





To describe the clinical and epidemiological behavior of Dupuytren's contracture (DC) in the Colombian population, and to compare the results of this study with other series published in the literature.
Materials and methodsA descriptive, observational study of 33 cases of DC presented at the Hospital San Pedro y San Pablo, La Virginia Risaralda, over the last 6 years. The patients were diagnosed with DC according to the established parameter. The results were compared against different series of DC cases published in the literature.
ResultsThe mean age at diagnosis was 61.3 years, with a higher prevalence of men (64% of cases). The most frequent form of presentation was unilateral in the right hand (73%), unlike the reports from other series with usually bilateral involvement. Diabetes mellitus was the comorbidity most often associated with DC (24.24%), a finding similar to those of previous publications. Most patients required surgical treatment.
ConclusionsDC is a condition that occurs more often in men in the sixth or seventh decade of life. Diabetes mellitus is the most frequently associated disease, with no differences being found among the various studies. In the Colombian population there is no apparent association with epilepsy. The presentation of DC is variable, but our series showed more unilateral involvement as compared to other populations where the presentation is usually bilateral.
Describir el comportamiento clínico y epidemiológico de la contractura de Dupuytren (CD) en la población colombiana y comparar nuestros resultados con otras series publicadas en la literatura.
Materiales y métodosEstudio descriptivo observacional de 33 casos de CD presentados en el hospital San Pedro y San Pablo de la Virginia, Risaralda, durante los últimos 6 años. Los pacientes cumplieron con el diagnóstico de CD de acuerdo con el parámetro establecido. Se compararon los resultados con diferentes series de casos de CD publicadas en la literatura.
ResultadosLa edad promedio al momento del diagnóstico fue de 61,3 años con mayor prevalencia en hombres (64% de los casos). La forma de presentación más frecuente fue unilateral en mano derecha (73%), a diferencia de lo reportado en otras series, donde el compromiso usualmente fue bilateral. La diabetes mellitus fue la comorbilidad con mayor asociación a la CD (24,24%), hallazgo similar a lo publicado previamente. La mayoría de los pacientes requirió tratamiento quirúrgico.
ConclusionesLa CD es una entidad de mayor ocurrencia en hombres de la sexta a la séptima década de la vida. La diabetes mellitus es la enfermedad que más se asocia a su aparición, sin encontrase diferencias entre los estudios realizados. En población colombiana no hay relación aparente con epilepsia. La presentación de la CD es variable, encontrándose en nuestra serie un mayor compromiso unilateral a diferencia de otras poblaciones donde la presentación usualmente es bilateral.
The original descriptions of Cupuytren's Contracture (DC) date back to the 12th and 13th Centuries and include narratives of miraculous healings of the disease by a priest.1 In 1614, the Swiss doctor, Felix Plater made the first observations about the etiology of this phenomenon, attributing it to trauma.2 Later, Henry Cline, a renowned surgeon at that time, contributed with new information about DC and conducted some surgical procedures. However, it was not until 1831 that Guillaume Dupuytren, MD surgeon,3 formally described the disease and performed the first open fasciotomy.
DC is a fibroproliferative disorder involving the palmar aponeurosis and the fingers, causing a flexion contracture of the metacarpophalangeal and interphalangeal joints; the most frequently affected digits are the ring and little finger.4 The pathognomonic lesion of DC are nodules on the bands of the palmar aponeurosis which, as the disease progresses, develop into cords that cause continuous flexion of the digit involved. DC has a predilection for the right hand, which is affected in 60% of the cases.2
The prevalence of the disease is estimated between 2 and 42%, depending on the population evaluated.5
DC has been described in all ethnic groups, although the highest prevalence has been reported in Scotland, Iceland, Norway and Australia.6 Although the etiology of the disease is not clearly established, observational studies have identified several associations with metabolic diseases such as diabetes and hypothyroidism, trauma, alcohol use, cigarette smoking, and even epilepsy. Globally, DC is more frequent among males, though the prevalence varies with regards to age, with a higher occurrence among males between 40 and 60 years old, but this changes after 70 years of age, when the disease is more frequent among females.7
According to Luck, DC is classified into 4 evolutionary stages:
- 1)
The early stage where the pathognomonic lesion is a painless and insensitive nodule at the level of the distal palmar fold. There is thickening and modularity of the fascia, with a prevalence of Collagen type III.
