





Videocapillaroscopy is a diagnostic procedure that allows an assessment of the microcirculation in the nailfold of patients with Raynaud's phenomenon. There are few reports of videocapillaroscopic findings in healthy subjects, none in Colombia. It is important to know the findings that exist in the Colombian healthy population to have a reference and define abnormalities in people with diseases.
ObjectiveOur aim was to describe the standardized qualitative, quantitative videocapillaroscopic findings and the sociodemographic characteristics in healthy volunteers from a Colombian population.
Materials and methodsA cross-sectional descriptive study was conducted at the Simon Bolívar and Hospital Universitario Nacional de Colombia in Bogota, Colombia. Healthy adult volunteers over 18 years of age were included in the study. Two images were taken per finger from the second to fifth of each hand. A pilot test was conducted to refine the procedure and establish the agreement between the evaluators of the test, in which a kappa concordance index was estimated for the findings of capillary density, presence of dilated capillaries, megacapillaries, abnormal morphologies and avascular areas. Subsequently, measurements of the venous loop, arterial loop, apical portion, intercapillary distance, capillary density, presence of dilated capillaries, megacapillaries, avascular zones, and description of capillary morphology were performed. Finally, a capillaroscopic diagnosis was issued by Fast-track flowchart.
ResultsOne hundred one videocapillaroscopy studies were performed. The age range of the participants was 20–62 years (average 31 years). 59 women and 42 men. A total of 1611 photographs at 200× were analyzed. Agreement between the two observers was excellent for capillary density, dilated capillaries, microhemorrhages and abnormal shapes. The average of each the findings was as follows: capillary density of 8.2capillaries/mm, apical diameter 14.1μm, arterial loop 10.8μm, venous loop 13.7μm, and intercapillary distance 147μm. Morphology was evaluated in 10,855 capillaries. The predominant morphology was hairpin with 58.8%, followed by crossed 30.2% tortuous 10.4%, and abnormal forms corresponded to 0.48% of the sample. No avascular or megacapillary zones were documented. In 53 individuals, there were some dilated capillaries (182), corresponding to 1.7% of the capillaries analyzed (median of apical diameter: 23.3μm). Microhemorrhages was found in 16 volunteers, most of them hemosiderin content. The capillaroscopic diagnosis using the Fast-Track algorithm and standardization criteria were category I (a non-scleroderma pattern) in the entire sample, non-specific abnormal findings were observed in 67 (66.3%) of the 101 videocapillaroscopy analyzes.
ConclusionsIn healthy people of our cohort, the most frequent finding was nonspecific isolated abnormalities, but do not conform a scleroderma pattern when Fast-Track algorithm and standardization criteria are applied. In addition to ectasias up to 36μm, microhemorrhages with or without hemosiderin, rare abnormal and decreased capillary densities. Avascular or megacapillary zones were uncommon observed in these healthy subjects.
La videocapilaroscopia es un procedimiento diagnóstico que permite evaluar la microcirculación en el pliegue ungular de pacientes con fenómeno de Raynaud. Existen pocos reportes de hallazgos videocapilaroscópicos en sujetos sanos, ninguno en Colombia. Es importante conocer los hallazgos que existen en la población sana colombiana para tener un referente y definir anormalidades en personas con enfermedades.
ObjetivoNuestro objetivo fue describir los hallazgos estandarizados videocapilaroscópicos cualitativos y cuantitativos, así como las características sociodemográficas en voluntarios sanos de una población colombiana.
Materiales y métodosSe realizó un estudio descriptivo transversal en el Hospital Simón Bolívar y el Hospital Universitario Nacional de Colombia en Bogotá, Colombia. En el estudio se incluyeron voluntarios adultos sanos mayores de 18 años. Se tomaron dos imágenes por dedo, desde el segundo al quinto de cada mano. Se realizó una prueba piloto para afinar el procedimiento y establecer la concordancia entre los evaluadores de la prueba, en la que se estimó un índice de concordancia Kappa para los hallazgos de densidad capilar, presencia de capilares dilatados, megacapilares, morfologías anormales y áreas avasculares. Posteriormente, se hicieron mediciones del asa venosa, asa arterial, porción apical, distancia intercapilar, densidad capilar, presencia de capilares dilatados, megacapilares, zonas avasculares y descripción de la morfología capilar. Finalmente, se emitió un diagnóstico capilaroscópico mediante diagrama de flujo fast-track.
ResultadosSe llevaron a cabo 101 estudios de videocapilaroscopia. El rango de edad de los participantes fue de 20 a 62 años (promedio 31 años), 59 mujeres y 42 hombres. Se analizaron un total de 1.611 fotografías a 200x. La concordancia entre los dos observadores fue excelente para la densidad capilar, los capilares dilatados, las microhemorragias y las formas anormales. El promedio de cada uno de los hallazgos fue el siguiente: densidad capilar de 8,2 capilares/mm, diámetro apical de 14,1μm, asa arterial de 10,8μm, asa venosa de 13,7μm y distancia intercapilar de 147μm. Se evaluó la morfología en 10.855 capilares. La morfología predominante fue en horquilla con un 58,8%, seguida de cruzada con un 30,2%, tortuosa con un 10,4%, y las formas anormales correspondieron al 0,48% de la muestra. No se documentaron zonas avasculares o megacapilares. En 53 individuos hubo algunos capilares dilatados (182), correspondientes al 1,7% de los capilares analizados (mediana del diámetro apical: 23,3μm). Se encontraron microhemorragias en 16 voluntarios, la mayoría con contenido de hemosiderina. El diagnóstico capilaroscópico mediante el algoritmo fast-track y los criterios de estandarización fueron categoría I (patrón no esclerodérmico) en toda la muestra, se observaron hallazgos anormales inespecíficos en 67 (66,3%) de los 101 análisis de videocapilaroscopia.
