





Despite the numerous benefits of core muscle strengthening in improving symptoms of fibromyalgia (FM), limited studies have quantified core muscle function in FM patients.
ObjectiveTo compare the core muscle endurance of FM females with age-matched healthy females and determine whether a correlation exists between core muscle endurance and FM severity.
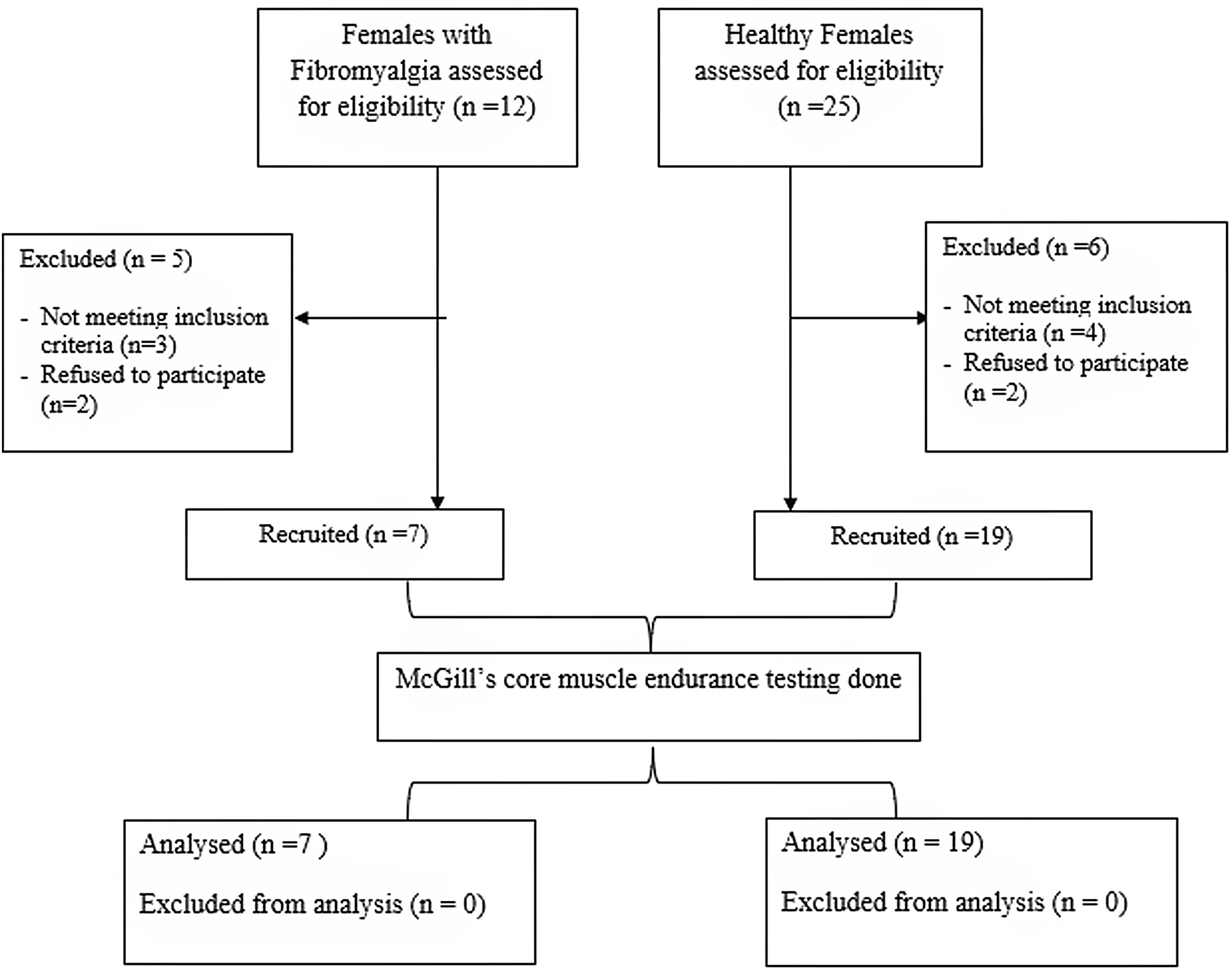
Materials and methodsPre-diagnosed female FM patients (n=7) and age-matched healthy females (n=19) were assessed using McGill's core endurance tests in four positions – flexion, extension, and bilateral side-bridge. The longest contraction holding time (in seconds) in each position was noted and compared in both groups. Additionally, patient-reported Fibromyalgia Impact Questionnaire (FIQ) scores were obtained to determine disease severity.