- 2)
Active or proliferative phase: onset of contraction and the first sign is palpation of a cord proximal to the nodule. The skin attaches to the fascia and there is presence of collagen type III and IV, but with a prevalence of fibroblasts.
- 3)
Advanced or involution phase: the nodules disappear and the joint contracture develops at the level of the metacarpophalangeal and proximal interphalangeal joint, with hyperextension of the distal interphalangeal joint and the formation of firm cords and bands similar to a tendon.
- 4)
Residual phase: There are only retracted fibrous bands.8
This study discusses 33 cases of DC, comparing the behavior of the disease in our setting versus other populations. This article represents the largest case series ever published in Colombia on DC.
Materials and methodsObservational, descriptive study reviewing 33 cases of DC diagnosed in Virginia (Risaralda), between January 2010 and October 2016. A detailed review of the medical records was conducted, including all patients with a confirmed diagnosis of DC. Patients with an unclear diagnosis were excluded.
We conducted a review of DC cases published until 2016, using PUBMED and SCIELO search engines. Any articles including 5 or more patients were analyzed and compared against the Colombian series.
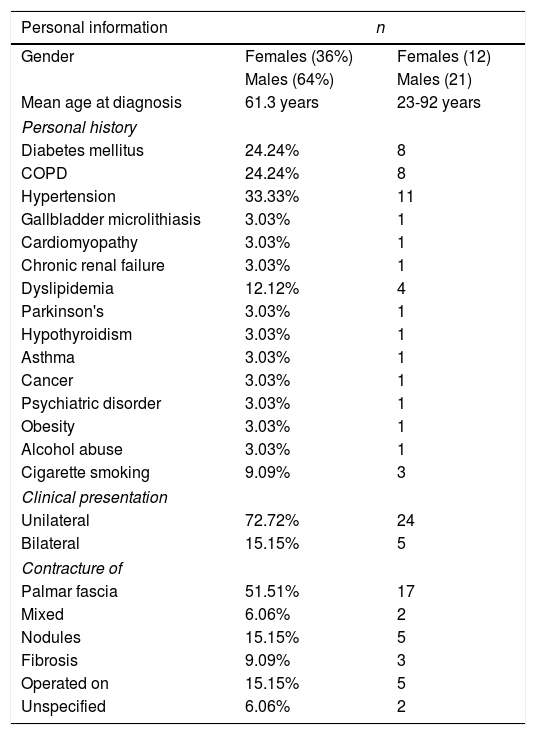
Results33 patients with DC were identified, mostly males (n=21). The mean age at the time of diagnosis was 61.3 years (range 23–92). The mode of presentation described in the medical record was fibrous nodules and bands (mixed) (n=2), contracture (n=17), nodules only (n=5), fibrosis only (n=3), unspecified in the medical record (n=2) and already operated on (n=5); most of them complained about swelling and functional limitation (Table 1).
General characteristics of the 33 patients with DC.