ConclusionesEn personas sanas de la cohorte, el hallazgo más frecuente fueron las anomalías aisladas no específicas, pero sin conformar un patrón de esclerodermia al aplicar el algoritmo fast-track y los criterios de estandarización. Además, se observaron ectasias de hasta 36μm, microhemorragias con o sin hemosiderina, densidades capilares anormales y formas anormales escasas. Las zonas avasculares o megacapilares fueron poco frecuentes en estos sujetos sanos.
Videocapillaroscopy is a non-invasive, safe, and available diagnostic procedure that is useful in the assessment of microcirculation in the nail capillary fold of patients with rheumatic diseases. It allows measurements of capillary dimensions, determination of capillary density per millimeter, classification of capillary morphology, establishing the presence of microhemorrhages, and avascular areas to issue a final diagnosis.1 Its main indication is the assessment of Raynaud's phenomenon, allowing its division into primary or secondary etiology.2 It is also a prognostic factor given that the presence of dilated capillaries, microhemorrhages, and a decrease in the number of capillaries is associated with a greater risk of progression from primary Raynaud's phenomenon to Systemic Sclerosis3; that is the reason, since 2013, capillaroscopy has been part of the classification criteria for Systemic Sclerosis.4 However, these findings, considered abnormal, have also been described in people without disease.5–11
Recently, new definitions and flowcharts have been proposed in order to standardize the interpretation of videocapillaroscopy.2,12 The descriptions of findings in healthy subjects were performed with different instruments, magnifications, and terminology,5–11 so these works predate these standardization proposals. Likewise, in our population there are no previous descriptions; therefore, it was considered important to develop a study using a USB capillaroscope and the definitions proposed by the EULAR group (European Alliance of Associations for Rheumatology) for the study of microcirculation in rheumatic diseases.2,12
The final objective of our study was to determine the findings in videocapillaroscopy in a group of healthy people from the city of Bogota, Colombia with standardization criteria.
Materials and methodsA cross-sectional study was developed in volunteers without any disease over 18 years of age after completing the informed consent, the project was approved by the ethics committees of Subred Norte de Servicios de salud and National University Hospital of Colombia in Bogota, Colombia This study followed the regulations of the Declaration of Helsinki and resolution 8430 of 1993 of the Colombian Ministry of Health. The necessary sample size was calculated based on the cited studies,5–11 where a frequency of findings of 27% was observed and with an expected alternative difference of 12%, with a significance level of 5%, a power of 80%, and a two-tailed test. The calculated sample size was 96 individuals, even so, the study was planned to be carried out in at least 100 healthy subjects, estimating losses in data collection and processing.
Participants were recruited consecutively in outpatient consultation services. They were mainly workers, accompanying patients, and students who attended the hospitals. People with Raynaud's phenomenon, any disease, use of medications with potential alteration of microcirculation, and reports of recent traumatic lesions of the nailfold were excluded. Healthy status was determined by the investigators through questioning and a brief preliminary examination. Information was collected on hobbies with possible disruption of microcirculation due to unintentional trauma. Before carrying out the test, it was verified that there was no report of manicure three weeks prior or consumption of caffeine or tobacco 2h before the exam. Additionally, patients were acclimatized to the environment where the study was conducted.
Videocapillaroscopy was performed on each participant with DinoLite® AF4115ZT device, which was manufactured by Dunwell Tech Inc at a magnification of 200×, calibrated according to the manufacturer's recommendation. To perform the capillaroscopy, 16 images were taken in each healthy volunteer, 2 images per finger and 8 fingers (except the thumbs). In each nail, two adjacent 1mm images were taken in the middle of the nail fold. This technique was based on the capillaroscopic technique, considered the gold standard.2,3 The images obtained were stored in the DinoCapture® 2.0 software, encoding the data of the participants and the information obtained was entered into the REDCap platform for its storage and security. Each person was evaluated for capillary density, capillary morphology, presence of microhemorrhages, dilations, megacapillaries, and avascular areas; as well as the diameters of the arterial and venous loop, apical diameter, internal diameter, and intercapillary distance.
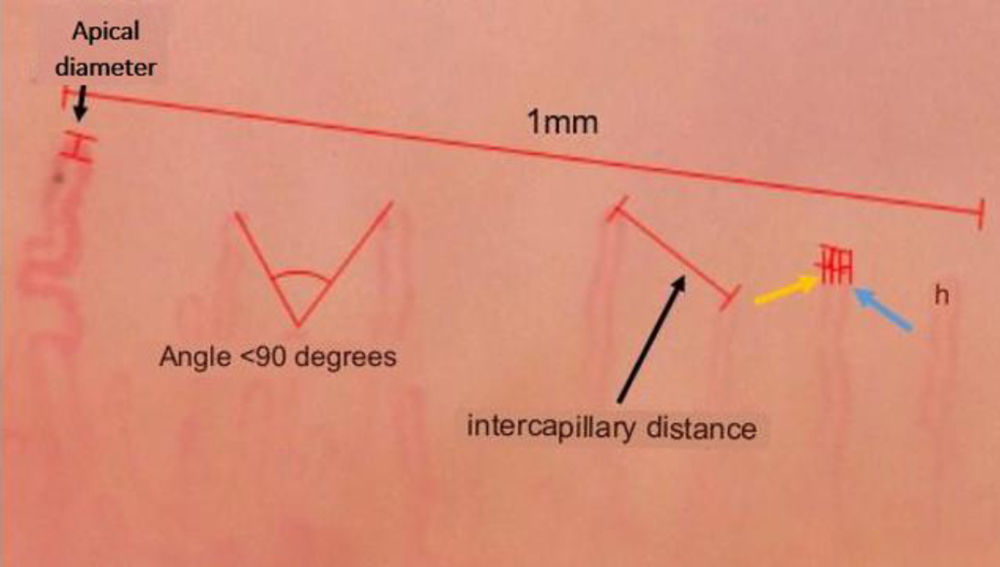
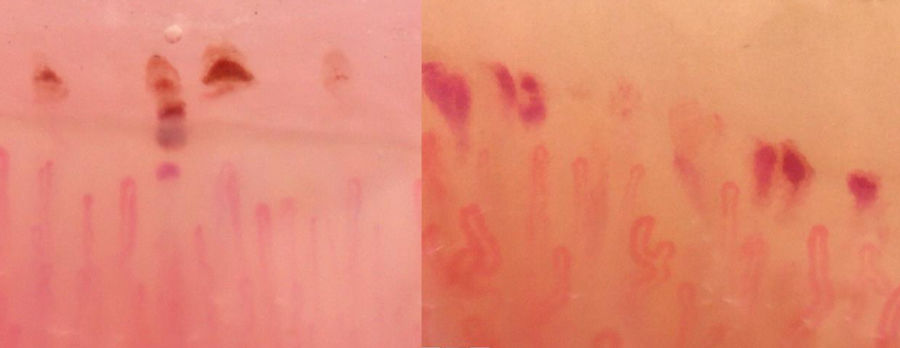
Microhemorrhages were divided into Microhemorrhages with and without hemosiderin. This classification is due to the fact that there is a differential description in the literature. Hemorrhages with hemosiderin were considered those that were hyperpigmented, and hemorrhages without hemosiderin were those that did not present hyperpigmentation (see Fig. 7). Measurements were conducted on a 1mm linear scale of each image (see Figs. 1 and 2). For each person, the images were analyzed quantitatively and semiquantitative.
