




Currently, the age of onset for pubertal changes is decreasing, especially in girls, which may have an impact on psychosocial factors such as anxiety, self-esteem and body image. The aim of the present study is to compare these variables in two groups: a group of 15 girls with precocious puberty and a group of 16 girls of the same age without precocious puberty. A non-experimental descriptive design was used and the State-Trait Anxiety Inventory for Children (STAIC) and Self-Description Questionnaire (SDQ) were used to measure variables. Significant differences were found in Anxiety and Body Image levels between groups, but there were no differences in Self-Esteem levels. In conclusion, the findings show girls with early onset pubertal changes present high anxiety levels and negative body image compared to girls who start pubertal changes at the normal time.
Actualmente se está produciendo una disminución de la edad de inicio de los cambios puberales, particularmente en las niñas, lo cual puede incidir en variables como ansiedad, autoestima e imagen corporal. El objetivo es establecer una comparación de estas variables en 2 grupos: uno de 15 niñas diagnosticadas de pubertad precoz y otro grupo de 16 niñas sin ese diagnóstico. Se realizó un diseño descriptivo no experimental, y para la medición de variables se utilizaron el State-Trait Anxiety Inventory for Children (STAIC) y el Self Description Questionnaire (SDQ). Se encontraron diferencias significativas entre ambos grupos en los niveles de ansiedad y de imagen corporal, pero no en los de autoestima. A través de los hallazgos obtenidos, se evidencia que las niñas que inician los cambios puberales de manera precoz sufren altos niveles de ansiedad y tienen una imagen corporal de sí mismas más negativa que las niñas que inician los cambios puberales en el momento normativo.
Puberty is the name given to all of the changes occurring in the second stage of life which transform a child's body into an adult body with reproductive capacity, gonad maturation, secondary sex characteristics, somatic growth and bone maturation.1,2 It is a stage that entails multiple biopsychosocial changes in girls, so the vast research undertaken by various fields of study including paediatrics, paediatric endocrinology, psychology and psychiatrics, among others, is not surprising.
According to Pasqualini et al.,3 in girls, breast development (thelarche) is the first normative sign of puberty, which occurs at a mean age of 10.8 (range, 8.3–13.3) years. Following the breast buds, the appearance of pubic hair (pubarche) and underarm hair is customary. Menarche (first occurrence of menstruation) is one of the last events in the sequence of female pubertal changes, occurring approximately two years after the appearance of breast buds, and marks the onset of the girl's sexual maturity.4,5
Pubertal changesThe onset of all these pubertal changes is the result of the activation of the hypothalamic–pituitary–gonadal axis, which during this period increases the pulsatile secretion of gonadotropin-releasing hormone (GnRH), stimulating the pituitary glad to produce luteinising hormone (LH) and follicle-stimulating hormone (FSH).1,6 GnRH activation leads to biochemical and morphological interaction with neuronal and glial subpopulations through inhibitory and trans-synaptic excitatory stimuli, adhesion molecules, transcription factors, lipid derivatives and growth factors,7 giving rise to the onset of puberty-related changes.
Advances in neuroimaging techniques have enabled the more accurate definition of a significant proportion of the cerebral changes that occur throughout puberty, and these have been found to occur primarily in the prefrontal cortex and cortical and subcortical limbic regions.8,9 During puberty, a significant increase in synaptic density is observed in the prefrontal cortex due to the occurrence of synaptogenesis, after which a pruning process takes place on abundant neuronal connections that are not being used.6,8,10 The myelination process is another notable cerebral change to occur during puberty, whereby a progressive increase of white matter is observed, improving the speed and efficacy of neuronal communication.6,8
Likewise, the corticolimbic connections involved in analysing high-risk situations, planning, decision-making, behavioural self-regulation and impulse control are found to be at their peak, influenced by neuroendocrine and environmental factors,2,11 causes which explain the behavioural changes that occur in this period of development. Similarly, oestrogen and androgen secretion reaches such high levels in the brain that they cause changes in the modulation of certain cognitive capacities, such as learning, memory, behaviour and emotions.6,12 Knowing the prefrontal cortex's influence on executive function and behavioural self-regulation, and taking into account that this area of the brain remains in the midst of the maturation process up until the end of this stage, it is reasonable to believe that the behaviours typically associated with adolescence owe to these developmental processes.
