






Ankle fractures are one of the main causes of consultation with emergency services around the world, with an incidence of 187 / 100,000 inhabitants per year. The most common is type B in the Weber-Dannis classification, with a long-term evolution towards osteoarthritis of 14%. Although the diagnosis of distal fibular fracture on an ankle radiograph is very simple, its usefulness has probably been overestimated to provide the necessary insights to decide the appropriate treatment method for the fracture. The objective of the study is to evaluate the diagnostic utility of ankle radiographs and their inter-observer agreement for a treatment decision making in Weber B fractures.
MethodsA prospective, randomized, double-blind, multicenter trial using three-country surveys of orthopedic surgeons was conducted; orthopedic surgeons and foot and ankle surgeons, were exposed to four Weber B ankle fractures x-ray series where surgery was actually required as the only treatment option. Unilateral and comparative projections, where presented in different time and order to each surgeon, measuring the variability of surgical decisions.
ResultsFifty-one orthopedic surgeons (72.37%), 24 foot and ankle surgeons (15.79%), 4 surgeons of other orthopedic subspecialties (2.63%) and 14 orthopedic surgery residents (9.21%) were surveyed. An inter-observer agreement of 70.83% (p <0.05) was found in the comparative projections series and 55.31% (p <0.05) in the unilateral ones. When performing linear regression between the training degree, years of experience and the provenance country of the surgeons, no causality was found (power of β <95%). Nevertheless, 100% of the respondents diagnosed the fracture of the distal fibula as a Weber B fracture.
DiscussionThe unilateral and comparative radiographic series are not recommended for making an adequate surgical decision in Weber B ankle fractures, given their very low inter-observer agreement. For decision making in Weber B ankle fractures it is necessary to take other complementary examinations such as Computed Axial Tomography.
Evidence LevelII
Las fracturas de tobillo constituyen una de las principales causas de consulta a los servicios de urgencias alrededor del mundo, con una incidencia de 187/100.000 habitantes año. La más frecuente es la tipo B en la clasificación de Weber, con una evolución hacia la artrosis a largo plazo del 14%. Aunque el diagnostico de la fractura del peroné distal en una radiografía de tobillo es muy sencillo, probablemente se ha sobrestimado su utilidad para proporcionar elementos de juicio necesarios para decidir el método de tratamiento adecuado para la fractura. El objetivo del estudio es evaluar la utilidad diagnóstica de las radiografías de tobillo y su concordancia interobservador para la toma de decisiones de tratamiento en fracturas de tobillo Weber B.
Materiales y MétodosSe realizó un experimento, prospectivo, aleatorizado, doble ciego, multicéntrico, mediante la aplicación de encuestas en tres países a Ortopedistas, residentes de ortopedia y Cirujanos de pie y Tobillo, en las cuales se les presentaban cuatro casos de fracturas de tobillo Webber B de características quirúrgicas en proyecciones unilaterales y comparativas, midiendo la variabilidad de las decisiones quirúrgicas.
ResultadosSe recolectaron 152 encuestas que respondieron 110 ortopedistas (72.37%), 24 cirujanos de pie y tobillo (15.79%), 4 cirujanos de otras subespecialidades ortopédicas (2.63%) y 14 residentes de ortopedia (9.21%). Se encontró una concordancia interobservador en las proyecciones comparativas del 70.83% (p<0.05) y en las unilaterales del 55.31%, (p<0.05), al realizar regresión lineal entre la respuesta el grado de entrenamiento, los años de experiencia y el país de procedencia no se encontró causalidad (poder de ?? <95%). El 100% de los encuestados diagnosticó la fractura del peroné distal.
DiscusiónLa serie radiográfica unilateral y comparativa no se recomiendan para la toma de una adecuada decisión quirúrgica en las fracturas de tobillo Weber B, dada su muy baja concordancia inter-observador. Para la toma de decisiones en fracturas de tobillo Weber B es necesaria la toma de otros exámenes complementarios como la Tomografía axial Computarizada.
Nivel de EvidenciaII
Injuries to the ankle joint cause about 5 million visits to emergency services in the United States causing an expense of $ 3 million per year, with an incidence of 187 / per 100,000 inhabitants per year. These fractures correspond to 9% of all fractures and about 30% of all foot and ankle injuries.1 In Colombia, Weber B ankle fractures interchangeably affect men and women with an incidence of 120/100,000 inhabitants per year. Its main cause is fall of one's feet in association with a partial lack of unconscious proprioceptive sensations, with a prevalence of 67% among all fractures related to ankle trauma.2,3
Among the ankle fractures the most frequent is a fracture dislocation pattern classified as Danis-Weber type B, which in turn corresponds to the Supination-Eversion and Prone-Abduction fracture in the Lauge-Hansen classification (classification according to trauma mechanism), and also to nine different types of patterns in the AO Classification (classification according to the exact fracture pattern).
The Danis-Weber classification, better known only as Weber, was introduced by Danis in 1949 and modified by Weber in 1972. The simplicity of the original Danis-Weber classification has made it very popular among orthopedic surgeons. However, its main disadvantage is that it does not take into account any injury of the medial structures. There are three types of lateral Weber injuries: A (fracture distal to the syndemosis), B (at syndesmosis level) and C (proximal to syndesmosis). Type A are fibular fractures distal to syndesmosis, that are produced by inversion moment forces, in which mechanisms of adduction and varus (Lauge-Hansen) are combined. The injuries occurs in an outside- in sequence pattern. Type B are injuries at syndemosis level that are produced by forced eversion moment at the heel, in which mechanisms of abduction and valgus (Lauge-Hansen) are combined. The appearance of the injuries varies according to the position of the foot. If the foot is supinated, the injury will start on the outer side and ending on the inner side of the ankle. If the foot is in pronation, the injury will start on the inner side and progress towards the outer side. Type C are fibular fractures proximal to the syndesmosis that are produced by forces that act in eversion (mostly abduction), but with a predominance of abduction vectors that increase the severity of injuries and instability (Lauge-Hansen). Type C are bifocal fractures with rupture of the anterior inferior tibioperoneal ligament or the anterior and posterior ligament. The fracture of the fibula is proximal to the syndesmosis and the medial injuries may involve both the medial ligament or the medial malleolus.4 The biggest drawback with the Weber classification is that in a single group (Weber B) at least two different trauma mechanisms were included (Lauge-Hansen Supination-Eversion and Pronation-Abduction), so when the surgeon has to make a treatment decision will behave as pilot landing in a multiple landing track airport not knowing the code of several landing tracks. For the pilot all landing tracks look similar from the air, as for the surgeon all Weber B fractures looks too.