, intercapillary distance, arterial loop (yellow arrow), venous loop (blue arrow), internal diameter (between the venous and arterial loop).")
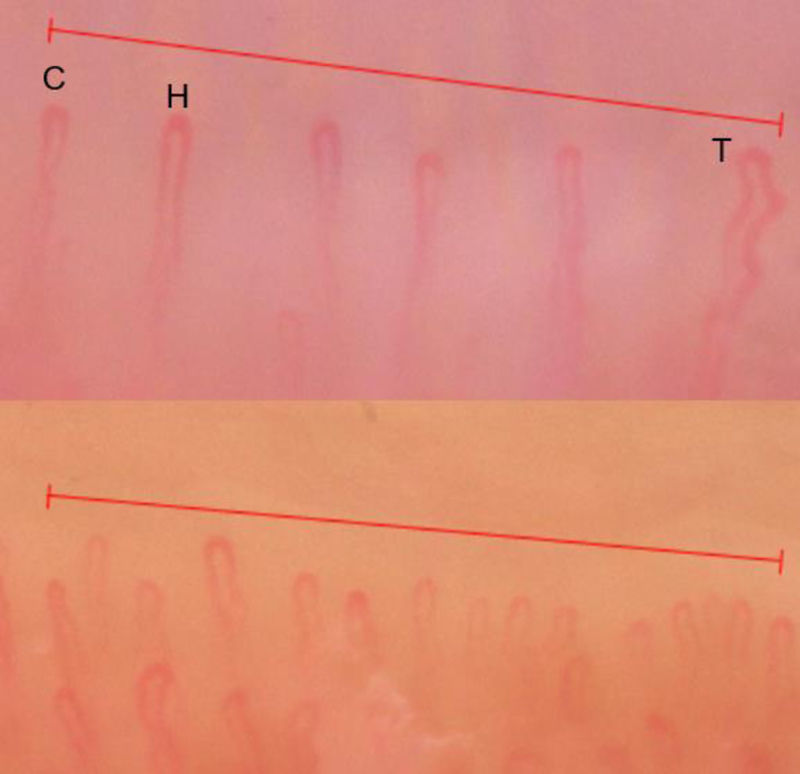
, crossed (C), and tortuous (T). In the lower part, a density of 12capillaries/mm is observed.")
A pilot study was developed in 20 persons that contribute to reducing possible biases and errors in obtaining the data that can guide to improve the previously proposed methodology. Also, capillary density, presence of dilated capillaries, megacapillaries, avascular areas and abnormal morphologies were explored to search for concordance between the two researchers (YM and HC), one certified with 4 years of experience and another beginner, using Cohen's kappa test with their respective confidence intervals The concordance results obtained were classified according to Landis and Koch scale as follows: 0 disagreement, 0–0.20 weak, 0.21–0.40 slight, 0.41–0.61 moderate, 0.61–0.80 high, 0.81–1.0 excellent.13
Capillaroscopic diagnosis and normal parameters were established using the Fast-Track flowchart and the standardization definitions of Smith et al. endorsed by standardization parameters suggested by the group of the EULAR Study of Microcirculation in Rheumatic Diseases.2,12 The results were classified into two diagnostic categories: 1. Non-scleroderma pattern, which were divided into A. Normal and B. Non-specific changes; 2. Scleroderma pattern. Inferential analyzes were performed considering gender, hobbies, and active smoking status. For the preparation of this study, the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) recommendations were followed.14
An exploratory data analysis was performed to identify the performance of the variables. For continuous variables, the mean, median, standard deviation, interquartile range, Spearman correlations, and Kolmogorov–Smirnov normality tests are described. For categorical variables, frequency tables were elaborated. Statistical tests based on inferential methods such as the comparison of means test for independent samples under the assumption of normality were performed, as well as non-parametric tests of U Mann de Whitney for variables that do not comply with the assumption of normality. Finally, a binary logistic regression model was applied taking capillaroscopic categorical variables as dependent variables and other variables (sex, occupation, hobbies, smoking) as independent variables. It was adjusted for each of the independent variables described.
ResultsOne hundred ten healthy volunteers and 1616 images were included and it was not possible to analyze 9 persons due to difficulty in assessing the images. Therefore, the data of 101 participants and 1611 photographs were analyzed. Thirty-nine participants were from the National University Hospital and 62 from the Simon Bolívar Hospital. Fifty-nine (54%) were women and 42 (46%) men, aged from 20 to 62 years (median 28, IQR 10). Demographic characteristics of the subjects can be seen in Table 1.