| Personal information | n | |
|---|---|---|
| Gender | Females (36%) | Females (12) |
| Males (64%) | Males (21) | |
| Mean age at diagnosis | 61.3 years | 23-92 years |
| Personal history | ||
| Diabetes mellitus | 24.24% | 8 |
| COPD | 24.24% | 8 |
| Hypertension | 33.33% | 11 |
| Gallbladder microlithiasis | 3.03% | 1 |
| Cardiomyopathy | 3.03% | 1 |
| Chronic renal failure | 3.03% | 1 |
| Dyslipidemia | 12.12% | 4 |
| Parkinson's | 3.03% | 1 |
| Hypothyroidism | 3.03% | 1 |
| Asthma | 3.03% | 1 |
| Cancer | 3.03% | 1 |
| Psychiatric disorder | 3.03% | 1 |
| Obesity | 3.03% | 1 |
| Alcohol abuse | 3.03% | 1 |
| Cigarette smoking | 9.09% | 3 |
| Clinical presentation | ||
| Unilateral | 72.72% | 24 |
| Bilateral | 15.15% | 5 |
| Contracture of | ||
| Palmar fascia | 51.51% | 17 |
| Mixed | 6.06% | 2 |
| Nodules | 15.15% | 5 |
| Fibrosis | 9.09% | 3 |
| Operated on | 15.15% | 5 |
| Unspecified | 6.06% | 2 |
The initial DC involvement was usually unilateral (72.7%), with a prevalence of the right hand (58.3% over the left hand (41.6%) The rest of the patients presented with a bilateral involvement.
In terms of comorbidities, there were 11 patients with high blood pressure which accounted for 33.3% of the cases; 8 patients had diabetes mellitus (DM) (24.24%), 8 patients with COPD (24.24%), alcohol abuse (3.03%) and cigarette smoking (9.09%). The 2 youngest patients in our series were 23 and 24 years old, and these were females with a history of diabetes. The most frequently used medications were antihypertensive drugs, lipid lowering agents, and anti-diabetic drugs.
Most patients (n=16) were referred for surgical treatment, either tenolysis or fasciotomy, upon assessment of the level of involvement.
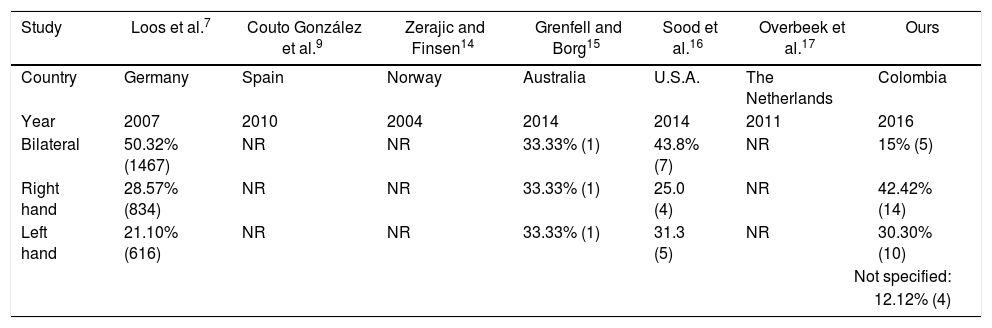
The comparison of our series against other series published showed that although the demographic characteristics and the DC-associated comorbidities are similar, the mode of presentation in our population is different, with a higher frequency of unilateral involvement (Table 2).
Comparison of the characteristics of patients with DC in various series.
| Study | Loos et al.7 | Couto González et al.9 | Zerajic and Finsen14 | Grenfell and Borg15 | Sood et al.16 | Overbeek et al.17 | Ours |
|---|---|---|---|---|---|---|---|
| Country | Germany | Spain | Norway | Australia | U.S.A. | The Netherlands | Colombia |
| Year | 2007 | 2010 | 2004 | 2014 | 2014 | 2011 | 2016 |
| Bilateral | 50.32% (1467) | NR | NR | 33.33% (1) | 43.8% (7) | NR | 15% (5) |
| Right hand | 28.57% (834) | NR | NR | 33.33% (1) | 25.0 (4) | NR | 42.42% (14) |
| Left hand | 21.10% (616) | NR | NR | 33.33% (1) | 31.3 (5) | NR | 30.30% (10) |
| Not specified: | |||||||
| 12.12% (4) | |||||||
Since this is a rare disease, there are not very many series published about DC in the medical literature. There seems to be unanimous agreement about the higher prevalence of the disease among the Caucasian population in Northern Europe, although the information from other ethnic groups is scarce. With regards to gender, the disease is more frequent among males, as evidenced by Couto González et al.,9 that reported an 85.9% prevalence among males, which is similar to the observations in this Colombian series, with 64% of the cases being males (Fig. 1).

