7 ± 25.8 | 4.64 (−2.83 to 12.12) | .214 |
| Quality of life | 54 ± 9.8 | 51.8 ± 9 | −2.26 (−5.78 to 1.26) | .200 |
| Emotional well-being | 62.7 ± 19.9 | 59.5 ± 24.1 | −3.23 (−11.06 to 4.61) | .407 |
| Fatigue | 51.1 ± 22.6 | 50.6 ± 25.7 | −.48 (−6.5–5.53) | .871 |
| Cognitive functioning | 55 ± 29.9 | 55.8 ± 29.9 | .74 (−4.36 to 5.85) | .768 |
| Medication effects | 53 ± 24.5 | 56.8 ± 26.4 | 3.85 (−5.99 to 13.69) | .430 |
| Social functioning | 63.2 ± 26.4 | 69.6 ± 22.5 | 6.42 (−.59 to 13.43) | .071 |
| Overall score | 57.5 ± 17.2 | 58.7 ± 17.7 | 1.18 (−2.6 to 4.96) | .529 |
CI: confidence interval; SD: standard deviation.
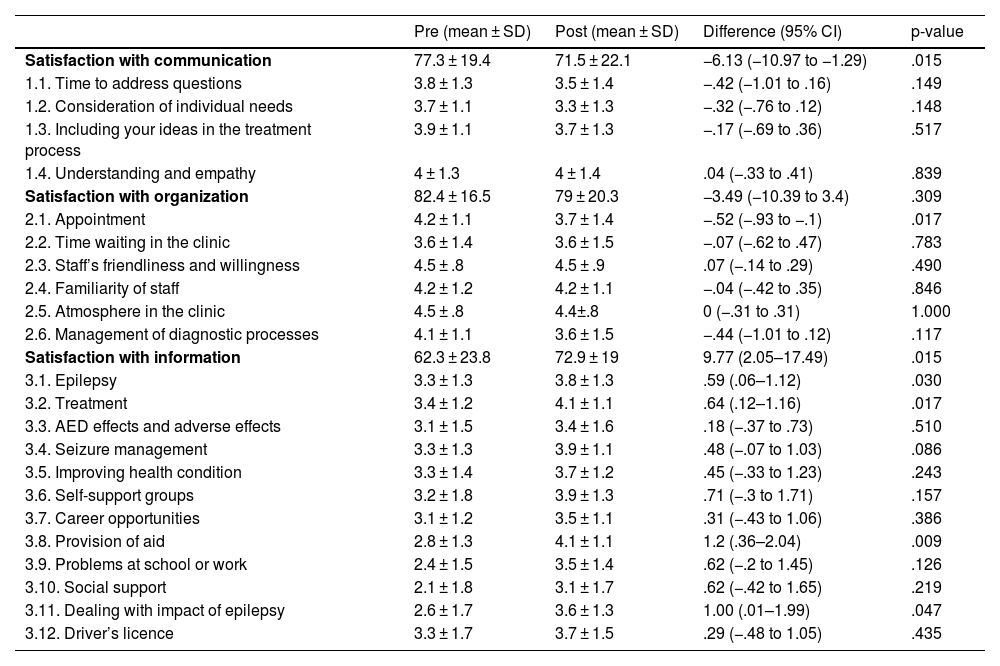
The changes in satisfaction can be seen in Table 3. The SEC-E showed some changes after the intervention: the dimension of satisfaction with the organisation showed no significant changes.
