





Rheumatoid arthritis (RA) is a chronic, inflammatory, and multisystemic disease that has an impact on the quality of life and is associated with depressive symptoms.
ObjectivesTo evaluate the quality of life, overall health status, and depression in patients with RA.
Patients and methodsA cross-sectional study was conducted in the outpatient Rheumatology Outpatient Department of a General Hospital in Mexico City. All patients met the criteria for rheumatoid arthritis according to the American Rheumatism Association, 1987. Clinical and sociodemographic characteristics were recorded. Four measurement tools were used: Arthritis Impact Measurement Scale (AIMS), Dunbar Questionnaire, a Visual Analog Scale, and the Beck Depression Inventory.
ResultsA total of 43 patients aged≥18 years were evaluated. The highest AIMS scores were in social activity (6.49±1.93), pain (4.70±2.04), depression (4.70±2.23), and physical activity (4.03±2.10). The mean score with the Dunbar questionnaire was 6.48±1.87, the mean Visual Analog Scale score was 69.41±24.67, and the mean of the Beck inventory was 15.74±9.85.
ConclusionsThe presence of anxiety and depression has an impact on the quality of life of patients with RA, but not on the presence of comorbidity or disease activity. Depressive symptoms are common in patients with RA, and should therefore be considered when evaluating this rheumatological disease.
La artritis reumatoide (AR) es una enfermedad que afecta la calidad de vida de quienes la padecen y se asocia a sintomatología depresiva.
ObjetivosEvaluar la calidad de vida, el estado global de salud y depresión en pacientes con AR.
Pacientes y métodosSe trata de un estudio transversal y comparativo. Se incluyeron 43 adultos mayores,≥de 18 años, con diagnóstico de AR según los criterios de la American Rheumatism Association de 1987, que acudían al servicio de consulta externa de Reumatología de un hospital general en la ciudad de México. Se determinaron características clínicas y sociodemográficas. Se les aplicaron 4 índices: Escala de Medición del Impacto de la Artritis (AIMS), Cuestionario de Dunbar, Escala Análoga Visual y el Inventario de Depresión de Beck.
ResultadosSe evaluaron 43 pacientes mayores de 18 años, en su mayoría del sexo femenino. Para la AIMS, las puntuaciones más altas fueron en actividad social (6, 49±1, 93), dolor (4,70±2,04), depresión (4,70±2,23) y actividad física (4,03±2,10). Para el cuestionario de Dunbar la puntuación promedio fue de 6, 48±1, 87, en la escala análoga visual la puntuación media fue de 69,41±24,67, finalmente, en el inventario de Beck el promedio fue de 15,74±9,85.
ConclusionesLa presencia de ansiedad y depresión se relacionan con la calidad de vida de los pacientes con AR mas no con la presencia de comorbilidad o actividad de la enfermedad. Los síntomas depresivos son comunes en pacientes con AR por lo que deben considerarse al evaluar esta enfermedad reumatológica.
Rheumatoid arthritis (RA) is a chronic, inflammatory, multisystemic and autoimmune disease, which is characterized by a persistent inflammatory synovitis, causing different degrees of disabililty, loss of quality of life and increased comorbidities in those in whom a control of the pathology has not been achieved. The key sign of the disease is the potential of the synovial inflammation to cause cartilage destruction, with bone erosions and joint deformities. In 2010, it was estimated that the prevalence of RA in the world was 0.5–1% in developed countries, being 3 times more frequent in women than in men.1 In 2011, a cross-sectional study was conducted in Mexico to estimate the prevalence of musculoskeletal diseases, including 5 different regions of the country. The prevalence of RA in Mexico City was 1.6%.2 The presence of depressive symptoms could be conditioned by fear of disability, giving up ambitions with changes in social functionality, a feeling of poor control of the disease and an altered perception with a sensation of loss of functions.3 The severe cronic pain accompanied by progressive joint destruction, disability and disfigurement, increases the risk of suffering emotional disorders.4 Depression is a common comorbidity in patients with RA, being sometimes not diagnosed by the medical staff,5 with a prevalence of 16.8% in the population with RA.6 It is estimated that the prevalence of depression throughout the life, reported by rheumatologists, is 12.9%.5 There is evidence that depressive symptoms temporarily influence the evolution of the activity of RA, although the mechanism is unknown, however, slower rates of decrease in the activity of the disease have been reported. The depressive symptomatology apparently has no relationship with the affected joints and the acute phase reactants.7 The great articular involvement leads patients to have varying degrees of disability, in addition to joint pain and stiffness, more accentuated during the active phase of the disease, which play an important role in the functional disability.8 The health-related quality of life is a concept linked with the individual impact of the disease and its treatment, the functional capacity and the patient's perception in the social, physical and mental roles.9,10 The need to assess the quality of life arises from the increase in life expectancy in our country, since much of the population will reach old age with the consequences of a physiological system in decline, increasing the vulnerability to chronic degenerative diseases and adverse health outcomes, for example, falls and their sequelae.11 The instruments for measuring the quality of life may be generic and specific.10 The generic include the SF-36 questionnaire, the Sickness Impact Profile, the Nothinghan Health Profile and the Dunbar Questionnaire; and the specific include the Arthritis Impact Measurement Scale (AIMS), the Rheumatoid Arthritis Quality of Life, and the Rapid Assessment of Disease Activity.12 The objective of the present study is to evaluate the presence of depression and the quality of life in patients suffering from RA by means of different instruments, since the latter is diminished in rheumatic diseases.