The mean age at presentation in this study was 61.3 (±15), which is similar to the mean age reported by Overbeek et al., in his Netherland's series (62±12 years). Considering that DC is a disease that presents more often in patients between sixty and seventy years old, we believe it is significant to highlight the finding in our series of two female patients aged 23 and 24, with a history of diabetes. This suggests that the presentation of the disease at a young age could be associated with metabolic disease.
The presentation with nodules or fibrous bands differs according to the disease progression. With regards to the initial involvement, our series exhibited differences with regards to what was described earlier. The unilateral involvement (72.7%) was more prevalent as opposed to other series, particularly the European, where the majority of patients had both hands involved since the onset of the disease (Fig. 2). This aggressive behavior of the disease, with more functional limitations among the Caucasian population, indicates genetic and environmental differences in the genesis of the disease.

Multiple risk factors associated with DC have been described, including alcohol abuse, cigarette smoking, trauma, DM, dyslipidemia, epilepsy, and HIV. Practically every series agrees in the association between DC and DM, dyslipidemia, and epilepsy.
DM is the result of connective tissue metabolism impairment, with an increase in the intramolecular and intermolecular collagen crosslinks, that reduce their solubility and increase resistance to collagenases. These molecular changes are the result of collagen glycosylation, resulting in its accumulation in the connective tissue; in this case, in the palmar aponeurosis.10 The prevalence of diabetic patients in our series was of 24.4%, which is high, considering that the prevalence of diabetes in the Colombian population is estimated at 8%.11 Furthermore, while 11 patients (33%) presented with hypertension, no claims can be made about the biological likelihood or causality of this condition with DC.
There were no patients with epilepsy in this series of cases. A relationship to DC has been described in the past, and although some more accurate analyses have been made, the predisposition is actually associated with barbiturate therapy. Phenobarbital has a profibrotic effect which is time and dose-dependent.12 Couto Gonzalez et al.9 in his series of 184 patients found a prevalence of epilepsy of just 1.6%.
Another risk factor previously described for DC is alcohol use, with a dose-dependent relationship. Descatha et al. showed that the severity of DC depends on the dose of alcohol used by the patient, so heavy drinkers (more than 3 glasses of any drink per day) have a higher probability of developing DC and requiring surgery.13 In our series we identified just one (3.03%) alcohol user, although considering the small sample size, significant associations may not be ruled out in our population.
Due to the limited information about the occurrence of this disease in our country, we decided to conduct this case report, with a view to show the clinical spectrum in Colombian patients. We believe that this is an important contribution, since although DC is a rare condition, it is the cause of a significant functional limitation when the diagnosis is delayed and therapy is not appropriate. This series gives us a better epidemiological insight about the occurrence of the disease based on the type of population affected and enables a comparison against other populations. Further studies are needed in the future to analyze the genetic, environmental, and immunological factors that account for the differences in the behavior of the disease among the various ethnic groups.
ConclusionDC is a condition with a higher prevalence among males, between 60 and 70 years old. DM is the disease most frequently associated to the occurrence of DC, with no differences among the studies conducted. There is no relationship to epilepsy among the Colombian population. The presentation of DC is variable, and in contrast to other populations in which the presentation is usually bilateral, in our series there is a higher unilateral involvement. The differences are probably due to a different genetic, immunological, and environmental background.
Conflict of interestsThe authors have no conflict of interests to disclose.
We acknowledge Hospital San Pedro y San Pablo, Virgina, Risaralda, for giving us access to the medical records database.
Please cite this article as: Henao Ruiz JE, Ospina Vargas D, Idarraga López DA, García Ospina DA, Quintana Duque MA. Contractura de Dupuytren. Estudio de 33 casos en Colombia. Rev Colomb Reumatol. 2019;26:140–144.