Satisfaction with epilepsy care questionnaire (SEC-E) before and after the intervention.
| Pre (mean ± SD) | Post (mean ± SD) | Difference (95% CI) | p-value | |
|---|---|---|---|---|
| Satisfaction with communication | 77.3 ± 19.4 | 71.5 ± 22.1 | −6.13 (−10.97 to −1.29) | .015 |
| 1.1. Time to address questions | 3.8 ± 1.3 | 3.5 ± 1.4 | −.42 (−1.01 to .16) | .149 |
| 1.2. Consideration of individual needs | 3.7 ± 1.1 | 3.3 ± 1.3 | −.32 (−.76 to .12) | .148 |
| 1.3. Including your ideas in the treatment process | 3.9 ± 1.1 | 3.7 ± 1.3 | −.17 (−.69 to .36) | .517 |
| 1.4. Understanding and empathy | 4 ± 1.3 | 4 ± 1.4 | .04 (−.33 to .41) | .839 |
| Satisfaction with organization | 82.4 ± 16.5 | 79 ± 20.3 | −3.49 (−10.39 to 3.4) | .309 |
| 2.1. Appointment | 4.2 ± 1.1 | 3.7 ± 1.4 | −.52 (−.93 to −.1) | .017 |
| 2.2. Time waiting in the clinic | 3.6 ± 1.4 | 3.6 ± 1.5 | −.07 (−.62 to .47) | .783 |
| 2.3. Staff’s friendliness and willingness | 4.5 ± .8 | 4.5 ± .9 | .07 (−.14 to .29) | .490 |
| 2.4. Familiarity of staff | 4.2 ± 1.2 | 4.2 ± 1.1 | −.04 (−.42 to .35) | .846 |
| 2.5. Atmosphere in the clinic | 4.5 ± .8 | 4.4±.8 | 0 (−.31 to .31) | 1.000 |
| 2.6. Management of diagnostic processes | 4.1 ± 1.1 | 3.6 ± 1.5 | −.44 (−1.01 to .12) | .117 |
| Satisfaction with information | 62.3 ± 23.8 | 72.9 ± 19 | 9.77 (2.05–17.49) | .015 |
| 3.1. Epilepsy | 3.3 ± 1.3 | 3.8 ± 1.3 | .59 (.06–1.12) | .030 |
| 3.2. Treatment | 3.4 ± 1.2 | 4.1 ± 1.1 | .64 (.12–1.16) | .017 |
| 3.3. AED effects and adverse effects | 3.1 ± 1.5 | 3.4 ± 1.6 | .18 (−.37 to .73) | .510 |
| 3.4. Seizure management | 3.3 ± 1.3 | 3.9 ± 1.1 | .48 (−.07 to 1.03) | .086 |
| 3.5. Improving health condition | 3.3 ± 1.4 | 3.7 ± 1.2 | .45 (−.33 to 1.23) | .243 |
| 3.6. Self-support groups | 3.2 ± 1.8 | 3.9 ± 1.3 | .71 (−.3 to 1.71) | .157 |
| 3.7. Career opportunities | 3.1 ± 1.2 | 3.5 ± 1.1 | .31 (−.43 to 1.06) | .386 |
| 3.8. Provision of aid | 2.8 ± 1.3 | 4.1 ± 1.1 | 1.2 (.36–2.04) | .009 |
| 3.9. Problems at school or work | 2.4 ± 1.5 | 3.5 ± 1.4 | .62 (−.2 to 1.45) | .126 |
| 3.10. Social support | 2.1 ± 1.8 | 3.1 ± 1.7 | .62 (−.42 to 1.65) | .219 |
| 3.11. Dealing with impact of epilepsy | 2.6 ± 1.7 | 3.6 ± 1.3 | 1.00 (.01–1.99) | .047 |
| 3.12. Driver’s licence | 3.3 ± 1.7 | 3.7 ± 1.5 | .29 (−.48 to 1.05) | .435 |
CI: confidence interval; SD: standard deviation.