Patients and methodsA cross-sectional and comparative study which included patients from the Rheumatology outpatient service of a general hospital in Mexico City, with a diagnosis of RA made by their rheumatologist according to the criteria of the American Rheumatism Association, 1987.13 In the study participated a total of 43 subjects of legal age, female or male gender, literate, with pharmacological treatment prescribed by their treating physician, among which were included non-steroidal anti-inflammatory drugs, corticosteroids and methotrexate, mainly. The treatment indicated for each patient was not recorded systematically, and data related with the adherence to treatment were not obtained. Patients suffering from juvenile rheumatoid arthritis, from any serious medical disease or with clinically assessed cognitive impairment, were not included. The study was approved by the local ethics committee and informed consent was given by patients who voluntarily agreed to participate in the study. The scales and indexes used in the study are described below.
MeasurementsThe AIMS is used to assess the overall health status of patients with arthritis and other chronic diseases, covering the areas of physical, social and emotional well-being. It consists of 45 items and evaluates 9 dimensions of health and functional capacity.14 The score range goes from 0 to 7 for each dimension and item. The lowest score is equivalent to “never” and the highest score to “always” according to the positive or negative direction of the answer. The Dunbar Questionnaire (consisting of 46 items, elaborated in visual analog scales for their rating from 1 to 10, where the highest score corresponds to a complete well-being) was used to provide a method for assessing the quality of life in patients with affective disorders,15 a Visual Analog Scale was used to estimate the patient's satisfaction with his life; and the Beck Depression Inventory (which consists of 21 items, and each category of the questionnaire describes a specific behavioral manifestation of depression) was used to indicate a measure of severity (not a diagnosis) of the depression under the following categories: normal 0–9, mild 10–15, mild-moderate 16–19, moderate-severe 20–29 and severe >29.16 The criteria of the Disease Activity Score (DAS) in its modified version which includes 28 joints (DAS-28) were used to categorize the patients into 2 groups (with or without active disease).17 This version of the DAS evaluates the swollen joints, the erythrocyte sedimentation rate and the assessment of the patient's activity.18 The DAS-28 has demonstrated to be a reliable and valid measurement for the evaluation of the activity of RA.19
Statistical analysisMeasures of central tendency and dispersion were evaluated for each of the sociodemographic characteristics and indexes. Subsequently, the correlation of each of the indexes with the AIMS scale was evaluated using the Pearson's r correlation coefficient. Using the T test for each of the subscales of the AIMS, the Beck inventory, the Dunbar questionnaire and the visual analog scale, were compared the means between the following groups: those who presented disease activity and those who did not, those who had comorbidities and those who did not, and regarding to those who were dedicated to household tasks and those with other occupations.
