



Othello syndrome, an eponym of Shakespeare's character, is a transnosological diagnostic term that designates a clinical picture characterised by the presence of delusions of infidelity with respect to a partner and that, consequently, can lead to typical jealousy attitudes and violent behaviour towards the partner. In its pure form, it corresponds to delusional disorder of infidelity, but it may also be secondary to brain organicity and drug use.
MethodsCase report and non-systematic review of the relevant literature.
Case presentationA 26-year-old man, with a history of drug abuse and a victim of domestic violence as a child, presented with tonic–clonic seizures and intracranial hypertension three years ago, for which he underwent a craniotomy with the finding of a right frontal cerebral tuberculoma. After a lapse, he developed a clinical picture of delusions of infidelity regarding his partner and violent behaviour towards her.
Literature reviewDelusional jealousy is associated, like other delusions, with lesions of the right frontal lobe. Despite the high and growing prevalence of tuberculosis worldwide, there are no reported cases of Othello syndrome secondary to cerebral tuberculoma in the literature.
ConclusionOthello syndrome, although not the main cause of domestic violence, can be associated with particularly violent manifestations and be secondary to cerebral tuberculoma. This is the first published case of its kind.
El síndrome de Otelo, epónimo del personaje de Shakespeare, es un término diagnóstico transnosológico que designa un cuadro caracterizado por delirios de infidelidad respecto a la pareja que, por consiguiente, puede acarrear actitudes celotípicas y conductas violentas hacia ella. En su forma pura, corresponde al trastorno delirante de infidelidad, pero también puede ser secundario a organicidad cerebral y a consumo de drogas.
MétodosReporte de caso y revisión no sistemática de la literatura relevante.
Presentación del casoVarón de 26 años con antecedente de consumo de drogas y víctima de maltrato infantil, 3 años antes había sufrido crisis convulsivas tónico-clónicas e hipertensión intracraneal, por lo que se sometió a una craneotomía, en la que se halló un tuberculoma cerebral frontal derecho. Tras un lapso, comenzó con delirios de infidelidad y conductas violentas hacia su pareja.
Revisión de la literaturaLos celos delirantes se asocian, como otros delirios, a lesiones del lóbulo frontal derecho. Pese a la elevada y creciente prevalencia mundial de tuberculosis, no se han publicado casos de síndrome de Otelo secundario a tuberculoma cerebral.
ConclusionesEl síndrome de Otelo, aunque no es la principal causa de violencia doméstica, puede asociarse con manifestaciones particularmente violentas y ser secundario a tuberculoma cerebral. Este es el primer caso de tal índole que se publica.
According to the Oxford English Dictionary, being jealous means, “feeling or showing a resentful suspicion that one's partner is attracted to or involved with someone else”.1 Jealousy, obviously not of an erotic nature, can be observed as instinctive behaviour in infants as of six months of age, providing a clear idea of the omnipresence of this psychic phenomenon in the human condition.2 But although it is biological in nature, jealousy has an unquestionably sociocultural demarcation, to the extent that what decades ago was an expression of normal jealousy would be morbid today; in turn, this changing boundary blurs the distinction between normal jealousy and pathological jealousy. The latter include jealousy of a delusional nature, in which the psychopathological nucleus is made up of delusions that the partner is being erotically and sexually unfaithful.3 This phenomenon is classically called Othello syndrome and it has been reported as stemming from various aetiologies: primary psychiatric, organic brain injury and psychoactive substances. It has been suggested that pathological jealousy should also include jealousy of an obsessive nature or formed by overvalued ideas; the limits between these phenomena are not always clear.4
On the other hand, tuberculosis (TB) is the endemic disease with the highest prevalence worldwide: it has an incidence of 10 million new cases a year, half a million of which are resistant to multiple drugs.5 In Peru, in 2015, a morbidity rate of 73.33 cases/100,000 inhabitants was recorded and 1686 cases were multi-drug-resistant.6 Between 10% and 15% of all cases of TB have central nervous system (CNS) involvement. Tuberculoma or tuberculous granuloma (the cause of 15%–30% of cases of CNS TB) is a histopathological form consisting of a caseous necrosis centre in which there may be latent tuberculosis bacilli, encircled by an irregular capsule of fibrous tissue, giant multinucleated cells and lymphocytes, with oedematous outer borders and astrocyte infiltration. Tuberculoma is the most common form of brain parenchyma disease and is known to have a predilection for settling in the frontal lobes in adults.7
To our knowledge, there are no previous reports in the literature of Othello syndrome stemming from CNS tuberculosis. This has prompted us to present this clinical case.