Ankle fractures correspond to intra-articular fractures. Usually, these fractures are accompanied by loss of articular congruence, secondary or not to the presence of a capsule and ligaments injuries.5 With exception of the ankle, almost all other articular injuries require additional imaging tests to X-rays (Computed Tomography (CT) or Magnetic Resonance imaging (MRI)). The determination of the intra-articular step and gap in an intra-articular ankle fracture has an additional component: the rotation of the fibula, which behaves biomechanically as an intra-articular step (impossible to measure in conventional series of trauma radiographs of the ankle, even using comparative measurements of the healthy contralateral ankle). However, most orthopedic surgeons and even some foot and ankle surgeons a priori misjudge the Weber B ankle fracture as a relatively innocent fracture. This misjudge tend to induce an error and bias the treatment decision the has to be made. Nevertheless, it could be stated that the probability of diagnostic error of the fracture of the distal fibula is practically 0%. The problem is that a Weber B ankle fracture is not the same as an isolated extra-articular fracture of the distal fibula and therefore the diagnostic element of screening (radiological series of trauma) must be differentiated from the different elements of judgment that should be taken into account to establish the appropriate treatment in each particular case. The ease with which the diagnosis of the fracture of the distal fibula is made does not necessarily mean that it is an easy to treat fracture that could be successfully assessed with just a simple or comparative radiological trauma series of the ankle because the rotation of the distal fibula, the shortening of it, and associated soft tissue injuries needs to be assessed with axial images of the ankle mortise. Since the ankle is considered as a complex articular system of kinetic energy transfer, the slightest variation in its anatomical configuration will generate an increase in load that in the long term will inevitably end up producing an ankle osteoarthritis. This is why we increasingly see patients with ankle fractures managed both surgically and non-surgically, 30 or 40 years ago, developing ankle osteoarthritis.
With the increase in population survival around the world, it has become clear that 14% of Weber B ankle fractures evolve towards osteoarthritis. However, this number has been growing in recent years. Three situations mean that the orthopedist does not recognize this problem in his own experience: first, the development of an ankle osteoarthritis exceeds in most cases the professional life of the Orthopedist (because the ankle is a Kinetic energy transfer system, osteoarthritis develops in a very long time); second, the high increase in the average world population life, which in the last 50 years has practically doubled that observed in the immediately previous period of 2,000 years (There is a very high probability