



Low back pain is a prevalent condition with health, social and occupational impact. The aim of this study is to assess the influence of social and occupational factors on worker patients with low back pain.
MethodA descriptive study was conducted on 349 subjects with low back pain. The main independent variable was being a manual or non-manual worker. Other social-occupational and lifestyle variables were also considered. The level of disability was established according to the Oswestry low back pain disability questionnaire, and the association between the type of job and the test was evaluated using multiple linear regressions.
ResultsManual workers are heavier smokers (47%), experience more pain (74.3%), have a lower economic status (89.3%), use more drugs (57.7%), have limitations in walking (17.5%) and standing (25.6%), used carrying protocols (85.5%), make repetitive movements (77.4%). They made trunk (52.6%) and upper limb movements (24.8%), and received less prevention training (51.7%), but used low back protection (19.6%).
The non-manual workers had greater limitation in handling loads (37.4%) and sitting (43.5%), and computer screen user protocols were applied (94.8%), and had a lower social class classification (57.1 low-middle class).
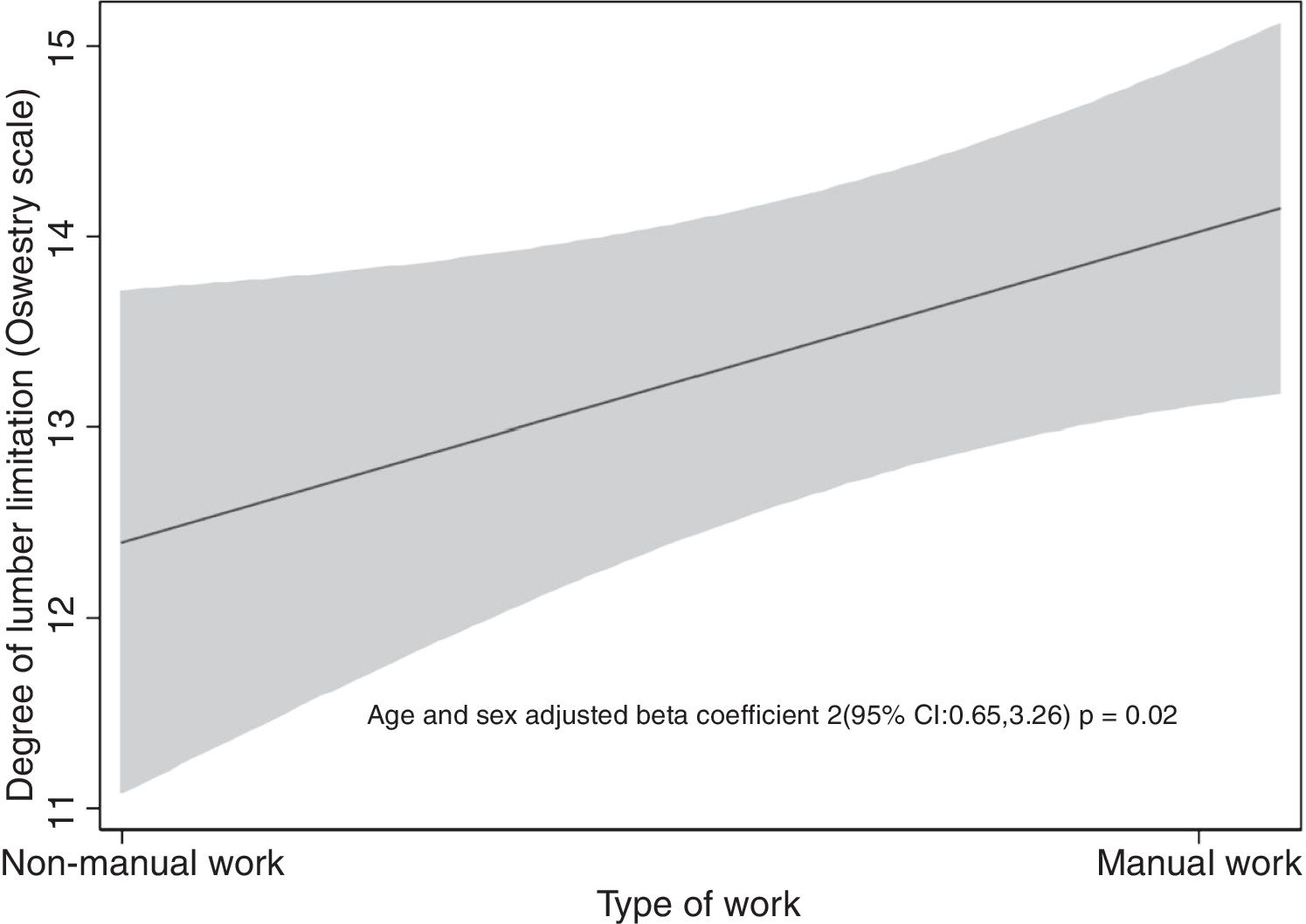
Performing manual tasks at work is significantly associated with an increase of 2 points in the Oswestry test compared to non-manual workers, when adjusted for age and gender (coefficient β: 2, 95% CI: 0.6–3.36).