Case reportA 26-year-old male who lived with his partner. He had a poor secondary education and behavioural issues: cruelty to animals, impulsiveness and scant tolerance of frustration. He came from a dysfunctional home: his father was alcoholic and violent. From the age of 17 he had been drinking alcohol and using marijuana and cocaine paste; in the last 5 years he had been using all three every weekend. He claimed to have given up using due to brain surgery he had. He was also jealous and aggressive in his relationship with his partner.
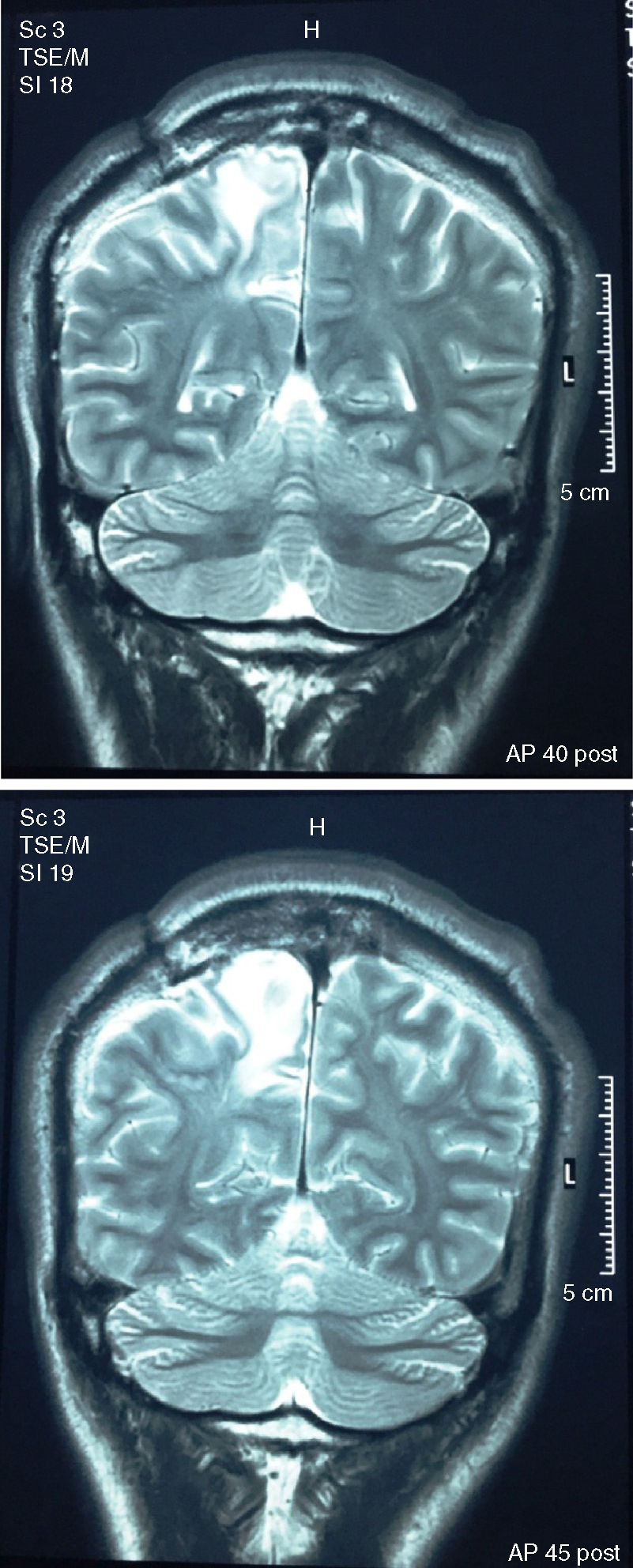
Three years prior to the present illness, he had suffered generalised tonic–clonic seizures, with sphincter relaxation, tongue-biting and eye sursumversion. After three months without symptoms, the latter reappeared with greater frequency (up to 10 seizures a day). After a medical evaluation, he was admitted to the intensive care unit with a diagnosis of epilepsy and intracranial hypertension. Brain magnetic resonance imaging (MRI) showed a “hyperintense para-sagittal image in the right frontal-parietal brain region with a large area of vasogenic oedema of approximately 2.5cm×3.5cm”. The patient was stabilised and scheduled for a right parietal craniotomy, in which the tumour mass of approximately 0.5cm×0.5cm was resected: the pathology study revealed “brain tissue with glial reaction and histiocytes with granulomatous tendency, consistent with tuberculous granuloma”, whereupon he was started on the Ministry of Health anti-tuberculosis treatment regimen (12 months). After the operation, the patient was given prophylaxis with carbamazepine 400mg/day for one year, followed by 200mg/day, although he took it intermittently. He had no further epileptic seizures during that time. A follow-up MRI scan four months before the present illness showed residual lesions in the affected area, described as “area of oedema with finger-like pattern in the right frontal para-sagittal white matter” (Fig. 1).
 taken 4 months before the onset of the psychosis and 2.5 years after the surgical excision of the tuberculoma. The radiological report describes “large area of oedema with finger-like pattern in right frontal para-sagittal white matter.”")