that the patient to whom I placed the cast 10 years ago survives 30 more years to develop osteoarthritis of his ankle)6; and third, apparently and without any explanation in the scientific literature, this fracture has been considered as an extra-articular fracture, although clearly the stroke of the fracture in the fibula involves the ankle joint and therefore is an intra-articular fracture. Despite the complexity and wide variability of Weber B fractures, their evaluation and the way in which decisions about their management were made remains as at the beginning of time, when conventional radiology was invented. There are no studies regarding the positive and negative predictive values of the conventional radiological technique of one limb or comparative with the other limb. Despite having many duly standardized measurements for the radiological technique, sometimes the orthopedist does not perform them rigorously, or does not perform the comparison with the contralateral limb, usually normal.
There is no discussion about the diagnostic value of the ankle x-ray as a screening to determine the fracture of the distal fibula, or the inference that is made on the fracture pattern, in this case: Weber B.
Regardless of the population's lifetime, the inadequate anatomical reduction of Weber B ankle fractures is the cause of 14% of these lesions progressing to post-traumatic ankle osteoarthritis, with clinical and functional results, at least as bad as osteoarthritis of the hip and knee.
The objective of the study is to evaluate the diagnostic utility of ankle radiographs and their inter-observer concordance for surgical decision making in Weber B ankle fractures.
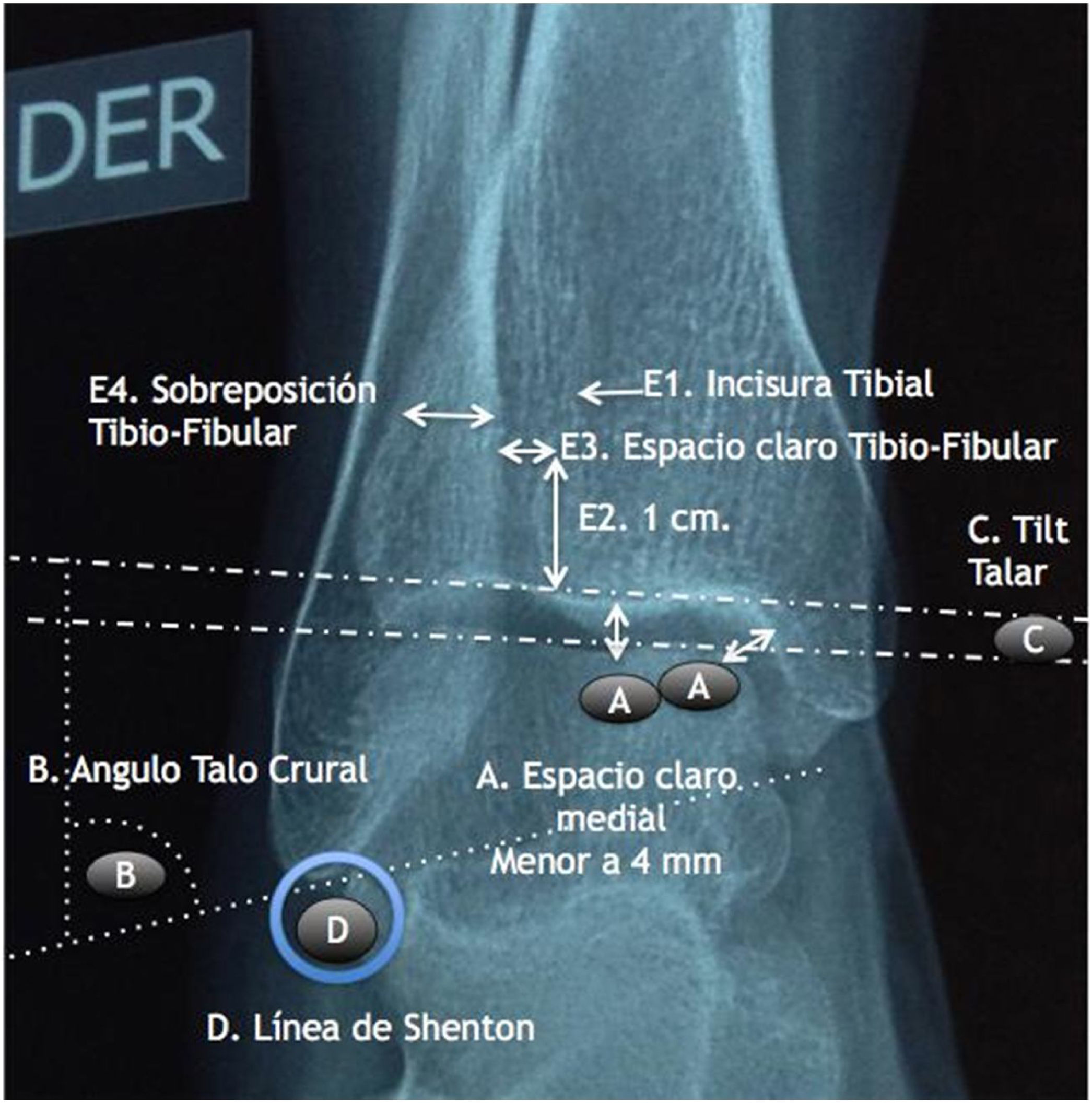
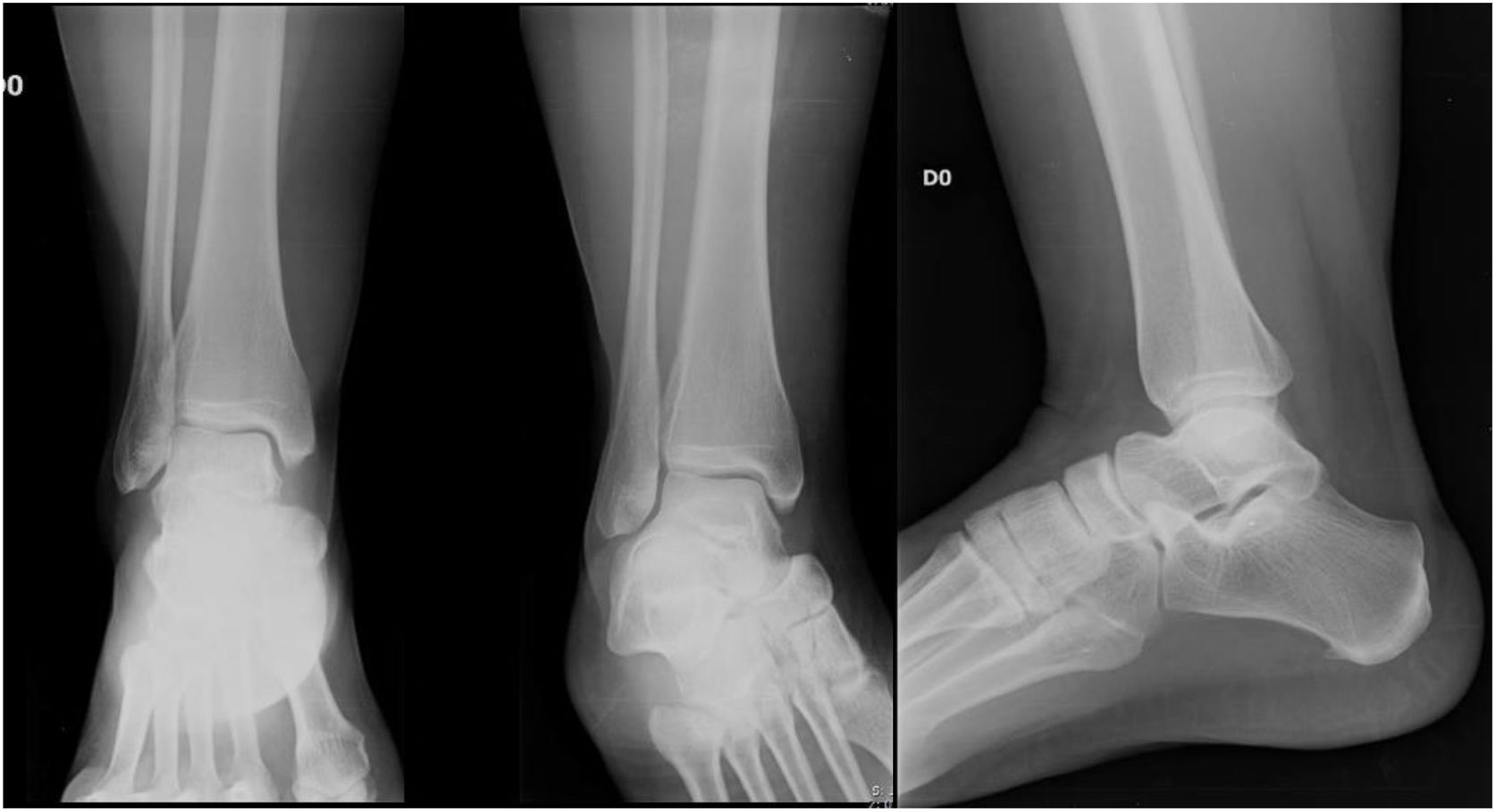
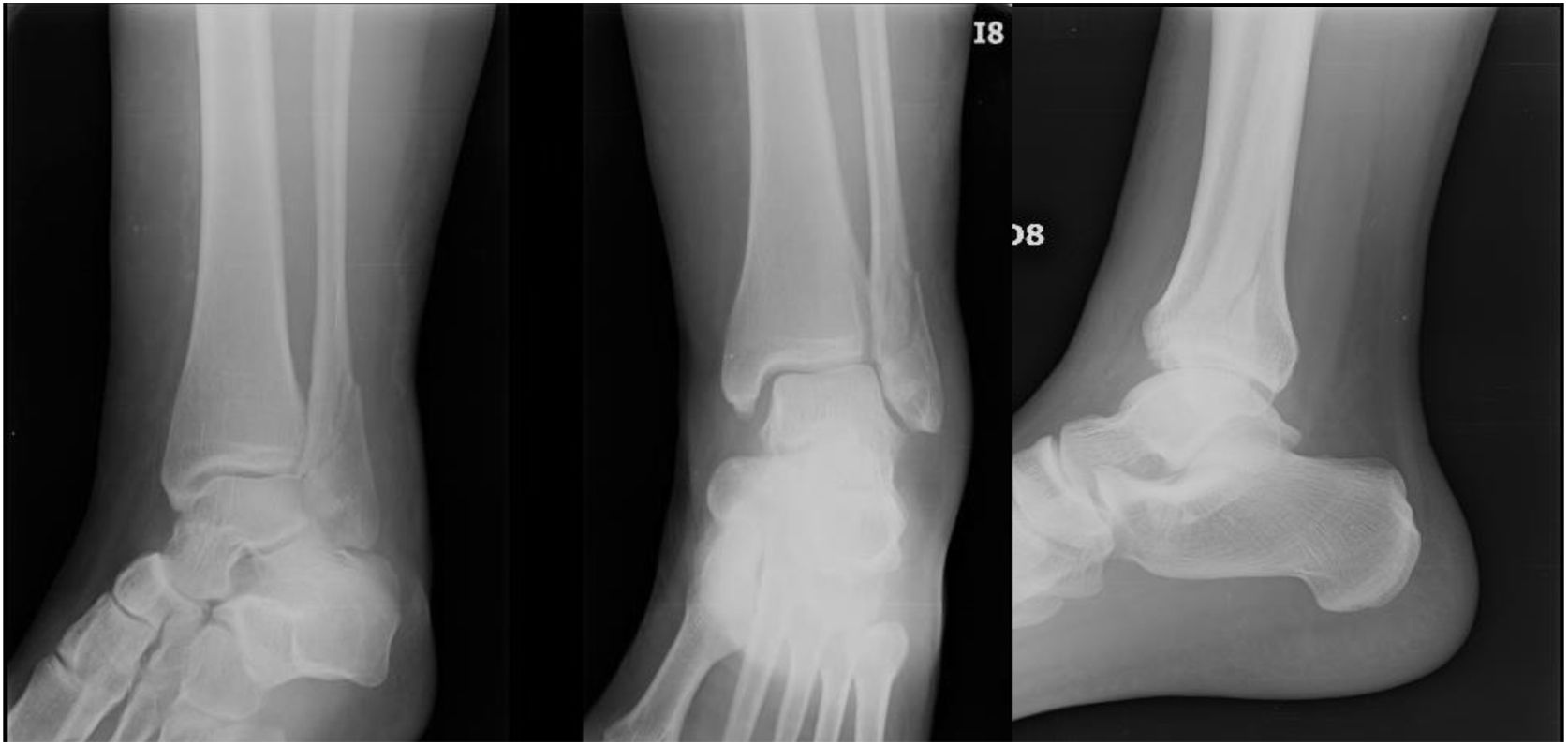
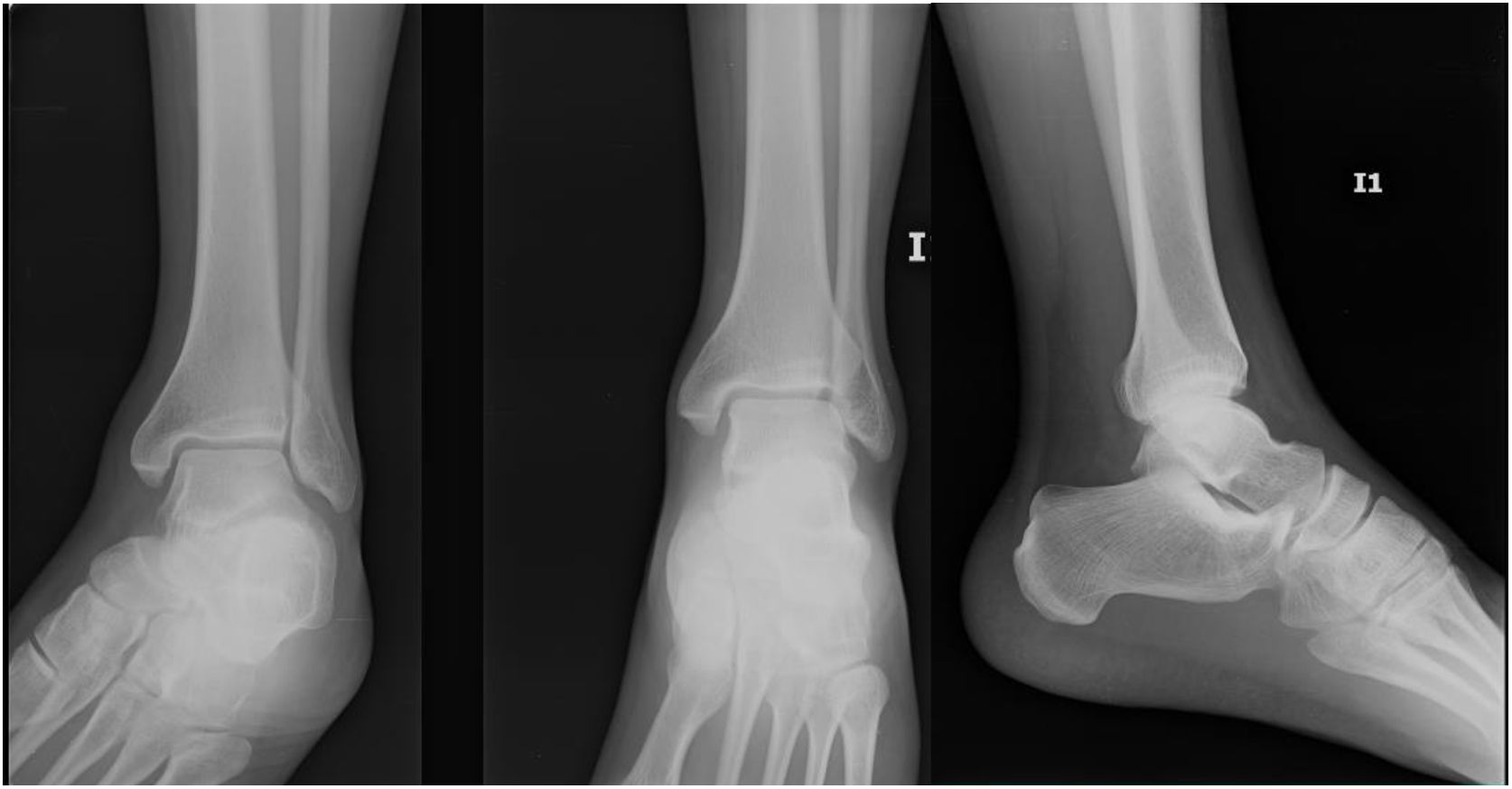
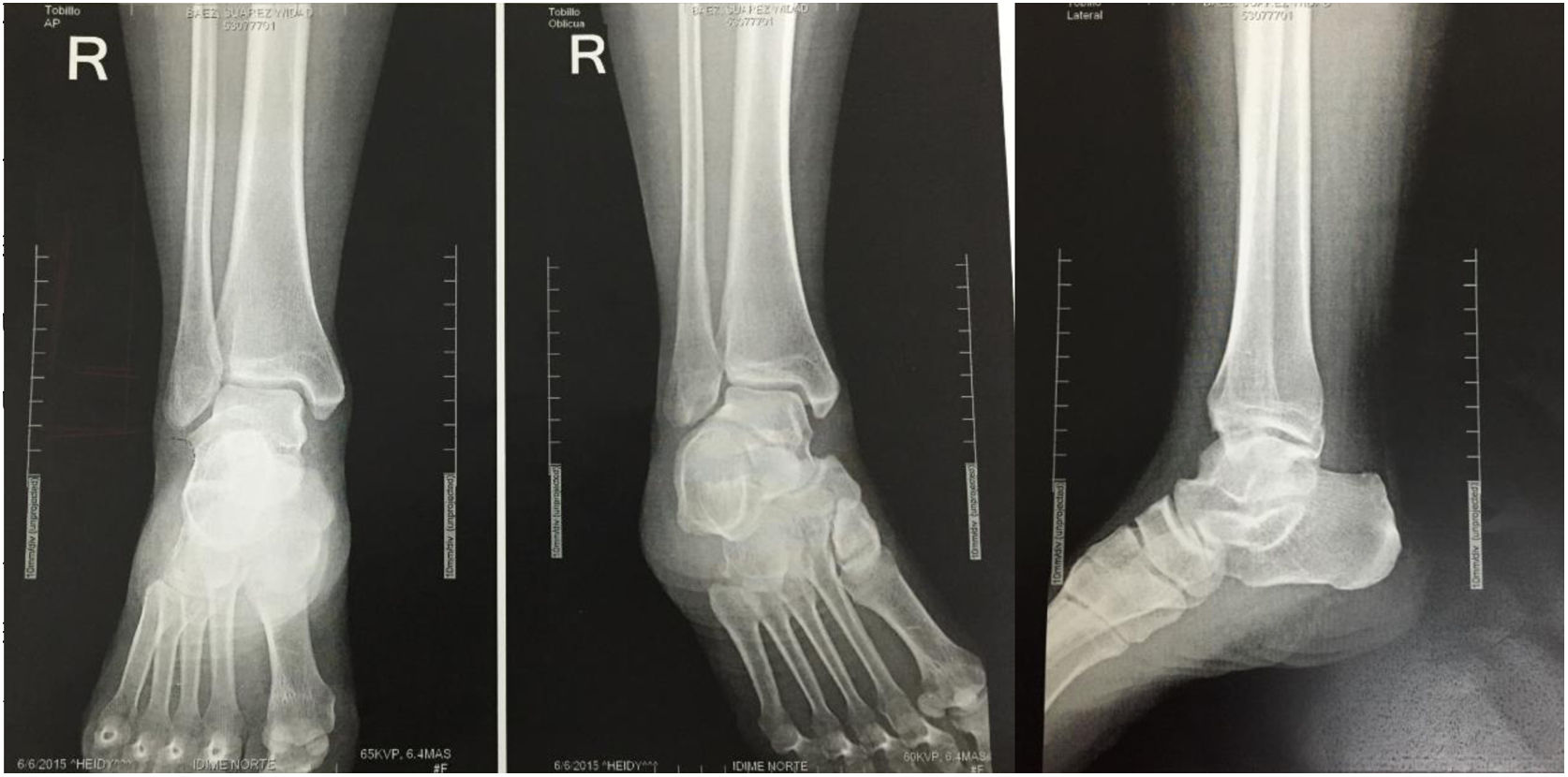
Materials and methodsA self-controlled, randomized, double-blind, multi-centric assay was carried out by applying surveys in three different countries to general orthopedists, foot and ankle surgeons and orthopedic surgery residents. The criteria of simple randomization was established through the presence of respondents in the foot and ankle symposiums in the city of Guayaquil in the framework of the Ecuadorian Congress of Orthopedics and Traumatology, In the city of Cali in the framework of the national foot course and Ankle of the Colombian Society of Orthopedics and Traumatology and in the city of Cancun within the framework of the Mexican Congress of Orthopedics and Traumatology of the FEMECOT, establishing as an inclusion criterion to be able to evaluate clinical cases and conduct the survey regardless of their degree of training or years of experience. Four cases of Webber B ankle fractures of surgical characteristics were delivered due to their radiological measurements with outcomes known by Senior authors (Eduardo Reina, Juan Manuel Herrera, Carlos Ramirez, Bosco Mendoza and Victor Toledo) as shown in Figure 1.