Demographic characteristics of the subjects.
| Type | n (%)101 (100) |
|---|---|
| Sex | Women: 59 (54%)Men: 42 (46%) |
| Age | From 20 to 62 years (median: 28)Women: median 28 yearsMen: median 28.5 years |
| Occupation | Health workers: 61 (55%)Students: 23 (21%)Others: 17 (24%) |
| Active smoking | 7 (6.9%) |
| Hobbies | 62 (61.3%) participants reported a hobby (sports, crafts, cooking) |
In the concordance test: the interobserver kappa index for the variables was excellent as follows: capillary density: 0.83 (95% CI, 0.67–0.98), dilated capillaries 0.85 (95% CI, 0.69–1), abnormal morphologies 0.91 (95% CI, 0.75–1), microhemorrhages 1.00 (95% CI, 0.84–1). For avascular areas and megacapillaries, we found an excellent observed concordance of 1.00.
Results of quantitative measurementsCapillary density of the population was on average 8.2capillaries/mm (standard deviation; –SD– 0.78), the image with the lowest number of capillaries had 4 per mm and the one with the highest number of capillaries had 14 per mm. The lowest capillary density observed in a person was on average 6 capillaries per mm and the highest density observed was on average 11 capillaries per mm (see Figs. 1 and 2; and Table 2). The results of the density measurements of apical diameter arterial loop diameter, venous loop diameter, internal diameter and intercapilar distance can be seen in Table 2.
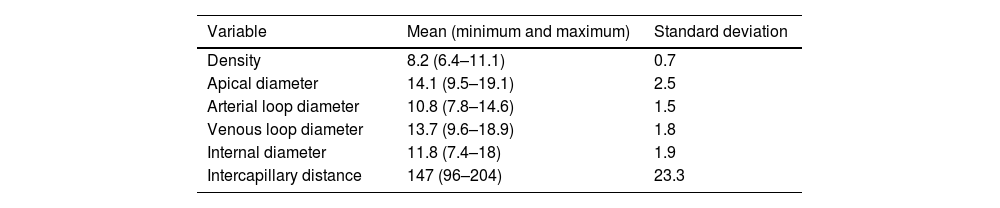
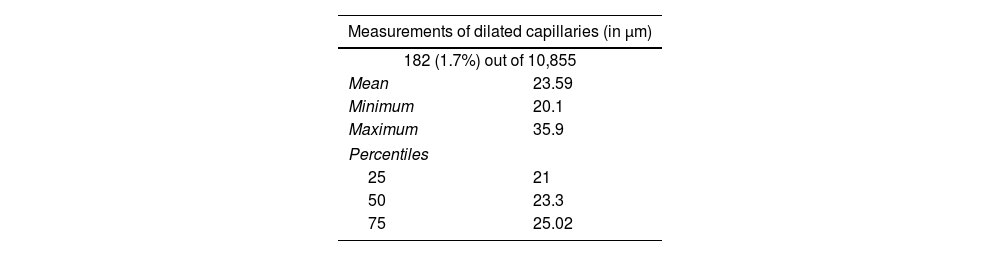
Summary of the measurements performed in capillaries (dilated capillaries can be seen in Table 3).
| Variable | Mean (minimum and maximum) | Standard deviation |
|---|---|---|
| Density | 8.2 (6.4–11.1) | 0.7 |
| Apical diameter | 14.1 (9.5–19.1) | 2.5 |
| Arterial loop diameter | 10.8 (7.8–14.6) | 1.5 |
| Venous loop diameter | 13.7 (9.6–18.9) | 1.8 |
| Internal diameter | 11.8 (7.4–18) | 1.9 |
| Intercapillary distance | 147 (96–204) | 23.3 |
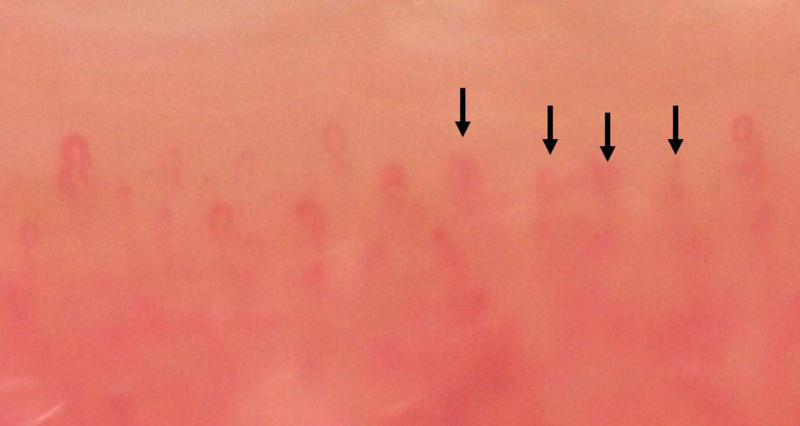
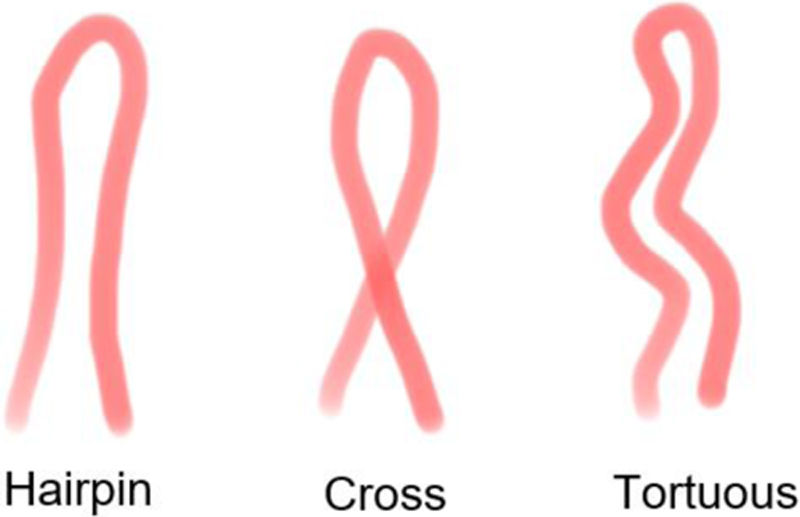
The morphology was analyzed in 10,855 capillaries from a total of 13,224, since in 2369 capillaries it was not possible to developed assessments due to visualization limitations (see Fig. 3). 10,802 (99.5%) evaluable capillaries were normal, hairpin shape was the most observed in 6391 (58.8%), followed by crossed in 3279 (30.2%), and tortuous in 1132 (10.4%). The capillaries with abnormal shapes presented mostly with bifurcations (see Fig. 4) and corresponded to 53 (0.48%) of the capillaries analyzed (see Fig. 5).