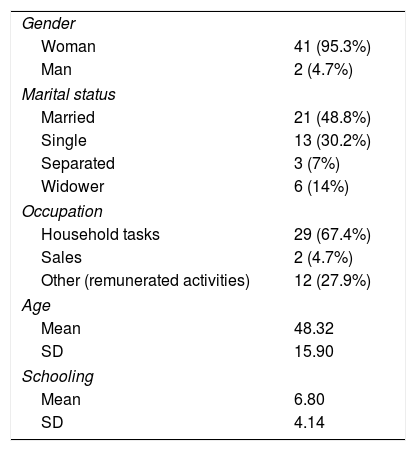
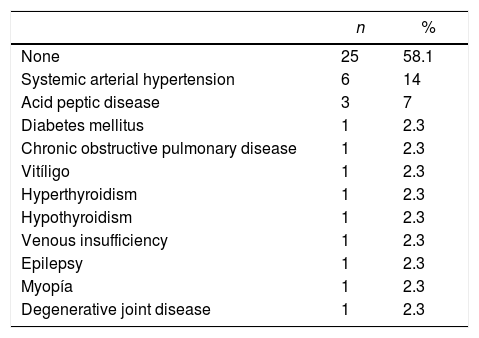
Results43 patients were included, most of them were women 95.3% (n=41) and 4.7% men (n=2), with an average age of 48.3±15.90 years and an average schooling of 6.8±4.22 years. According to the distribution of the marital status of the patients, the majority were married representing 48.8% (n=21). 67.4% were dedicated to household tasks and 32.6% to other remunerated occupations. The clinical and socio-demographic characteristics of the patients are found in Tables 1 and 2 and the comorbidities are listed in Table 3.
Socio-demographic characteristics of the patients.
| Gender | |
| Woman | 41 (95.3%) |
| Man | 2 (4.7%) |
| Marital status | |
| Married | 21 (48.8%) |
| Single | 13 (30.2%) |
| Separated | 3 (7%) |
| Widower | 6 (14%) |
| Occupation | |
| Household tasks | 29 (67.4%) |
| Sales | 2 (4.7%) |
| Other (remunerated activities) | 12 (27.9%) |
| Age | |
| Mean | 48.32 |
| SD | 15.90 |
| Schooling | |
| Mean | 6.80 |
| SD | 4.14 |
Comorbidities of the patients of the study.
| n | % | |
|---|---|---|
| None | 25 | 58.1 |
| Systemic arterial hypertension | 6 | 14 |
| Acid peptic disease | 3 | 7 |
| Diabetes mellitus | 1 | 2.3 |
| Chronic obstructive pulmonary disease | 1 | 2.3 |
| Vitíligo | 1 | 2.3 |
| Hyperthyroidism | 1 | 2.3 |
| Hypothyroidism | 1 | 2.3 |
| Venous insufficiency | 1 | 2.3 |
| Epilepsy | 1 | 2.3 |
| Myopía | 1 | 2.3 |
| Degenerative joint disease | 1 | 2.3 |
The scores of the indexes are found in Table 4. In the AIMS, the highest scores were in social activity with a mean value of 6.49±1.93, followed by the subscale of pain 4.70±2.04, then the depression with values of 4.70±2.23 and the physical activity whose mean score was 4.03±2.10. For the Dunbar questionnaire the mean score was 6.48±1.87. In the visual analog scale the mean score was 69.41±24.67, and finally in the Beck Inventory the mean was 15.74±9.85.
Scores of the indexes used in the study.
| x¯ | SD | Mín. | Máx. | |
|---|---|---|---|---|
| AIMS | ||||
| Mobility | 3.36 | 2.91 | 1.42 | 10 |
| Physical activity | 4.03 | 2.10 | 1.42 | 9.14 |
| Dexterety | 3.22 | 1.86 | 1.42 | 8.57 |
| Social performance | 2.62 | 1.43 | 1.42 | 8.33 |
| Social activity | 6.49 | 1.93 | 1.42 | 10 |
| Daily activities | 2.4 | 1.51 | 1.42 | 9.28 |
| Pain | 6.22 | 2.04 | 1.42 | 9.76 |
| Depression | 4.70 | 2.23 | 1.42 | 9.76 |
| Anxiety | 2.24 | 0.95 | 0.70 | 4.20 |
| Dunbar questionnaire | ||||
| Current subjective quality of life | 6.48 | 1.87 | 2.60 | 9.47 |
| Visual analog scale | ||||
| Overall quality of life (subjective) | 69.41 | 24.67 | 5.0 | 100 |
| Beck's inventory | ||||
| Severity of the depressive symptoms | 15.74 | 9.85 | 0 | 40 |
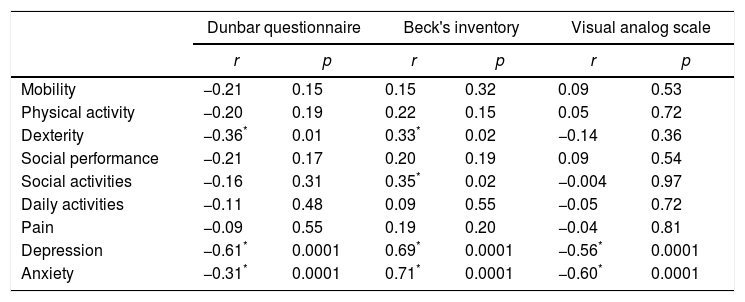
The correlations between the AIMS and the indexes used in the study are shown in Table 5. Between the Dunbar questionnaire and the AIMS, negative correlations above 0.3 were obtained in the following subitems: dexterity (r=−0.36, p=0.01), depression (r=−0.61, p=0.0001) and anxiety (r=0.64, p=0.0001). Between the Beck inventory and the AIMS, direct and significant correlations were observed in the subitems of the AIMS scale: dexterity (r=0.33, p=0.02), depression (r=0.69, p=0.0001) and anxiety (r=0.70, p=0.001). Regarding the visual analog scale there were inverse correlations with the following subitems of the AIMS: depression (r=−0.56, p=0.0001) and anxiety (r=−0.60, p=0.0001).