Magnetic resonance imaging of the brain (coronal plane in T2 without contrast) taken 4 months before the onset of the psychosis and 2.5 years after the surgical excision of the tuberculoma. The radiological report describes “large area of oedema with finger-like pattern in right frontal para-sagittal white matter.”
His current illness had been coursing for three months: after comments from a close friend, he went to complain to his partner for talking to a neighbour too much. Since then, she had noted that the patient was suspicious and hypervigilant. Sometimes he would come home early from work and spy on her. When she confronted him about it, he judged her anger as a sign of deceit and betrayal. The patient began to refer to alleged memories of past infidelities: he had supposedly witnessed sexual encounters between his partner and several other men years before but had remained silent “for the sake of their children”. His sexual appetite increased and he demanded they film their sexual intercourse on his mobile phone. These delusions of infidelity went on to involve the patient's own father, and he accused her of sleeping with him for money.
Finally, after a huge argument, the patient had several clonic movement seizures, without falling to the ground, while sobbing with his eyes closed and performing defensive movements. These seizures were not accompanied by sphincter relaxation, eye sursumversion or tongue-biting, and the subsequent recovery was immediate and without postictal sequelae. During that period, the patient continued to demand sexual intercourse from his wife up to twice a day in order to “prevent further infidelities”.
He was referred to psychiatry for these apparent seizures. The psychiatric examination highlighted the patient's dysphoric mood compounded by prominent delusions of infidelity and fantastic paramnesias (i.e., he experienced certain figments of his imagination as if they were memories: for example, he claimed to have seen videos of his wife's sexual acts with former partners, even from her adolescence, describing the intercourse in great detail). He had no hallucinations or disorganised affect or speech. He threatened to kill himself so that his partner would get sent to jail. He lacked insight into his own condition. A follow-up computed tomography scan showed no new lesions since the aforementioned magnetic resonance imaging.
He was started on treatment with olanzapine 10mg/day. One month later, the patient's mood had improved, but as the delusions of infidelity persisted, his partner left him due to the abuse she was receiving. Sulpiride 600mg and carbamazepine 200mg were subsequently added to the treatment and the dissociative seizures ceased, at least temporarily.
DiscussionThere are no accurate figures on the prevalence of pathological jealousy or delusional infidelity disorder. In 2011, Soyka8 reported an infidelity delusion rate of 0.5% among hospitalised psychiatric patients. In 2008, Portugal9 found that 5.5/100,000 population met the criteria for delusional infidelity disorder. The literature suggests that delusional jealousy tends to be more common in men (although more recent evidence questions this) and its prevalence increases with age.4,10 Moreover, 10% of the general population reportedly worries, with feelings of jealousy, without any gender differences.4 Between these statistical extremes, a large set of people suffer from psychic phenomena related to jealousy and violence against their partners. There is no doubt that jealousy, pathological or not, is the most common catalyst in the world for uxoricide.11
The frequency of each aetiology (primary psychiatric, organic or secondary to psychoactive substances) in Othello syndrome varies due to the very small number and heterogeneity of the case series. For example, in Graff's recent series,12 69.5% of Othello syndrome cases had an organic cause. Other series find a much lower rate of organicity: the average with this aetiology fluctuates around 30%.4,13
Lesions to both hemispheres have been found to produce psychosis in a similar proportion (but right temporal-parietal involvement is slightly predominant), although psychosis secondary to focal brain injury is generally rare.13 Although localised cerebral aetiology has been reported in a considerable number of cases of Othello syndrome, infidelity delusions have also arisen from non-focal conditions such as normal pressure hydrocephalus, various encephalitis, multiple sclerosis, Alzheimer's disease and Parkinson's disease.10 Even with focal lesions, there is still debate over whether or not the affected cerebral hemisphere is decisive. Some recent findings point to a greater involvement of the right hemisphere, specifically the frontal lobe,12 precisely, as in our case, where tuberculomas tend to take root most.