.")


Morphologies defined as normal and any different morphology presented was considered abnormal according to classification of Smith et al.3 Images of our healthy volunteers.
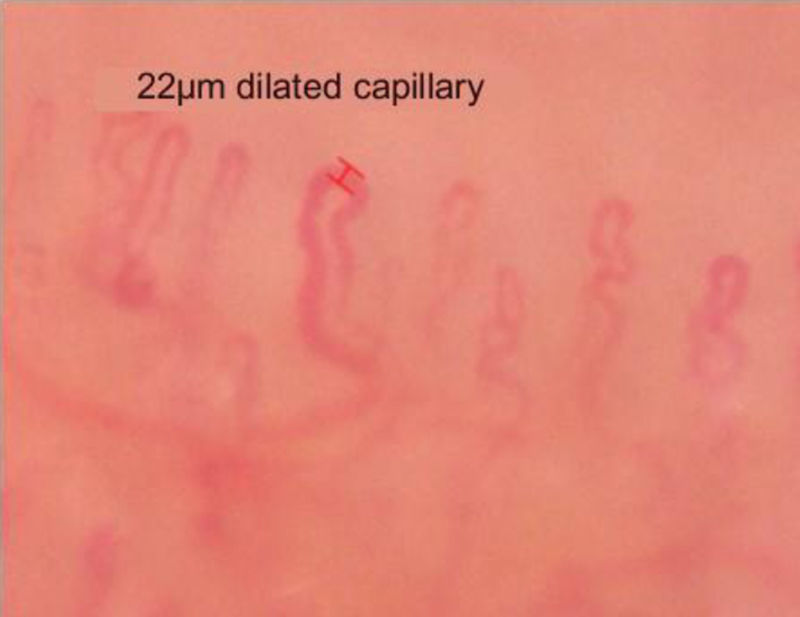
Ectasias or dilated capillaries were found in 53 (52.5%) of the participants. Of the total sample of capillaries, 182 (1.7%) were found to be dilated. The maximum number of dilated capillaries in the same videocapillaroscopy, that is, in the same patient, was 19 dilated capillaries. See Fig. 6 and Table 3.

Microhemorrhages were observed in 16 (15.96%) of the 101 volunteers. The maximum number of microhemorrhages in a patient was 13 and the minimum was 1. Microhemorrhages with hemosiderin were observed in 13 participants and microhemorrhages without hemosiderin were observed in 6 individuals (see Fig. 7). No avascular zones were documented.

The venous plexus was visible in 32% of the total fingers examined (in 33 of the participants). The 82% of these findings were registered in the 4th and 5th fingers.
Videocapillaroscopic diagnosisThe definitive videocapillaroscopic diagnosis was category I or a non-scleroderma pattern for all 101 participants. Normal findings were seen in 34 (33.6%) of them. Findings defined as non-specific were found in 67 (66.3%) participants, these changes were distributed as follows: decreased density in two (3%) of the participants, dilations in 53 (52.5%), microhemorrhages in 16 (15.8%), and abnormal morphologies in 33 (32.7%). A categorization was made on the semiquantitative scale (from zero to three according to: 0=absence of abnormality, 1=<33% of capillaries, 2=between 33% and 66% of capillaries and 3=>66% of capillaries) and it was observed that all findings corresponded to category 1, that is, non-specific changes. No avascular or megacapillary zones were observed in the sample.
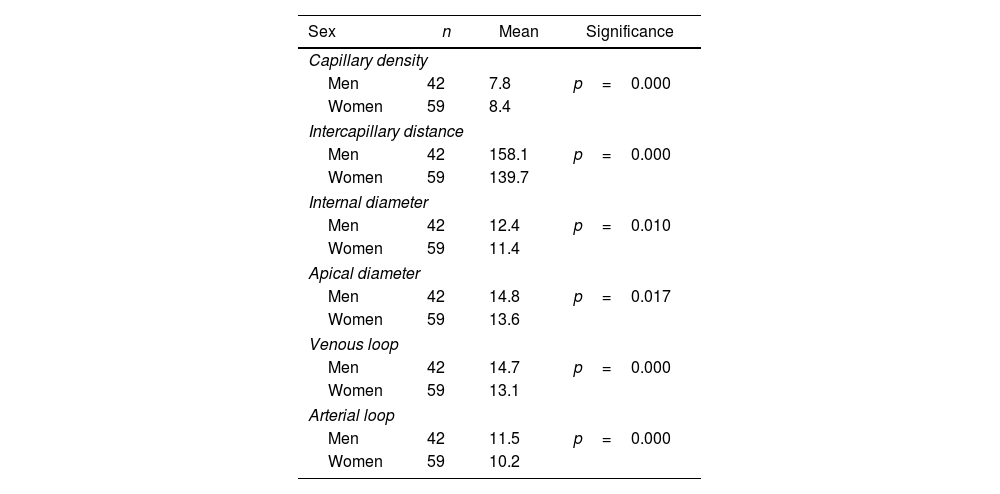
Other capillaroscopic findingsIn analysis of association by sex, smoking and hobbies with impaired microcirculation, we found greater capillary density in women, and greater Intercapillary distance, greater diameter of the venous loop, arterial loops, and apical diameter in men. Also, more abnormal forms were found in men than in women (p=0.008), as well as a greater number of dilated capillaries (p=0.001) (see Table 4).