Correlations between the AIMS and the indexes used in the study.
| Dunbar questionnaire | Beck's inventory | Visual analog scale | ||||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| Mobility | −0.21 | 0.15 | 0.15 | 0.32 | 0.09 | 0.53 |
| Physical activity | −0.20 | 0.19 | 0.22 | 0.15 | 0.05 | 0.72 |
| Dexterity | −0.36* | 0.01 | 0.33* | 0.02 | −0.14 | 0.36 |
| Social performance | −0.21 | 0.17 | 0.20 | 0.19 | 0.09 | 0.54 |
| Social activities | −0.16 | 0.31 | 0.35* | 0.02 | −0.004 | 0.97 |
| Daily activities | −0.11 | 0.48 | 0.09 | 0.55 | −0.05 | 0.72 |
| Pain | −0.09 | 0.55 | 0.19 | 0.20 | −0.04 | 0.81 |
| Depression | −0.61* | 0.0001 | 0.69* | 0.0001 | −0.56* | 0.0001 |
| Anxiety | −0.31* | 0.0001 | 0.71* | 0.0001 | −0.60* | 0.0001 |
When comparing the subjects who did or did not have disease activity, there were only differences in the pain subscale of the AIMS, with a mean score of 7.61±0.86 vs. 6.00±2.09 (t=−1.84, gl=36.5, p=0.05). When the patients had a comorbidity, they showed significant differences in the AIMS scale in the subscales of dexterity 3.73±2.28 vs. 2.86±1.42 (t=−1.52, gl=17.24, p=0.03) and social performance with values of 3.01±1.95 vs. 2.34±0.85 (t=−1.52, gl=17.24, p=0.0003). In the comparison of the occupation, which only included the female patients (n=41), differences were found between those who were dedicated to household tasks and those who had another remunerated occupation in the AIMS scale in the subscales of social performance 2.84±1.61 vs. 2.28±0.88 (t=−1.14, gl=28.11, p=0.04) and daily activities 2.29±1.18 vs. 2.82±2.19 (t=1.01, gl=11.28, p=0.007). No correlations were found in the Beck inventory, the Dunbar questionnaire and the visual analog scale with the disease activity, the presence or absence of comorbidities and the occupation of the patients.