As regards the psychosocial element, during puberty, girls are confronted with a new role and struggle between the roles of girls and adult women that society imposes. It is thus easy to understand that, at the onset of all these changes, there may be negative emotions and insecurity regarding body image and self-esteem, also taking into account that increased gonadal hormone secretion greatly influences neural changes in the prefrontal cortex, striatum and amygdala, which cause greater levels of emotionality.13 López et al.12 show that, during the brain's pubertal maturation, there is a vast emotional response and high expectations of reward and motivation due to the activation of specific dopaminergic pathways.
Early puberty onsetThe results provided by the Pediatric Research in Office Settings (PROS), Lawson-Wilkins Pediatric Endocrinological Society (LWPES) and National Health and Nutrition Examination Survey (NHANES) III studies reveal that there has been an advance in the age at onset of puberty3,5,14 which may lead to a series of adverse psychological effects.
There is currently a worldwide trend towards a decrease in the age at onset of the first characteristics associated with puberty. This is, in part, due to environmental pollutants that exert an oestrogenic effect, with a self-limited secular trend.15 Various studies1,16–19 have found that the advance in normative age is influenced by epigenetic conditions, perinatal conditions, nutritional statuses of obesity, chemical and endocrine interferences, altered light and dark cycles, earlier releases of GnRH due to constant stress exposure and other chronic diseases.
Precocious puberty (PP) is thus understood as a phenomenon characterised by the onset of secondary sex characteristics at a non-physiological age (considered to be 8 years in girls) whereby complete sexual maturation and adult stature is reached.20,21 Progressive PP is considered to be puberty which, as well as starting early, quickly evolves in terms of physical development, bone maturation and growth. Therefore, drawing on clinical, hormonal and radiological findings is of the utmost importance for proper diagnosis.20
Nevertheless, it should be taken into account that there are racial differences regarding the age at onset of the first signs of pubertal maturation. In the cross-sectional studies performed, it was found that Caucasian girls started puberty 1–1.5 years later than Afro-American girls, of which 37.8% presented breast development earlier than 8 years of age, compared to 10.5% of Caucasian girls.22,23
PP has a total annual incidence of 29 in 100,000 females (with a female:male ratio of 20:1), and there are data worldwide regarding a growth in prevalence of 3.5/100,000 cases per year.9,11,14 In a study carried out between 1997 and 2009, under the auspices of the Spanish Paediatric Endocrinology Society (Sociedad Española de Endocrinología Pediátrica, SEEP), Soriano-Guillén et al.24 found a total of 226 girls diagnosed with PP variants (central PP [CPP]) versus a total of 24 boys with the same diagnosis.
Between normal puberty and PP, there is a population in a “borderline” situation, which can be defined as early puberty (EP). Although there is a lot of discussion surrounding the age at onset of the latter, EP is generally understood to be the onset of pubertal signs between 8 and 9 years of age.25,26 Although EP is considered a normal variant of puberty, it is approached in the same way as PP in practice since it may end up having negative repercussions both on final stature and on social and psychoemotional factors.15,26,27 Complementary investigations into bone age, the uterine body-to-cervix ratio and hormonal analyses provide the definitive differential diagnosis.15
Given that EP is not necessarily a pathological condition, it is difficult to find data on the incidence and prevalence thereof.28 However, it has been estimated that 16.5% of girls aged 7–8 years experience isolated thelarche29 as a sign of EP.