Analysis of the measurements according to sex.
| Sex | n | Mean | Significance |
|---|---|---|---|
| Capillary density | |||
| Men | 42 | 7.8 | p=0.000 |
| Women | 59 | 8.4 | |
| Intercapillary distance | |||
| Men | 42 | 158.1 | p=0.000 |
| Women | 59 | 139.7 | |
| Internal diameter | |||
| Men | 42 | 12.4 | p=0.010 |
| Women | 59 | 11.4 | |
| Apical diameter | |||
| Men | 42 | 14.8 | p=0.017 |
| Women | 59 | 13.6 | |
| Venous loop | |||
| Men | 42 | 14.7 | p=0.000 |
| Women | 59 | 13.1 | |
| Arterial loop | |||
| Men | 42 | 11.5 | p=0.000 |
| Women | 59 | 10.2 | |
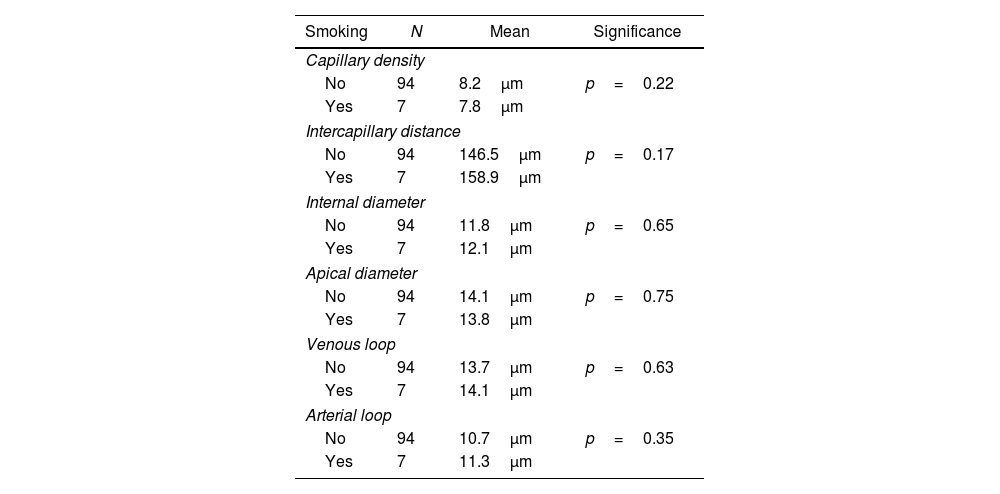
Regarding smoking, 7 (6.9%) volunteers smoked (5 men and 2 women) and 94 (93.1%) did not. There was a tendency to observe a lower capillary density in smokers without statistically significance (see Table 5). There were also no differences according to hobby, adjusting for the other variables. When performing logistic regression to analyze the relationship of the dichotomous dependent variable called dilation, with the independent variables: occupation, hobby, smoking, age and sex. Sex was significant, adjusting the model removing variables without changing the result.
Analysis of the measurements according to smokers and non-smokers.
| Smoking | N | Mean | Significance |
|---|---|---|---|
| Capillary density | |||
| No | 94 | 8.2μm | p=0.22 |
| Yes | 7 | 7.8μm | |
| Intercapillary distance | |||
| No | 94 | 146.5μm | p=0.17 |
| Yes | 7 | 158.9μm | |
| Internal diameter | |||
| No | 94 | 11.8μm | p=0.65 |
| Yes | 7 | 12.1μm | |
| Apical diameter | |||
| No | 94 | 14.1μm | p=0.75 |
| Yes | 7 | 13.8μm | |
| Venous loop | |||
| No | 94 | 13.7μm | p=0.63 |
| Yes | 7 | 14.1μm | |
| Arterial loop | |||
| No | 94 | 10.7μm | p=0.35 |
| Yes | 7 | 11.3μm | |
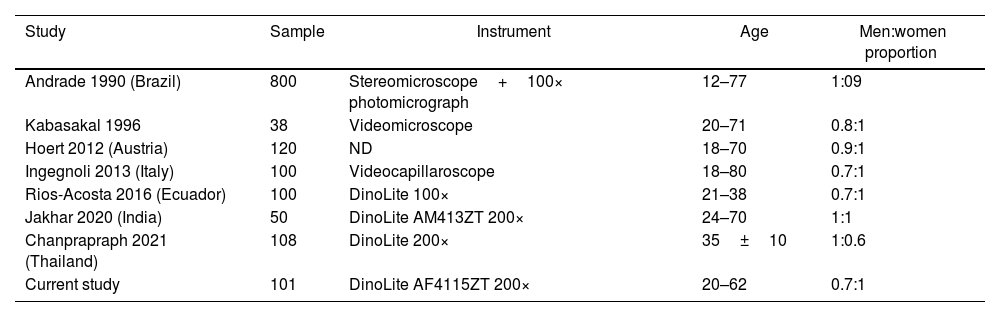
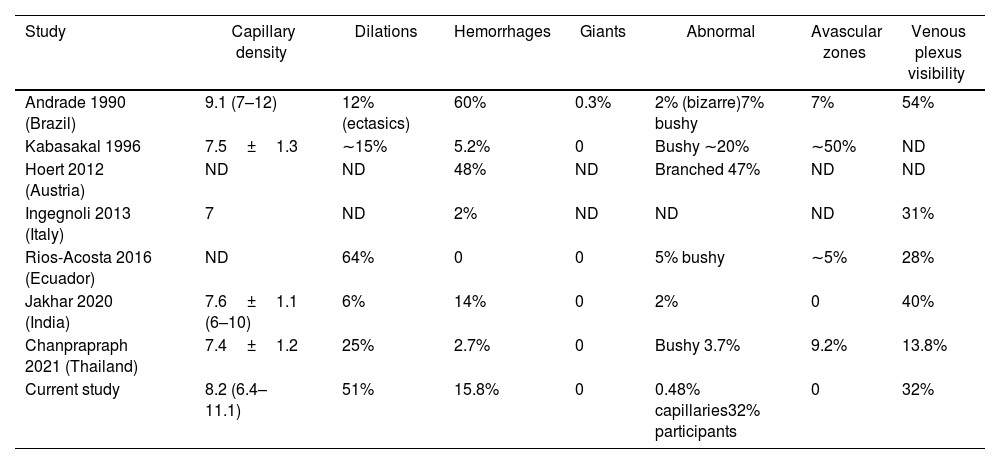
The present study describes changes in the videocapillaroscopy of healthy volunteers recruited in two hospitals in Bogotá, Colombia; and is the first study of its kind developed in Colombia up to our knowledge. We used the EULAR group nomenclature and a USB device that has been used in other studies and that is on the list of recommended devices to assess microcirculation.2 As far as we know, this is the first study of its type conducted in Colombia. We found a capillary density of 8capillaries/mm and we described so-called non-specific abnormalities in a significant number of people (63%). These abnormalities were generally isolated and reported on the semiquantitative scale as category 1 (less than 33% of the total capillaries evaluated). The visibility of the venous plexus was 32%, higher in fingers 4 and 5. Our study is in line with what was previously reported by other researchers (see Tables 6 and 7),5–11 with a capillary density greater than 7capillaries/mm, in addition to nonspecific findings such as dilations, microhemorrhages, and less frequent findings such as abnormal capillary shapes and reduced density. Ectasias observed were mostly less than 30μm, which is the threshold that has been associated with the future development of systemic sclerosis in patients with primary Raynaud's and a capillary diameter greater than 30μm.15
Comparison of capillaroscopy studies in a healthy population in terms of population variables and measurements.