It has been argued that the greater frequency of psychosis-generating frontal lesions of the right hemisphere can be explained by the fact that this brain area is responsible for the processing of emotions linked to complex stimuli (e.g. understanding other people's intentions in social interaction or moral reasoning) as is the case of situations linked to jealousy; with this area injured, misinterpretation and integration of irrelevant stimuli would be feasible. If the left cerebral hemisphere is left unscathed, instinctive tendencies related to partner possession (such as the hyper-erotic behaviour of our patient) would be triggered and the consequent jealous delusional thinking might be expressed.11
Our patient had demonstrated his proclivity to jealousy from the premorbid stage. Insecure and unstable childhood links (such as those due to domestic violence and childhood abuse in our patient) have been identified as a predictive event of jealous attitudes in adulthood.4 The subsequent presence of extensive tuberculoma, with its correlate of intense inflammation, in addition to its space-occupying nature (to the point that it produced intracranial hypertension) and its subsequent scarring and oedematous sequelae, was the unavoidable stimulus for the onset of the organic delusional symptoms in our patient. It should also be pointed out, as additional factors in our case, that seizures significantly increase the likelihood of psychosis occurring, in the same way as neurobiological sensitisation due to prolonged consumption of psychoactive substances, which conditions modifications in the sensitivity of the dopamine and glutamate receptors.13
Although our patient did not meet the criteria for a major depressive episode during his delusional symptoms, his mood deterioration was palpable. In this context, psychomotor phenomena and changes in consciousness emerged, diagnosed as dissociative seizures, because of the clinical presentation and also because the electroencephalogram ruled out an epileptogenic focus. On the subject of the patient's Othello syndrome, it should be noted that in the works of Shakespeare there are 18 instances of fainting due to strong emotions, several consistent with vasovagal syncope, and even with myoclonic shocks that could be confused with epilepsy14; our patient's psychopathic personality and cerebral organicity made him more prone to the emergence of these conversive phenomena. Dissociative seizures, also called non-epileptic psychogenic seizures, while classified as a diagnosis per se (F44.5; ICD-10), are symptoms that commonly emerge as an expression of an underlying psychic conflict: the existence of frank epileptic seizures does not exclude the coexistence of dissociative seizures.15 Among the factors associated with this phenomenon are a history of serious mistreatment in childhood, depression, alcoholism, personality disorders and even brain disease, more specifically in the right hemisphere, and a history of neurosurgery, all of which were presented by our patient.16 There is no psychopharmacological or psychotherapeutic standard for the treatment of dissociative seizures: medication is beneficial to the extent that it treats comorbid psychiatric conditions.17 It cannot be asserted that the prescribed medication was the direct cause of the disappearance of dissociative seizures in our case; perhaps the separation of the couple, causing our patient's jealous conflict to abate, did away with the need for these psychogenic seizures as a defence mechanism.
The diagnosis of tuberculoma is based on pathological identification by biopsy; however, craniotomy and direct excision of the lesion are indicated when there is an increase in intracranial pressure, as in our patient.7 Although it was relatively brief, the follow-up of the case showed no reactivation of the TB.
Although our patient did not actually carry out suicidal or homicidal behaviour, as a product of his delusional jealousy, he did perpetrate verbal threats, harassing behaviour (stalking) and threats of physical violence against his partner; his family nucleus also abruptly dissolved: in the end, without treatment, he could have become far more dangerous. However, despite the psychopathological severity of delusional jealousy, the serious attacks it leads to are minimal compared to the psychopathic risk of gender violence. In Peru, the lifetime prevalence of physical or sexual violence against women is 36%, a figure similar to that of Colombia.18 In Lima, the last metropolitan mental health study showed a lifetime prevalence of any type of abuse of 54.7%, a high but hopefully lower rate than the figure from 10 years ago (65.8%).19 Our case, in which organic tubercular disease and jealous and violent behaviour are combined, both of which are problems of enormous importance in the public health of the country and Latin America, is a peculiar association of two complex situations that intersect in multiple spheres. This is the first published case of Othello syndrome secondary to cerebral tuberculoma.
Conflicts of interestThe authors have no conflicts of interest to declare.
To the psychiatrist Adelguisa Mormontoy, from the Hospital Cayetano Heredia, for providing us with clinical information.
Please cite this article as: Strobbe-Barbat M, Macedo-Orrego LE, Cruzado L. Síndrome de Otelo secundario a tuberculoma cerebral: a propósito de un caso. Rev Colomb Psiquiatr. 2020;49:115–119.