Aetiology of precocious pubertyThe causes that give rise to PP may have a central (CPP) or peripheral (PPP) origin. As regards CPP, the Spanish Obstetrics and Gynaecology Society (Sociedad Española de Ginecología y Obstetricia, SEGO)21 highlights that the condition is caused by the activation of the hypothalamic-pituitary axis, so it is considered GnRH-dependent. CPP may be activated by idiopathic causes or central nervous system disorders (such as hypothalamic hamartomas, astrocytomas, pinealomas, hydrocephalus malformations and agenesis of the corpus callosum, among others).21,30 Unlike PPP, CPP affects a neuroanatomical substrate on the hypothalamic–pituitary–gonadal axis.1,31
PPP may be defined as PP that has not begun due to the activation of the hypothalamic-pituitary axis (irrespective of GnRH), the origins of which are ovarian tumours, functional cysts, adrenal gland disorders and McCune-Albright syndrome, etc.21 While in CPP, secondary sex characteristics emerge in a harmonious and expected sequence, in PPP the appearance of breasts or pubic hair follows no ordered chronological sequence.32
For the most part, precocious puberty cases are GnRH-dependent, so correspond to CPP, with a prevalence of 98% of all of the PP cases presented.15
In order to diagnose PP, a detailed history is required alongside a physical examination that helps to determine the girl's Tanner pubertal development stage. It is also necessary to determine physical characteristics such as height, weight and other signs (body odour, acne, gynaecomastia, galactorrhoea, leucorrhoea, etc.).25 Moreover, hormone levels (FSH, LH, TSH, etc.) should be determined and imaging tests performed (head MRI, ultrasound to measure the uterine body-to-cervix ratio and X-ray to estimate bone age, among others).15,21,25
Associated psychological effectsThe significant increase in data on the incidence of PP has led to growing interest in studying patients diagnosed with PP with the objective of analysing the biological, psychological and social factors involved. From a psychological perspective, the factors that most commonly affect this population have been studied; the most examined aspects are body image, self-esteem and symptoms associated with anxiety, depression and stress.
One classical view when studying the psychological effects of precocious puberty is Caspi and Moffitt's “stressful change hypothesis”,33 where it is argued that transitional periods such as puberty are universally considered to be stressful experiences that may end up causing the onset of psychopathologies. Given that the physical changes that occur throughout life have a certain psychological impact, Mendle et al.34 highlight that in cases of PP this impact could be more negative. The psychological consequences of girls reaching puberty early are even worse for those who mature in a normative stage, due to difficulties adapting to the physical and psychological changes that occur prematurely and quickly outside of the expected timeframe.4,25,35
Similarly, biological theories on maturation dysfunction assert that, because of the huge hormonal changes that accelerate PP, symptoms of excitation, nervousness or excessive emotionality appear, typical characteristics in cases of anxiety.36 At present, various studies uphold these theories, demonstrating that, in case of the onset of precocious puberty, there is a greater risk of suffering lifelong anxiety than when puberty occurs at the normative stage.37,38 In a literature review carried out by Reardon,39 consistent results were found, associating early maturation in girls with a greater probability of anxiety disorders and evidence that these effects are clinically persistent and significant.
Moreover, Kim et al.1 note that, due to premature growth plate closure, which leads to small stature, social complications may arise, as peers may perceive this physical development—in its different manifestations—as strange, which would lead to their isolation from pertinent social groups as well as psychological damage that will cause the girl with PP to suffer from anxiety and insecurity regarding her body image. Understanding body image as the mental image one has of one's own body and the emotional reactions towards it, when in puberty there are physical appearance-related concerns, psychological and social development is hindered.40
In this regard, Palacios et al.,41 from the classical study of developmental psychology, sustain in their hypotheses that the psychological consequences on body image, in general, are unfavourable for girls, since the increase in body fat engendered by the pubertal stage is not in line with female beauty standards, which are currently associated with slimness. This leads to negative self-image and a high incidence of eating disorders.3
Since the physical appearance of girls with PP resembles that of an adult woman, they may be forced to hesitantly face situations for which they are neither emotionally nor cognitively ready, leading to low levels of self-esteem.40 Self-esteem is understood to mean a personal evaluation of worth, the acceptance with which people perceive their self-image, both in comparison to others and themselves, and continues to change throughout the developmental cycle, with huge changes seen during puberty.
In light of these possible psychological problems associated with PP, broader research is of the utmost importance in order to reduce the difficulties that arise as girls facing precocious maturation adjust to puberty, and it is paramount that we understand the psychological variables that are affected in these processes in order to seek better prevention and intervention alternatives that approach PP in an integral manner.
Thus, the overall objective of this research is to compare a sample of subjects with PP to another of the same age in whom said changes have not yet started. The specific objective is to compare anxiety levels, self-esteem and body image between both sample groups, hypothesising that, in the group with PP, anxiety levels will be higher, self-esteem will be lower and that the concept of body image will be more negative than in the group of girls not affected by PP.
MethodsInvestigation designDue to the degree of control, this research is a non-experimental, cross-sectional field study. Taking into account the objective or knowledge being sought, this is a descriptive study.