| Study | Sample | Instrument | Age | Men:women proportion |
|---|---|---|---|---|
| Andrade 1990 (Brazil) | 800 | Stereomicroscope+100× photomicrograph | 12–77 | 1:09 |
| Kabasakal 1996 | 38 | Videomicroscope | 20–71 | 0.8:1 |
| Hoert 2012 (Austria) | 120 | ND | 18–70 | 0.9:1 |
| Ingegnoli 2013 (Italy) | 100 | Videocapillaroscope | 18–80 | 0.7:1 |
| Rios-Acosta 2016 (Ecuador) | 100 | DinoLite 100× | 21–38 | 0.7:1 |
| Jakhar 2020 (India) | 50 | DinoLite AM413ZT 200× | 24–70 | 1:1 |
| Chanprapraph 2021 (Thailand) | 108 | DinoLite 200× | 35±10 | 1:0.6 |
| Current study | 101 | DinoLite AF4115ZT 200× | 20–62 | 0.7:1 |
Comparison of several capillaroscopy studies in healthy subjects (main results).
| Study | Capillary density | Dilations | Hemorrhages | Giants | Abnormal | Avascular zones | Venous plexus visibility |
|---|---|---|---|---|---|---|---|
| Andrade 1990 (Brazil) | 9.1 (7–12) | 12% (ectasics) | 60% | 0.3% | 2% (bizarre)7% bushy | 7% | 54% |
| Kabasakal 1996 | 7.5±1.3 | ∼15% | 5.2% | 0 | Bushy ∼20% | ∼50% | ND |
| Hoert 2012 (Austria) | ND | ND | 48% | ND | Branched 47% | ND | ND |
| Ingegnoli 2013 (Italy) | 7 | ND | 2% | ND | ND | ND | 31% |
| Rios-Acosta 2016 (Ecuador) | ND | 64% | 0 | 0 | 5% bushy | ∼5% | 28% |
| Jakhar 2020 (India) | 7.6±1.1 (6–10) | 6% | 14% | 0 | 2% | 0 | 40% |
| Chanprapraph 2021 (Thailand) | 7.4±1.2 | 25% | 2.7% | 0 | Bushy 3.7% | 9.2% | 13.8% |
| Current study | 8.2 (6.4–11.1) | 51% | 15.8% | 0 | 0.48% capillaries32% participants | 0 | 32% |
Descriptions in the universal literature on capillaroscopy in a healthy population are scarce. In 1990, Andrade reported the findings in 800 individuals using a 16× stereomicroscope with microphotographs that generated a final magnification of 100× and found morphological abnormalities in 34% of the sample and a few for each individual. Andrade also found 12% of dilations, 7% of ramifications, 2% of “rare” capillaries, 25% of tortuosities, and 0.3% of megacapillaries.5 Like Andrade et al., we found a higher capillary density in women than in men, although contrary to our study, they found more dilated capillaries in women than in men. Kabasal, in 1996, evaluated 38 healthy controls using a videomicroscope and found a density of 7.5capillaries/mm with microhemorrhages in 5.2%, branched capillaries in approximately 20%, dilations in 15%, avascular zones in 50%, and no megacapillaries.6 Hoerth found that only 18 individuals (15%) had no deviation in morphology, hemorrhages, or capillary density on any finger. Overall, 67% had morphological changes, 48% had microhemorrhages, and 40% of volunteers below 40 years of age and 18% above age 40 had less than 8capillaries/mm. Among morphological changes tortous (43%), ramified (47%), and bushy capillaries (27%) were the most frequently altered capillary types.7
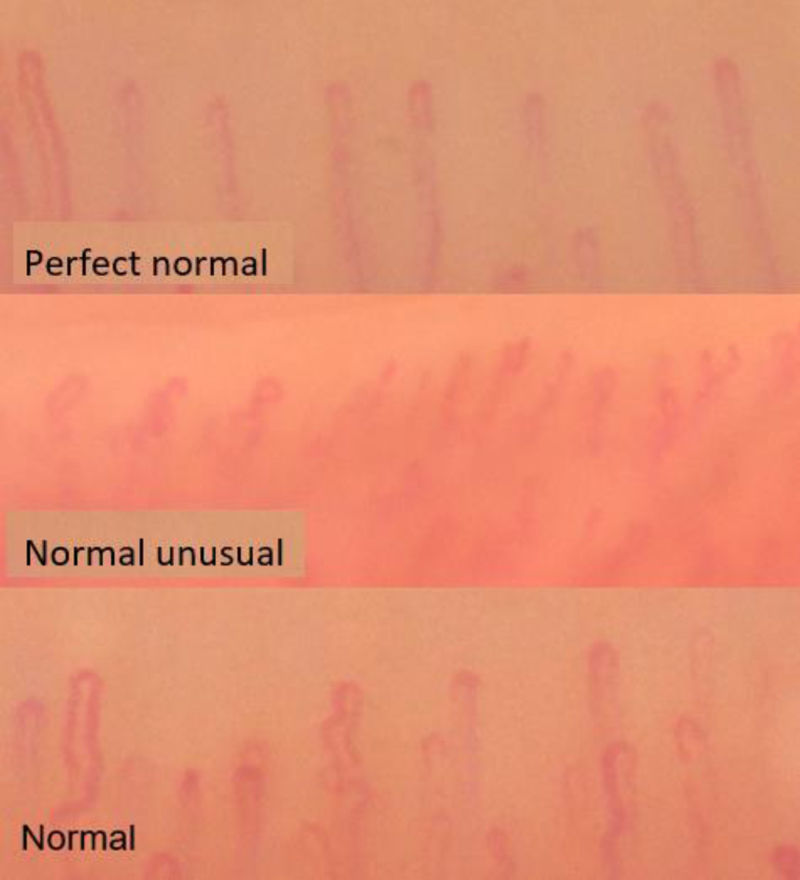
Ingegnoli et al. in 2013, using VideoCap® at 200×, described the findings in 100 subjects in 400 images and concluded that the average density was 7capillaries/mm. In addition, they proposed three normal patterns: one with a predominance of hairpin forms with a maximum of two tortuous or “normal” capillaries, another pattern with ≥5 hairpin capillaries/mm or “perfect normal” and a third pattern where there are branched, tortuous capillaries, with microhemorrhages or observing more than 4 crossed capillaries (“unusual normal” pattern). The frequency of dilations was not mentioned, although they described apical diameters of up to 106μm; that is, there would be the presence of giants (megacapillaries) in their sample, finding that is clearly pathologic.8 In our study, we found some tendency to that proposed by Ingeoli et al. (see Fig. 8), but without the pathological characteristics described.