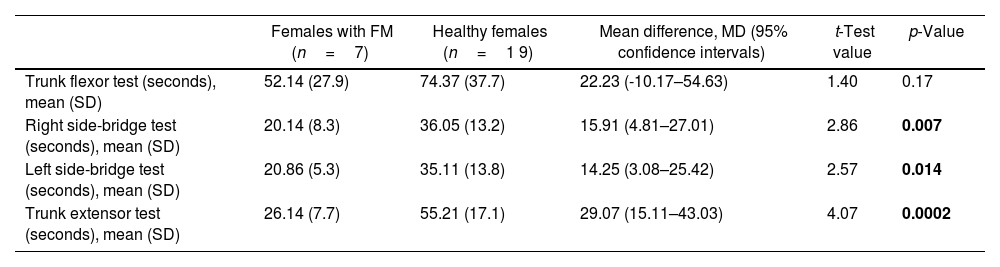
ResultsThe mean holding time for trunk extensors (26.14±7.7s), right lateral flexors (20.14±8.3s), and left lateral flexors (20.86±5.3s) was significantly lower in the FM females than the healthy females (trunk extensors=55.21±17.1s; right lateral flexors=36.05±13.2s; left lateral flexors=35.11±13.8s). The endurance of trunk flexors was statistically similar in both groups (FM females=52.14±27.9s; healthy females=74.37±37.7s). Lastly, core muscle endurance was not correlated with the FIQ scores in FM patients (p>0.05).
ConclusionThe results of this preliminary study revealed that core extensor and lateral flexor endurance in FM females was lower than their healthy female counterparts. Larger sample studies are needed to further substantiate our findings.
A pesar de los numerosos beneficios del fortalecimiento de los músculos centrales para mejorar los síntomas de la fibromialgia (FM), investigaciones limitadas han cuantificado la función de estos en pacientes con FM.
ObjetivoComparar la resistencia de los músculos centrales de mujeres con FM con mujeres sanas de la misma edad y determinar si existe una correlación entre la resistencia de los músculos centrales y la gravedad de la FM.
Materiales y métodosSe evaluaron pacientes femeninas con FM prediagnosticadas (n=7) y mujeres sanas de la misma edad (n=19), para lo cual se utilizaron las pruebas de resistencia central de McGill en cuatro posiciones: flexión, extensión y puente lateral bilateral. Se anotó el tiempo de mantenimiento de la contracción más largo (en segundos) en cada posición y se comparó en ambos grupos. Además, se obtuvieron las puntuaciones del Cuestionario de Impacto de la Fibromialgia (FIQ) informado por el paciente para determinar la gravedad de la enfermedad.
ResultadosEl tiempo medio de retención para los extensores del tronco (26,14±7,7 s), flexores laterales derechos (20,14±8,3 s) y flexores laterales izquierdos (20,86±5,3 s) fue significativamente menor en las mujeres FM que en las sanas (extensores de tronco=55,21±17,1 s, flexores laterales derechos=36,05±13,2 s y flexores laterales izquierdos=35,11±13,8 s). La resistencia de los flexores del tronco fue estadísticamente similar en ambos grupos (mujeres FM=52,14±27,9 s; mujeres sanas=74,37±37,7 s). Por último, la resistencia muscular central no se correlacionó con las puntuaciones FIQ en las pacientes con FM (p>0,05).
ConclusiónLos resultados de este estudio preliminar revelaron que la resistencia de los extensores centrales y flexores laterales en las mujeres con FM fue menor que en sus contrapartes sanas. Se necesitan estudios con muestras más grandes para corroborar aún más nuestros hallazgos.
Artículo
Comprando el artículo el PDF del mismo podrá ser descargado
Precio 19,34 €
Comprar ahora