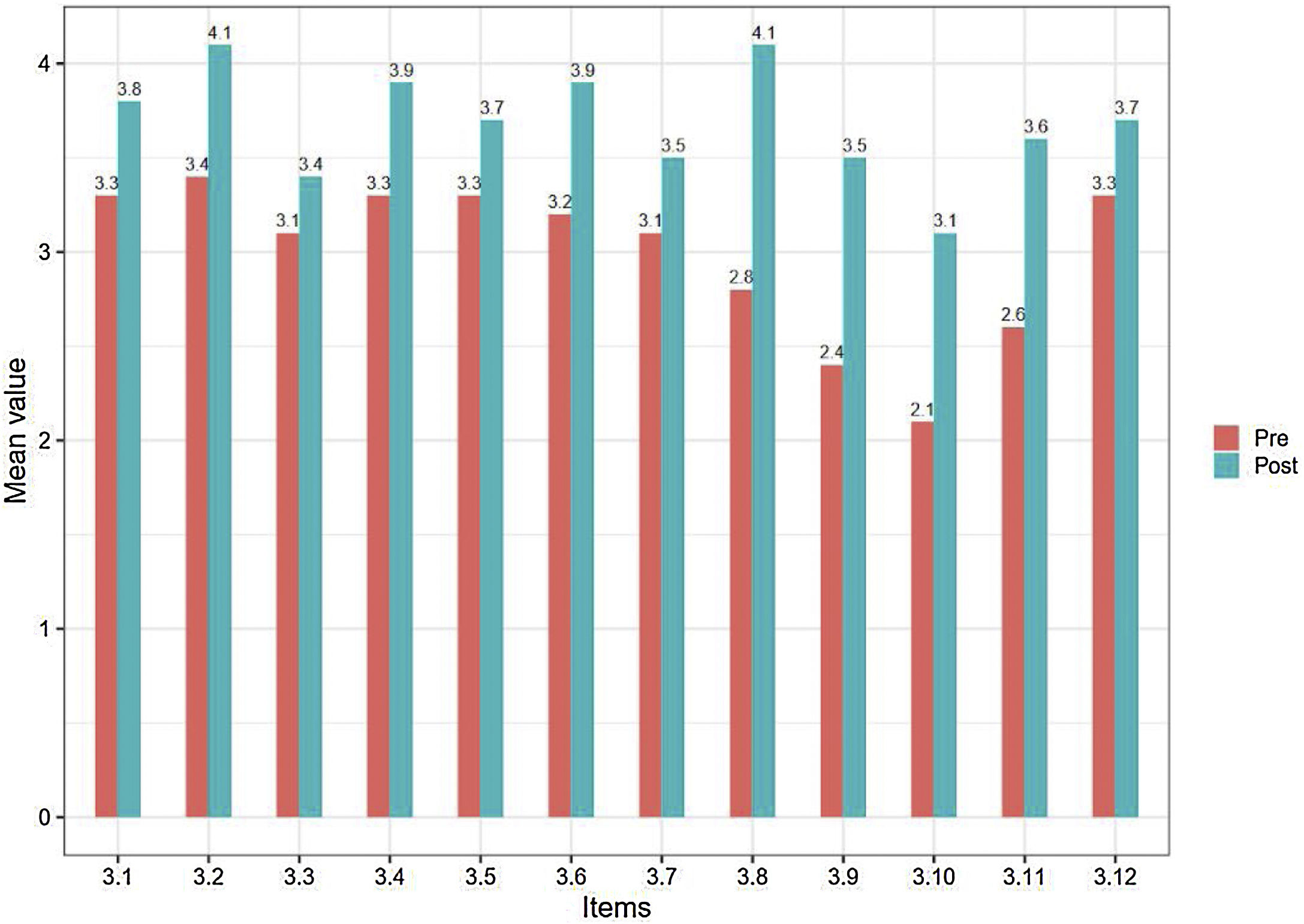
Satisfaction with communication decreased (p < .005), and the items with the most changes were ‘time to address questions’ and ‘consideration of individual needs’. Satisfaction with information showed a significant improvement (p < .005), as we can also see in Fig. 2. The information items with significant improvements were satisfaction with information about epilepsy, treatment, provision of aid, and dealing with the impact of epilepsy (p < .005). Seizure management, self-support groups, and problems at school or work showed an improving trend.
Discussion.")
Although studies have demonstrated the effectiveness of health education for patients with epilepsy, holistic practice and service design components in healthcare must be advanced using patient-centred interventions.