; 61-78.).")
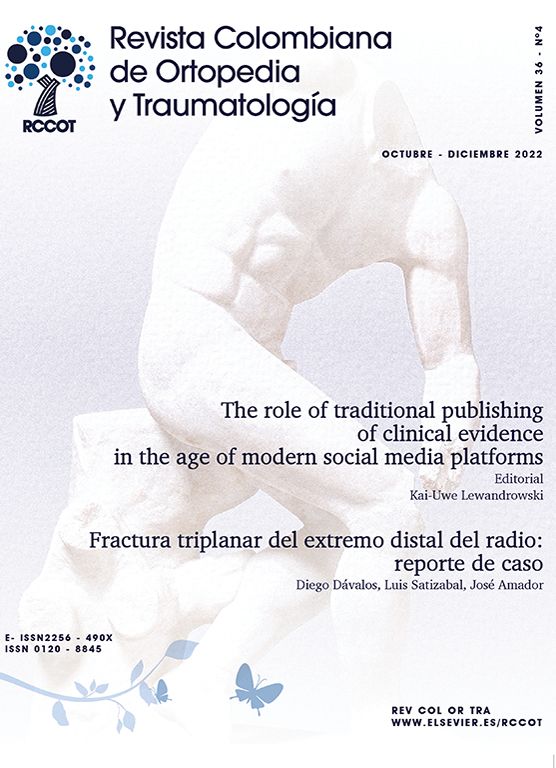
In case number one, the difference between the talocrural angle of 6° and the shenton line with a incongruity of 3mm on the fractured side was established as surgical criteria Figures 2 and 3.


In case number two, the medial clear space increased by 5mm and the difference of 5 degrees of the talocrural angle was established as a surgical criterion as observed in Figures 4 and 5.


In case number three, 1mm of discrepancy of the shenton line and an opening of the medial clear space of 6mm were established as a surgical criterion, in addition to a fibular apparent rotation and discrepancy of the talocrural angle, as observed in Figures 6 and 7.


In case number four, the surgical criterion established the difference of 9 degrees in the talocrural angle with the comparative radiography and the medial clear space increased by 1mm. Figures 8 and 9


At different times, each study participant was given a series with the four cases, all evaluated by means of a series of unilateral trauma and again at different time the same four cases with the radiological measurements explicitly written and duly made with comparison of the contralateral side was also provided. The order of the series was unchanged and subjects were not informed that they were evaluating the same four series.
We named the unilateral radiographic without radiological measurements as the study group, and the comparative radiographic series with explicit measurements of the same 4 cases of fractures as the self-control group. The order of the radiographic series remain unchanged.
The degree of training of the respondents, the years of experience, the country of the survey, the variability of surgical decision-making, were measured on a case-by-case basis and together with the responses on comparative and non-comparative radiographs, as well as the causal relationship between the response, by degree of training, years of experience and country of completion of the survey.
For the statistical analysis, the PSPP program was used, and the statistical significance of the variables was measured by T Student for the quantitative variables; and the Chi square for the non-quantitative variables, with significance set at p <0.05, the similarity ratio was assessed by linear regression with a Beta power set at 95% (B-5).
The study was considered without risk for the respondents, and approved by the ethics committee of the CIMB Foundation thus complying with the technical and administrative standards for health research included in resolution 008430 of 1993 of Republic of Colombia Health Ministry (Article 17).
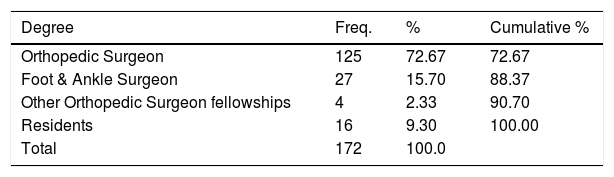
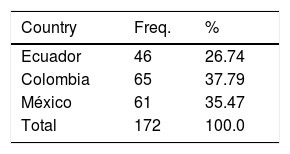
ResultsA total of 172 surveys were carried out, 90 were in comparative series and 82 non-comparative radiographs, the distribution by degree of training can be seen in Table 1. One hundred twenty five (125) orthopedic surgeons (72.67%), 27 foot and ankle surgeons (15.70%), 4 surgeons of other orthopedic subspecialties (2.33%) and 16 Orthopedics residents (9.30%) answered the surveys. 46 surveys were answered (26,74%) in Ecuador, 65 (37.79%) in Colombia and 61 (35.47%) in Mexico
100% of the respondents diagnosed the fracture of the distal fibula and inferred that the fracture line corresponded to a Weber B ankle lux fracture, both when viewing the series of unilateral radiographs, as the series of comparative radiographs for a positive predictive diagnostic value of the 100% and 100% negative predictive
The distribution between countries was documented in Table 2.
The experience of the respondents was measured in years with an average of 13.4 years standard deviation (DS) 9.79 (range 1-44)
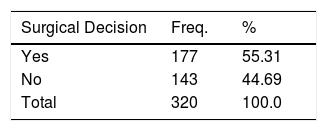
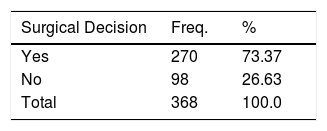
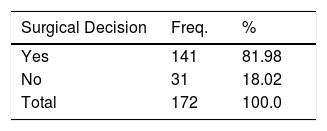
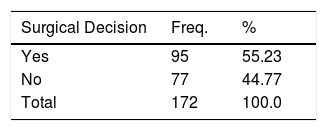
The responses of cases of unilateral radiographs were a total of 320. (Table 3), making a surgical decision 55.31% of respondents, with a statistical significance of p <0.5 when performing the independent analysis by clinical case. The surgical decision in the comparative radiographs with the explicit measures and the contralateral control radiographs corresponding to 368 cases (self-controlled group) showed that 73.37% of the respondents made a surgical decision with a statistical significance of p <0.5 when performing the independent analysis by clinical case. Table 4
When measuring how many professionals under study the 4 cases were considered surgical, it was found that on unilateral radiographs 14 (17.07%), they responded that the 4 cases were surgical, while on comparative radiographs 32 subjects (35.55%) considered Surgical the 4 cases, when measuring comparative and non-comparative, 46 subjects were successful in the 4 cases (26.74%)
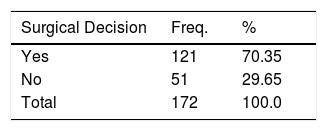
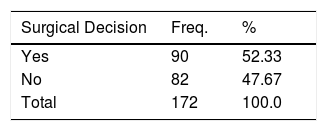
The surgical decision in cases regardless of the presence of comparative radiographs are shown in Tables 5, 6, 7 and 8.