The sample of participants was chosen from a population of patients from different localities in the province of Alicante, Spain. A total of 31 girls were intentionally included, adopting two non-probabilistic cut-off criteria: (a) PP case group: selection using the non-probabilistic method based on the specific criteria proposed by the investigators (15 patients with a diagnosis of PP or EP in their different manifestations), and (b) non-PP case group: intentional selection using age and education pairing criteria according to the case group (16 subjects with no PP diagnosis).
The inclusion criteria were as follows: aged between 8 and 12 years-old, diagnosis of PP or EP according to the criteria established and verified by a paediatric endocrinologist, and no diagnosed neurological or psychiatric disorder, including traumatic brain injury, epilepsy, childhood depression, learning difficulties or autism spectrum disorder, as demonstrated in a clinical history through a semi-structured interview with the parents.
The PP group presented some sign of PP diagnosed in the past year by the Paediatric Endocrinology Unit of the Hospital General Universitario de Elche [General University Hospital of Elche]. Ages ranged between 8 and 12 years and all of the girls were educated and belonged to a medium-to-high socioeconomic class. Among them, there were cases of pubarche, thelarche and EP (with clinical suspicion of tall stature, body odour or advanced bone age), some of whom received pharmacological treatment with analogues.
The non-PP group included a total of 16 girls from the province of Alicante (Spain), of a medium-to-high socioeconomic status and all of whom were educated, the majority at private schools.
Instruments and techniquesIn order to collect the sociodemographic data, a series of questions was designed that gathered age, date and place of birth, school year, school, diagnosis, time of diagnosis, pharmacological treatment and duration of treatment (only in the PP group).
As a measure of anxiety, the Spanish version of the State-Trait Anxiety Inventory for Children (STAIC)42 was used, as adapted by Seisdedos,43 in particular the section on state anxiety, which is described as an emotional state characterised by subjective feelings of tension and apprehension and hyperactivity of the autonomic nervous system. It contains 20 items, with a 3-point Likert-type response format (not at all=1, somewhat=2 and very much so=3), where higher score indicates greater anxiety levels. The STAIC obtains high internal consistency coefficients in various studies, of around 0.8.43 The application time of the test is approximately 10min.
To assess self-esteem and body image, we used Marsh's Self Description Questionnaire (SDQ-I),44 which is based on the hierarchical, multifaceted model proposed by Shavelson et al.45 It measures 11 facets of self-concept for preadolescents; we selected the physical appearance variable (to measure body image) as well as the one relating to self-esteem. The SDQI has repeatedly obtained acceptable internal consistency and test–retest reliability estimations and has been adapted and validated for use in the Spanish population.46
The body image and self-esteem variables comprise 8 and 10 items, respectively, with a Likert-type response scale ranging from false (1) to true (6). The average application time was 15min. The higher the scores obtained, the better the levels of self-esteem and body image perception.
ProcedureAn interview with the Head of Paediatrics of the Hospital General Universitario de Elche was conducted in order to gain access to patients with either a diagnosis or prediagnosis of PP who were attending paediatric endocrinology consultations. A short interview was carried out with the parents or relatives of the participants in order to explain the study and request their informed consent prior to the application of the questionnaires.
For the non-PP population, we made telephone contact with the Head of the Alfas del Sol Sports Centre and Summer School, who granted the relevant permissions for accessing the sample, taking into account the aforementioned exclusion criteria. Once the sample of the 16 girls selected had been established, we sent their parents an information letter about the study that was due to take place and, after the informed consent form had been signed, we proceeded to individually apply the questionnaires to each of the girls in the control group.
Ethical considerationsThe authors state that this article contains no participant data and that the procedures performed conformed to the standards set forth in the 2008 World Medical Association Declaration of Helsinki on ethical principles for medical research involving human beings. The informed consent of parents, guardians or the legal representative was collected and anonymity and data confidentiality ensured.
Data analysisData analysis was performed using SPSS software, version 18. First, we carried out a descriptive analysis of the mean±standard deviation of the direct scores obtained on the scales applied. Moreover, non-parametric comparative analysis (Mann–Whitney U test) was undertaken to establish any differences in scores between both study groups.
ResultsIn relation to the results obtained, the results of the descriptive analyses of both samples are detailed first, including the mean age and age at diagnosis, the type of diagnosis established and the frequency of the pharmacological treatment.