Three studies reported USB videocapillaroscopies findings with DinoLite® devices. In a study by Rios-Acosta in Ecuador, that was performed at 100×, abnormalities were found in 86% of the 100 capillaroscopies, ectasias in 62%, crossed capillaries in 60%, tortuous capillaries in 59%, and avascular zones (defined as >500μm without capillaries) in ∼5% did not report capillary density.9 In a study in India, a sample of 50 volunteers with 200× magnification, it was described microhemorrhages in 14% of the participants, tortuous in 14%, dilations in 6%, ramifications in 4%, “rare” capillaries in the 2%;and there were no avascular areas.10 Chanprapaph in Thailand used 200× magnification and described the findings in 108 participants: a density of 7.4capillaries/mm, avascular areas (defined as loss of two or more capillaries) in 9.2%, microbleeds in 2.7%, visibility of the venous plexus in 13.8%, tortuous capillaries 13.7%. In 88.8% of people, there are no data on dilations.11 None of the previous studies described the presence of megacapillaries.9–11
Capillaroscopy studies have limitations, one of which is operator dependent. To improve reliability Smith et al. proposed a reading algorithm,2,12 where the reliability between evaluators to discern a “scleroderma pattern” of a “non-scleroderma pattern” was good to excellent among rheumatologists with different levels of training in capillaroscopy.12 In another study by the same authors, a classification of capillary morphology into normal and abnormal was proposed, finding a moderate correlation of the definitions used. It is noteworthy that novice evaluators distinguished normal from abnormal capillaries with a one-hour training session and good concordance.16 In our study, inter-observer agreement is near perfect, due in part to the use of pre-assessment definitions of images proposed by Smith and during various consensus meetings as demonstrated by Boulon et al.17
A unified way of reporting capillaroscopy findings was recently proposed in consensus meetings, which will allow direct comparisons between studies. Some of the previously reported abnormalities (for example, tortuous capillaries) are currently not considered alterations but rather variations from normality, and the consensus emphasizes three areas to consider: informing the patient's preparation, describing the device used, and details of the examination, such as density and other measurements. Our study follows the recommendations for analysis and reporting videocapillaroscopy findings.18,19
There are several devices that can be used in videocapillaroscopy and the necessary standard is equipment that allows a 200× magnification with image storage and processing capacity and that captures at least two adjacent images of one linear millimeter in 8 fingers.2 The device used and the technique in the present study meet these specifications. In addition, there are comparisons between USB capillaroscopes, stereomicroscopes, and digital video capillaroscopes that showed equal diagnostic performance.20,21
A limitation of our study is that a significant number of capillaries could not be classified due to visualization problems, despite this we are reporting it. However, we were able to take a sufficient number of images of the total sample to evaluate a significant number of capillaries. In general, the studies do not report the number of capillaries that are not classifiable due to poor visualization.
A strength of our study was the simple definitions and flowcharts that were based on the aforementioned standardization criteria.
ConclusionBased on our findings conducted in normal subjects, we conclude that nonspecific isolated abnormalities in healthy subjects are frequent but do not conform a scleroderma pattern when Fast-Track algorithm and standardization criteria are applied. In addition to ectasias up to 30μm and some infrequent up to 36μm, microhemorrhages with or without hemosiderin; and also, rare abnormal forms. In healthy people, avascular or megacapillary zones (giant capillaries) are not found, their presence is abnormal and indicates microcirculation pathology.
Ethical considerationsThis study was approved by the Ethics Committee of Subred Integrada Servicios de Salud Norte E.S.E, with the ID: SNCEI-146, and it was carried out under the International Guidelines for Biomedical Research in Humans, the Declaration of Helsinki, amendment 2008, the Colombian Law 29 of 1990 and Resolution 008430 of 1993. All participants signed informed consent upon entering the study.
FundingThis project was accomplished with funds allocated through a grant with financial support for research projects from the Colombian Association of Rheumatology.
Conflict of interestsNone.