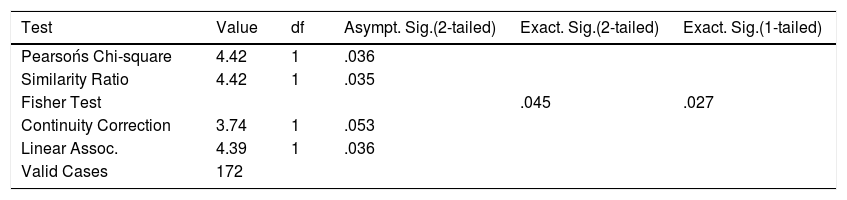
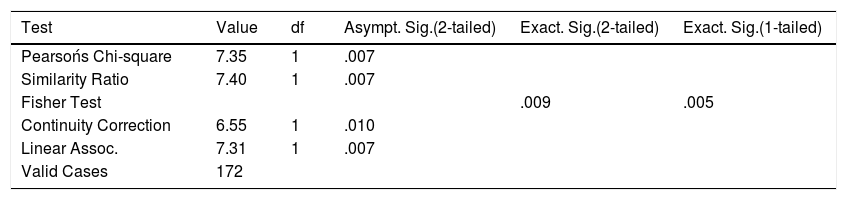
When crossing variables between cases and the presence of comparative and non-comparative radiographs per case, it was observed in Tables 9, 10, 11 and 12.
Cruce de variables entre radiografías comparativas y caso 1.
| Test | Value | df | Asympt. Sig.(2-tailed) | Exact. Sig.(2-tailed) | Exact. Sig.(1-tailed) |
|---|---|---|---|---|---|
| Pearsońs Chi-square | 4.42 | 1 | .036 | ||
| Similarity Ratio | 4.42 | 1 | .035 | ||
| Fisher Test | .045 | .027 | |||
| Continuity Correction | 3.74 | 1 | .053 | ||
| Linear Assoc. | 4.39 | 1 | .036 | ||
| Valid Cases | 172 |
Cruce de variables entre radiografías comparativas y caso 2.
| Test | Value | df | Asympt. Sig.(2-tailed) | Exact. Sig.(2-tailed) | Exact. Sig.(1-tailed) |
|---|---|---|---|---|---|
| Pearsońs Chi-square | 7.35 | 1 | .007 | ||
| Similarity Ratio | 7.40 | 1 | .007 | ||
| Fisher Test | .009 | .005 | |||
| Continuity Correction | 6.55 | 1 | .010 | ||
| Linear Assoc. | 7.31 | 1 | .007 | ||
| Valid Cases | 172 |
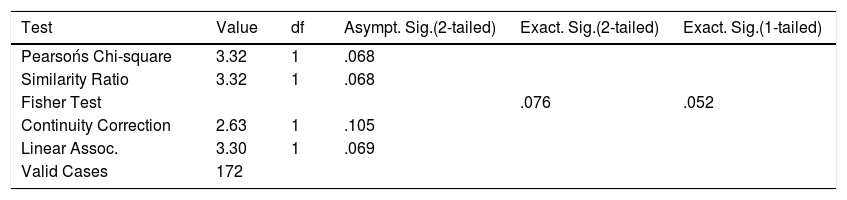
Cruce de variables entre radiografías comparativas y caso 3.
| Test | Value | df | Asympt. Sig.(2-tailed) | Exact. Sig.(2-tailed) | Exact. Sig.(1-tailed) |
|---|---|---|---|---|---|
| Pearsońs Chi-square | 3.32 | 1 | .068 | ||
| Similarity Ratio | 3.32 | 1 | .068 | ||
| Fisher Test | .076 | .052 | |||
| Continuity Correction | 2.63 | 1 | .105 | ||
| Linear Assoc. | 3.30 | 1 | .069 | ||
| Valid Cases | 172 |
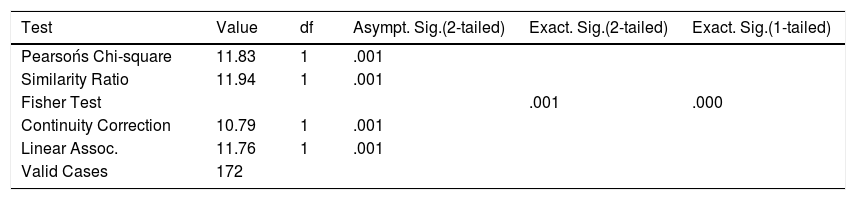
Crossing variables between comparative radiographs and case 4.
| Test | Value | df | Asympt. Sig.(2-tailed) | Exact. Sig.(2-tailed) | Exact. Sig.(1-tailed) |
|---|---|---|---|---|---|
| Pearsońs Chi-square | 11.83 | 1 | .001 | ||
| Similarity Ratio | 11.94 | 1 | .001 | ||
| Fisher Test | .001 | .000 | |||
| Continuity Correction | 10.79 | 1 | .001 | ||
| Linear Assoc. | 11.76 | 1 | .001 | ||
| Valid Cases | 172 |
When performing linear regression between the results of the surgical decision, training level, years of experience, country of origin, no causal relationship was found, with a beta power <95%. No observer made reference in the observations to a poor technique or quality of the radiological image.
DiscussionThe diagnosis of the distal fibula fracture and its inference to the Weber B ankle fracture dislocation pattern is made with a series of unilateral ankle trauma (AP, lateral and shroud), and no additional projections are required to perform it. However, according to our results, a unilateral radiographic series, in no way, makes it possible to objectify criteria for making a therapeutic decision.