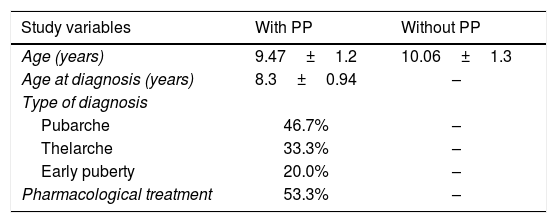
In the PP group, the mean age was 9.47±1.2 years and the age at diagnosis by the paediatric endocrinologist, 8.3±1.3 years. It should be noted that, in each and every case, there was previous diagnostic suspicion on the part of relatives or carers, which was the main reason for them attending the medical consultation. Seven cases of pubarche, five cases of thelarche and three cases of EP were found. 53.3% of these girls were undergoing pharmacological treatment with LH-RH analogues to halt GnRH secretion through receptor saturation (Table 1).
Description of the sample of participants.
| Study variables | With PP | Without PP |
|---|---|---|
| Age (years) | 9.47±1.2 | 10.06±1.3 |
| Age at diagnosis (years) | 8.3±0.94 | – |
| Type of diagnosis | ||
| Pubarche | 46.7% | – |
| Thelarche | 33.3% | – |
| Early puberty | 20.0% | – |
| Pharmacological treatment | 53.3% | – |
PP: precocious puberty.
Values are expressed as the mean±standard deviation.
When analysing the participants’ body image perceptions, we can observe that the score obtained was lower in the PP sample (mean, 30.13 points), which would indicate that their self-image is more negative than in the non-PP group (36.25) (Table 2).
Mean scores and comparison of the study variables.
| Study variables | PP group scorea | Non-PP group scoreb | Mann–Whitney U test | Z | p (two-tailed)c | p (one-tailed) |
|---|---|---|---|---|---|---|
| Anxiety | 41.20±6.63 | 25.38±4.12 | 6.500 | −4.502 | <0.01 | <0.01 |
| Self-esteem | 46.07±4.20 | 47.94±5.87 | 80.500 | −1.567 | 0.117 | 0.119 |
| Body image | 30.13±7.71 | 36.25±7.07 | 63.500 | −2.243 | 0.025 | 0.024 |
PP: precocious puberty.
Unless otherwise indicated, values are expressed as the mean±standard deviation.
Similarly, the results obtained on the anxiety variable, where there are significant differences in the means of both groups, indicate a more widespread presence of anxiety in the PP group (41.20 versus 25.38 in the non-PP group) (Table 2).
Said anxiety, self-esteem and body image variables were examined using a comparison of means statistical analysis, and different significances were recorded regarding the mean scores for the body image (U=63.50; p=0.024) and anxiety variables (U=6.50; p<0.001) of both groups. No major significance was seen in the self-esteem variable (Table 2).
Thus, we were able to observe differences between the mean scores achieved by both groups. These differences are significant in the scores relating to the body image and anxiety variables, although there does not appear to be wide discrepancies in self-esteem.
DiscussionPuberty is a complex process that occurs as a result of the activation of the hypothalamic–pituitary–gonadal axis and has a huge physical, psychological and social impact, especially when maturation does not occur at the expected time. Precocious puberty in girls has been associated with a greater risk relating to the prevalence and persistence of mental disorders in adolescence and adulthood.34,47,48 Thus, this study has focused on investigating the psychological effects of PP on girls, primarily addressing anxiety, self-esteem and body image.
The objective focused on comparing anxiety levels, self-esteem and body image in a sample of subjects with PP to another of the same age in whom said changes had not yet started. Although more studies are needed, the change hypothesis is supported by many, which propose that the changes occurring during puberty have a greater negative psychological impact when puberty takes place earlier than expected,33,34,38 which could be verified in certain variables where the results had worse scores in the PP group. The original working hypothesis, that anxiety levels would be higher and self-esteem and body image more negative in the PP group, was confirmed by the anxiety and body image variables.
After applying the different tests, it was verified in the body image variable that the PP group obtained a mean score that indicated a worse body image concept than in the non-PP group. Due to the fact that girls’ physical appearances mature during puberty, they are forced to adapt and change their social standards and expectations prematurely, which often implies confronting and reorganising their identity and perception of themselves,34 potentially damaging the image they have of their bodies.