International organisations such as the International League Against Epilepsy (ILAE)29 and the International Bureau for Epilepsy (IBE)30 disseminate knowledge and promote education, research, and the empowerment of people with epilepsy. However, there are no international guidelines available to improve the quality of patient education interventions or empower people with epilepsy.
Reports indicate that empowerment is an ambiguous concept that is poorly understood by service users and care providers alike. Conceptual ambiguity is a further impediment to its understanding and implementation.19 Empowerment is often used as a theoretical model, with no specific detail as to how to promote or achieve it, indicating that a new approach to empowerment interventions using new tools is required.
We design and deliver specific empowerment education, in which people empower themselves and others. Patients, in small groups, apply their knowledge and skills to problem solving, using nurses as facilitators who support their skills rather than merely performing a didactic role.31
The intervention was evaluated in a prospective, non-randomised study. Outcomes and measurements focused on patients' perceptions of benefits (satisfaction, quality of life, anxiety and depression).
Our results showed the benefits of an empowerment intervention in improving satisfaction with the information received, which has also been shown in other studies without empowerment.15 Many educational interventions, especially group interventions, can benefit from or use empowerment skills, without being designed for this purpose.
We found an association between a specific empowerment intervention and satisfaction when assessing specific epilepsy goals, such as disease, treatment, seizure management, provision of aid, and managing the impact of epilepsy. Previous studies have shown that patients with epilepsy failed to get the information they wanted from their care team,32 but the model and the way the intervention was conducted in our study was based on addressing their expectations; they do not only want knowledge, but also to share their experiences with other patients and professionals, and manage their disease better.25
Satisfaction with the organisational dimension remained unchanged after the intervention, as in another educational intervention study,15 which shows that this dimension of the tool is better for other organisational changes or interventions.
In the case of communication, even though the methodology involved and was focused on it, we found satisfaction with it decreased. In our case, these results could be explained by the design of the original scale, as the questions focus on communication in epilepsy outpatient clinics.15 It could also be interpreted as empowerment resulting in a more critical perception of the system. Another study using this scale found no improvement, although there was no reduction in satisfaction in this respect.15
Our intervention did not show beneficial effects on quality of life or on anxiety and depression, as was found in other similar interventions.15 The complexity of disorders such as depression and anxiety in patients with epilepsy and their relationship with other health outcomes such as quality of life is influenced by other psychological determinants such as self-compassion or resilience,33 which probably require more specific multidisciplinary interventions to achieve these goals.
Our limitations for patient inclusion and loss to follow-up of the sample also reveal the difficulties for people with epilepsy to participate in educational groups. This may be due to psychological barriers and distress that interfere with health behaviours,34 and stigma and patient perception of the disease resulting in problems with social integration.35
Educational and supportive interventions are therefore needed to counteract perceived stigma,36 as well as interventions with larger samples and that follow these lines of empowerment.
LimitationsAlthough the gender perspective is addressed in the intervention, there is no specific measure on this.
Low voluntary participation and the COVID-19 pandemic that interrupted the study limited the sample size, and therefore interpretation of the results must be limited to the present study.
ConclusionsOur results confirm the usefulness of the empowerment intervention to increase satisfaction with information for patients with epilepsy.
This intervention enables knowledge sharing, problem solving, and skills improvement, empowering the patient in a new concept of nurse-led education, in which nurses are facilitators collaborating with patients' demands.
It would be good to complement empowerment interventions with a multidisciplinary approach to depression and anxiety, addressing aspects such as self-compassion and resilience.
The benefits of group interventions, with the limitations imposed by the pandemic, show the need to explore new technologies and adapt online educational and empowerment interventions to maximise empowerment and interaction between patients, minimising limitations and barriers.
FundingSpanish society of Neurological Nursing (SEDENE) - UCB-Patient Value-2017. Hospital Clínic Pedrera Intensification Grant 2018. Peris Grant 2019–2020.
Conflict of interestThe authors have no conflict of interest to declare.
To Carol Aguilera and Francina Salord for their collaboration in the sessions.