DiscussionThe clinical-demographic results of our study differ discreetly from other studies. Regarding the age, our patients had an average of 48 years, in most of the studies the average age is between 51 and 59 years.10,12,20,21 In relation to the gender, in our study predominated the female gender (95%) coinciding with the same studies previously cited. The average schooling of our sample is 6.8 years, being slightly higher than in the study conducted by Ambriz et al.,10 in Mexican population with an average of 5.88 years. The time of evolution of the disease was 11 years on average, only coinciding with the study by Vinaccia et al.12
The patients recruited in this study presented a greater repercussion on social activities due to the RA with a score in the AIMS of 6.49 (SD 1.93), followed by the subscales: pain 6.22 (SD 2.04), physical activity 4.03 (SD 2.10), depression 4.70 (SD 2,23) and anxiety 2.24 (SD 0.95). Ndosi et al.,22 applied the AIMS2-SF scale (short version of the AIMS 2 with a high internal consistency),23 reporting a higher score in the social subscale, followed by pain and thirdly by the affect. Robles-García et al.,24 applied the AIMS-2 scale in Mexican women with osteoartrosis reporting similar results. The subscale with the highest score was pain, followed by the subscales of social activity, level of stress, and walking and flexing. Despite the above-mentioned authors applied different versions of the AIMS, patients suffering from RA report a greater repercussion on their social activities, followed by a high score in the subscale of pain, which could be a factor that affects the social interaction between individuals and their environment. The chronic pain experienced by the patients with RA influences the mood, so it is expected to manifest with negative changes. The third subscale with a high score corresponds to the affective field (level of stress, anxiety and depression). It is probable that these 3 subscales are related to each other, because the fact of presenting chronic pain makes the person, who is accustomed to interact in some way with his/her environment, to be limited in his/her social activities and it has a negative influence on his/her affection.
The average score of the depressive symptoms using the Beck Inventory was 15.74 (SD 9.85), being similar though that reported by Kojima et al.,25 with 12.9 (SD 9.6) and almost twice the score reported by Heimans et al.,26 of 8.5 (SD 7.7). Isik et al.,27 applied the Hamilton depression rating scale to those patients who already had a diagnosis of major depressive disorder, obtaining a score of 17.48 (SD 1.86); the patients in this study had a moderate depression (categorizing quantitatively the severity of the symptoms). In our study, the results were not divided according to the ranges of severity of the depressive symptoms, but it can be affirmed that most of the patients with RA have depressive symptoms, coinciding with that was reported by the authors previously mentioned.
In the Dunbar questionnaire, the average score was 6.48 (SD 1.87), there are no reports of previous studies in which this scale has been used in patients with RA, however, if we consider that being very satisfied is 10, the subjects with RA showed a deterioration in quality of life, although it could be related to the presence of depressive and anxious symptoms. It was found a negative correlation between dexterity and quality of life. Similar results were also obtained in the visual analog scale with negative correlations for depression and anxiety, that is, the higher score of depressive or anxious symptoms, the less satisfaction with life.
It was observed that regarding the comparison of the active or inactive disease, the only significant difference is the greater presence of pain during the active phase, which is expected due to the presence of joint inflammation during this stage. Although the scores of the instruments used did not reach significant levels, they are higher when the disease is active. The lack of significance could be due to the sample size, since only 6 patients presented the activity phase of RA. The fact of having any comorbidity has repercussions on the social performance and the dexterity of the patients with significant values, however, there were no differences regarding the severity of the depression or a worse quality of life.
It was observed that patients who have a remunerated occupation have a better social performance, however, women who dedicate themselves to household tasks perform daily activities better. This result draws attention because the scores of these subscales of mobility, physical activity and pain were higher, although they did not have statistical significance.
The presence of anxiety and depression is related to the quality of life of the patients with RA, but not with the presence of comorbidity or disease activity. The AIMS is an instrument that helps us to assess the health status of patients with RA, however, it does not evaluate satisfaction with life, since the correlations of a specific instrument to measure it (such as the Dunbar questionnaire) were low, correlating only with anxiety and depression.
In Mexico there is only one study, conducted by Ambriz et al.,10 in which the quality of life in RA an other 3 chronic diseases was evaluated. It is necessary to design further studies in the future aimed at evaluating the quality of life of the patients and not only the measurement of the impact that the disease has on health.
In our study, the majority of the patients had depressive symptoms, and for this reason we consider that it is important to identify the depressive symptomatology when evaluating patients with chronic-degenerative diseases, in this case RA, since they are symptoms that may go unnoticed during the consultation and have a negative impact on the quality of life.
Among the limitations of the present work, we must mention that a systematic record of the drugs used by each patient was not carried out, and the adherence to pharmacological treatment was not systematically evaluated.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interestThe authors declare they do not have any conflict of interest.
To the General Hospital “Dr. Manuel Gea González” and to the Rheumatology Outpatient Service of the same hospital for allowing us to carry out the research.
Please cite this article as: Guerrero-López JB, Cabrera DM, del Carmen Lara-Muñoz M, García RO. Evaluación de la calidad de vida y depresión en pacientes con artritis reumatoide en un hospital general. Rev Colomb Reumatol. 2017;24:199–204.

www.publicationethics.org.