Our results are coherent with theories which argue that, in the early stages of puberty, girls are preoccupied with and insecure about how their bodies look, and that it is through social comparison with their peers that, little by little, they start to accept their new body image.35 Taking into account the fact that the bodies of girls diagnosed with PP begin to change several years before their peers, these processes of comparison result in incongruities that lead them to perceive these changes as strange and negative, and may lead them to acquire a more negative outlook based on how different their bodies are to those of their peers.34
In this sense, current beauty ideals, which in our society equate to standards of slimness, cause body dissatisfaction, given that there are discrepancies between the body desired and the body perceived.41 The female body's increase in body fat which underlies puberty (and causes girls to accumulate more fat on their buttocks, abdomen, hips and thighs) distances them from socially accepted ideals reinforced by the media, promotes a negative body Image 3,41and constitutes a risk factor for the subsequent presentation of eating disorders. On this basis, Klump49 asserts that puberty is one of the most critical risk periods for developing eating disorder-related symptoms, due to the psychosocial effects of maturation, such as body dissatisfaction and low self-esteem. Cross-sectional and longitudinal studies associated the early onset of puberty with a greater incidence of eating disorders and anxiety symptoms that persisted into adulthood, partly due to hormonal mechanisms.47,48 The early detection of low self-esteem levels and poor body image satisfaction could serve as an indicator for prevention and early intervention in eating disorders and anxiety.
As regards the anxiety variable, vast differences were observed between the mean scores for both groups, with these being higher in the PP group. According to various authors, in the study of psychological effects resulting from puberty, this increase in anxiety is due to the fact that pubertal development (a phase that often causes anxiety), when it occurs at a non-normative or unexpected time, serves to increase anxious symptoms and may lead to physiological and behavioural sequelae.33,39,50 Biological theories on maturation dysfunction assert that the enormous hormonal changes that trigger precocious puberty give rise to symptoms of excitation, nervousness or excessive emotionality—characteristics typically related to cases of anxiety36—which would explain the huge differences between the scores obtained by both study groups and, moreover, coincides with the other authors’ results who have found that the risk of suffering anxiety disorders positively correlates with subjects who began puberty early.37,38
Regarding the results of the self-esteem variable, one could speculate that the higher the body dissatisfaction seen in our results, the lower the self-esteem would be. However, the results have not been able to reflect clear differences between the self-esteem levels of the groups with and without PP, despite the fact that a more negative body image was apparent. Generally speaking, it can be said that self-esteem during this phase is influenced by both physical factors and academic/social competence.51,52 For that reason, in future studies it would be useful to examine whether academic and social aspects have acted as determining factors that made self-esteem levels less disparate, or to consider the application of different instruments that assess self-esteem in girls.
As a final reflection, it is important to take into account the fact that the results regarding the psychological effects of PP are not conclusive. It is therefore necessary to continue researching the topic, preventing any possible study limitations so that investigators may provide solid evidence for research on PP.
Since it is considered that the hospital's influence—where the data was collected and the patients were treated with LH-RH analogues—might have interfered with the anxiety results of the PP group, this would constitute a reason for controlling both variables in future studies. On this basis, much of the literature on anxiety and puberty39 notes that childhood experiences or anxiogenic disorders that advance pubertal timing could also play a role, thus meriting a more in-depth and controlled analysis. Lastly, it should be taken into account that conducting a retrospective report has evident limitations, so the possibility of selecting subjects where less time has elapsed between the PP diagnosis and psychological assessment is proposed, in order to reduce possible bias, as well as to increase the size of the sample of girls diagnosed with PP. Given that no systematic assessment was undertaken regarding the pre-existence of anxious or affective disorders in the sample group, the results should be analysed with caution, and we propose measuring these variables in medical histories in future studies.
In conclusion, during puberty girls find themselves in an optimum state of physical health, but are far more unstable psychologically and socially. The psychological repercussions inherent to pubertal maturation compel healthcare professionals to perform closer monitoring of all pubescent children, particularly those maturing early, in order to prevent the onset of mental illnesses that persist into adulthood.
Ethical responsibilitiesProtection of people and animalsThe authors state that the procedures followed conformed to the ethical standards of the responsible committee on human experimentation and to the World Medical Association and the Declaration of Helsinki.
Data confidentialityThe authors declare that they have followed the protocols implemented in their place of work regarding the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Mercader-Yus E, Neipp-López MC, Gómez-Méndez P, Vargas-Torcal F, Gelves-Ospina M, Puerta-Morales L, et al. Ansiedad, autoestima e imagen corporal en niñas con diagnóstico de pubertad precoz. Rev Colomb Psiquiat. 2018;47:229–236.