ConclusionLow back pain is a prevalent condition, with an unfavorable prognosis that has an individual, social, and occupational impact. Performing manual tasks is associated with an increase in the disability scale, regardless of age and gender.
El dolor lumbar es una dolencia prevalente con repercusión sanitaria, social y laboral. Es objetivo de este trabajo valorar la influencia de las variables sociolaborales en pacientes con lumbalgia que trabajan.
MétodoEstudio descriptivo en 349 sujetos con lumbalgia. Es variable independiente principal ser trabajador manual y no manual; también son recogidas otras variables sociolaborales y de estilo de vida. La incapacidad se obtuvo mediante la escala del cuestionario de Oswestry y la asociación entre el tipo de tarea y el test se evaluó con regresión lineal múltiple.
ResultadosLos trabajadores manuales consumen más tabaco (47%), tienen más dolor (74.3%), peor situación económica (89.3%), consumen más fármacos (57.7%), tienen limitación en deambulación (17.5%) y bipedestación (25.6%), se les aplican protocolos de cargas (85.5%) y movimientos repetidos (77.4%), realizan movimientos de tronco (52.6%) y miembros superiores (24.8%) y reciben menor formación preventiva (51.7%), pero utilizan protección lumbar (19.6%).
Los trabajadores no manuales tienen mayor limitación en cargas (37.4%) y sedestación (43.5%) se les aplican protocolos de usuarios de pantallas (94.8%) y tienen peor tipificación en clase social (57,1 clase media-baja).
Realizar tareas manuales en el trabajo se asocia significativamente con un aumento de 2 puntos en el test de Oswestry respecto a los no manuales, ajustado por edad y género (coeficiente β: 2, IC 95%: 0,65–3,36).
ConclusiónLa lumbalgia es una dolencia prevalente, de curso desfavorable, que implica impacto individual, social y laboral. Realizar tareas manuales se asocia con un aumento en la escala de incapacidad, independientemente de la edad y el género.
Low back pain is a prevalent disease affecting people of all ages and limits patients around the world. Despite the progress achieved in treatment methods, low back pain management continues to be challenging for researchers and clinicians. Among the reasons, the most salient ones are the broad range of manifestations, the different causes, the triggering and maintenance factors, the course of the disease, the prognosis, and the consequences in terms of health-related quality of life (LRQOL), emphasizing the need for a multidisciplinary approach for treating low back pain, integrating the biological, psychological, social and labor components.1
Together with cervical pain, lumbar pain is considered the main cause of disability in most countries, according to 2015 data.2 Low back pain not only impacts the affected individual and his/her environment, but also results in a huge socioeconomic impact in terms of medical care, absenteeism, and sick leaves.3,4
Low back pain has a deep effect on wellbeing and is usually the cause of physical disability affecting on the job performance, social responsibilities, family life, and is an increasingly important factor in the escalation of medical care costs an sick leaves. Pain chronicity results in social, healthcare, and labor costs due to the need to use healthcare resources and support due to quality of life issues.5
Different risk factors increase the prevalence of this condition; the most relevant risk factors are: age,6 the type of job or occupation of the subject,7,8 gender (woman are more affected),9,10 and overweight and obesity.11
As the population ages, the number of people with low back pain is expected to rise, which encourages further studies to assess the influence of comorbid factors (for instance, obesity, smoking, lack of exercise), lifestyle factors and occupational hazards that help to control the escalation of costs.12
For public health purposes it is extremely important to have information on age, gender, and type of work variables, and their relationship to occupational hazards, the prevention protocols implemented, and the impact of limitations associated with low back pain.