Pott and Lane in 1894 were the first to consider that this type of lesions required an anatomical reduction, concentrating all surgical efforts to the stability of the medial compartment (tibial malleolus), performing surgical management only after a failed reduction in the conservative treatment. Subsequently, the AO group (association for osteosynthesis) in 1958 made anatomical reductions of the medial and lateral malleolus reporting excellent results. It is defined in the literature and biomechanical studies confirm that the tibia and astragalus are the joint that supports the most tension per unit area, which makes it very important that the joint contact surface must be preserved at all times as described by Ramsey and Hamilton and Lloyd et al.7,8 In lateral malleolus injuries, the talus follows the fibula, causing an alteration in the contact surface where 1mm of displacement reduces up to 42% of tibial talar contact area, causing irreversible damage to the articular cartilage. The ankle that corresponds to the most efficient load-kinetic energy transfer system described. It is responsible for an effective running kinetic chain by symmetrically distributing the load over a very small surface that supports 1.5 to 12 times the body weight depending on the speed of the march or the race. This load cannot be assumed per unit area by the ankle and is therefore handled biomechanically by transferring joint load to proximal or distal joints depending on whether the joint moment is in acceleration or deceleration.9 Small alterations in the ankle anatomy as a consequence of more than 1mm fibular displacement in sagital, coronal and axial (rotational) planes usually conduces to chronic pain able to evolve into functional osteoarthritis of the ankle.10 The further architectural damage of the ankle is a process subsequent to its functional damage, contrary to what occurs in pure load joints such as the hip and knee, where an architectural damage conduces to a further functional damage.
Controversy in the treatment of Fibular malleolus fractures persists over time, despite all the efforts made to have a better knowledge of the biomechanics of the ankle, the surgical decisions about patients with ankle fractures are still taken hastily with a single radiographic trump series, ignoring all the diagnostic tools that were described previously such as comparative radiographic series and are nowdays available such as tomography.
It has been recognized and is clear that isolated fractures of lateral malleolus (Weber b type) produce medial translation of the talus which biomechanically alters the loading surface of the joint. Most of the times, in ankle fractures there is a shortening of the fibula as well as rotation deformities of the distal fibula, in agreement with the measurements made in the study radiographs to which the respondents were exposed. To accurately diagnose such deformities, it is necessary to have the 3 radiographic projections described in the literature, have comparative projections and perform the respective measurements, for which an adequate technique and quality of the images is required. When these requirements are met, an adequate diagnosis can be made. In isolated fractures of the lateral malleolus, complete radiological measures should be performed, which allows establishing the degree of joint involvement, and thus let the surgeon be clear about the surgical or non-surgical decision making. An inter-observer concordance of 55.31% was observed in single radiographic series, while in comparative radiographic series a 73.37% inter-observer agreement (concordance) was observed. These concordances were neither influenced by the country of origin of the server, nor by the degree of training or years of experience. We did not find similar previous reports in literature.11
Although the scope of the study does not allow it to be demonstrated, we can infer that there is an “a priori” judgment of innocence about distal fibular fractures by respondents, given that only 26.47% of them made the appropriate therapeutic decision in the four series presented, regardless of whether Radiographs were comparative or not, 17.07% in the unilateral radiographs and 35.55% in the comparisons. This lead us to conclude that this a priori innocence judgment about the fracture could lead to inappropriate therapeutic decisions that result in high percentage of ankle osteoarthritis as described in previous reports by Donken et al, Glazebrook et al and Thomas et al.12–14
Meijer and Cols in 2015 determined the diagnostic accuracy of conventional radiography in the assessment of fractures of the posterior malleolus finding a poor correlation between radiographs and tomographic studies in three dimensions concluding that additional studies should be performed to adequately estimate the percentage of joint damage extension in these patients.15
Surgical treatment of weber B fractures with some radiological sign of joint involvement or displacement of contact area has shown better results in long term series by decreasing post-traumatic osteoarthritis developing and an overall decrease in pain signs referred by patients. It means that we, as surgeons, must be intolerant about residual deformities on ankle joint after a distal fibular fracture in order to improve our patients outcomes.16
Donken et al 17 found in their retrospective review of 288 patients with Weber B fractures a high incidence of non-union (up to 8%) as a consequence of underestimating their instability depending on the radiological criteria mentioned above when non surgical treatment was selected, and also found absence of Pseudoarthrosis after surgical stabilization, which adds another likely complication when an improper management of these injuries is performed.
Dong Yeo and Cols in 2015 18evaluated the results and complications of surgical treatment with blocked plates of Weber B fractures, finding excellent results in terms of function and improvement in ankle pain, by stabilizing the injuries in a safe and anatomical way, avoiding the development of secondary instability and allowing the proper functioning of the load/kinetic energy transfer system of the ankle.
We consider Weber B ankle fractures to be intra-articular fractures, with a high percentage of osteoarthritis secondary to inadequate reduction, with the presence of macro and micro-instability secondary to morphological alterations in the bone and ligament structures of the ankle.19 Because they are Considered a priori as innocent and daily-managed fractures, the perspective that they actually represent a potential risk of osteoarthritis for patients with severe functional, emotional and disability implications is easily lost. Additional imaging studies are required to restore joint stability and congruence with greater certainty during surgery, and further work is needed to clarify the usefulness of magnetic resonance imaging or computed tomography in patients with Weber B ankle fractures in order to carry out a correct pre-surgical planning of the management of these injuries, surgical decision-making and the type of technique to use in surgery.
Therefore, we conclude that a unilateral radiographic series and / or a comparative radiographic series are insufficient to treat a patient with a Weber B ankle fracture therapeutically. With the results obtained in the study, it is clear that ankle radiography is the gold standard in diagnosing distal fibula fractures, which at no time means that it has any utility in therapeutic planning and decision making in a Weber B ankle fracture.
Funding InformationStudy funding was independently performed by the researches
The research was funded by grant 001-17 from the CIMB Foundation.
DiclosuresNone