Along this lines, several research projects have been conducted with a view to identifying workers with different disabilities caused by low back pain, and determining to what extent are these associated with personal, occupational, or lifestyle factors and related to the pain characteristics. The results show that pain may be affected by various physical and psychosocial factors which are modifiable at work and outside the work environment, and may be subject to preventive measures.13 These conclusions are consistent with the reports from other papers on persistent and severe low back pain associated with medical leave and poor work performance, emphasizing the need for preventive strategies based on the awareness of risk factors and a comprehensive approach to reduce the labor and social impact among working populations.14
The most consistent occupational hazards for new episodes of low back pain and also for cervical pain are manual labor and repetitive movements and strain, particularly when previous episodes have been experienced. But, in addition to occupational prevention, extra-occupational aspects should also be considered, in addition to the adoption of evidence-based secondary prevention measures including recommendations to be constantly active.15
The underlying hypothesis in this paper is that low back pain is a highly prevalent condition that involves interrelated personal, social and occupational aspects.
The objective of this study is to estimate the impact of low back pain on social and occupational variables collected from the medical records of patients with low back pain from a traumatology unit in the Community of Valencia, and assess the disability resulting from the ensuing limitations.
MethodDescriptive study including 349 subjects from the Malvarrosa Traumatology Unit in Valencia, Spain. The inclusion criteria were: symptoms of low back pain, regardless of the causal etiology, and consultation with a traumatology specialist; be actively employed (unemployed individuals at the time of the survey were excluded). Productive age (18–65 years), participating voluntarily and giving a written consent to use the data for epidemiological purposes, and securing the authorization of the ethics committee of the health institution to carry out the trial (procedure number F-CE-GEva-15v1.1).
All the procedures followed the principles of the Declaration of Helsinki of the World Medical Association, and the protocols were approved by the Ethics in Human Research Committee of the Hospital Clínico de Valencia (Spain).
A clinical interview was conducted that included sociodemographic information such as age, gender, lifestyle, smoking and alcohol use, and functional limitation.
The age of the participants was classified into three groups: <40 years, 40–49 years and 50 years. Smoking was classified as: non-smoker, active smoker, and ex-smoker (at least one year without smoking) and the number of packs/year based on the number of cigarettes smoked per day, multiplied by the number of years smoking and divided by 20 (use of electronic calculation).16 In the opinion of the authors, healthy eating was considered as the intake of fruits and vegetables at least 3 times per week. Also according to the authors, physical exercise was classified as: never, occasional, 1–3 days per week, 3–6 days per week and daily. The use of alcohol was classified based on the grams of alcohol intake (UBE calculation)17: no consumption, low-mild risk consumption (<11 UBE per week in women and less than 17 in men), and hard – abusive consumption (>17 in women and 28 in men).
Social status and type of work. To evaluate the social status, 3 classes are identified: class 1, class 2 and class 3, based on the National Classification of Occupations of 1994 (NCO-94). The type of work is established based on these classifications as: blue collar (manual worker) and white collar (non-manual worker).
The social status calculation was based on the NCO-94. Each job in the study was included in one group pursuant to NCO-94. The list of occupations of the NCO-94 is considered according to a three digit code so that workers are included in one of the six groups of the abbreviated classification.18 For improved management, based on these 6 groups, a new classification is implemented by grouping the workers in I and II into the social status 1 category; workers in III belong to social status 2, and finally IVa, IVb, and v are considered social status 3. NCO-94 also allows divides workers into manual (blue collar) y non-manual (white collar); this takes into account the list of occupations with the first digit from 1 to 4 and which are considered non-manual workers, while workers with the first digit between 5 and 9 belong to the manual workers category.18
Pain intensity is measured with a digital analogue scale. The authors further classified it into absence of pain, mild pain if ≤6, moderate pain if between 7–8, and severe pain if ≥9.19
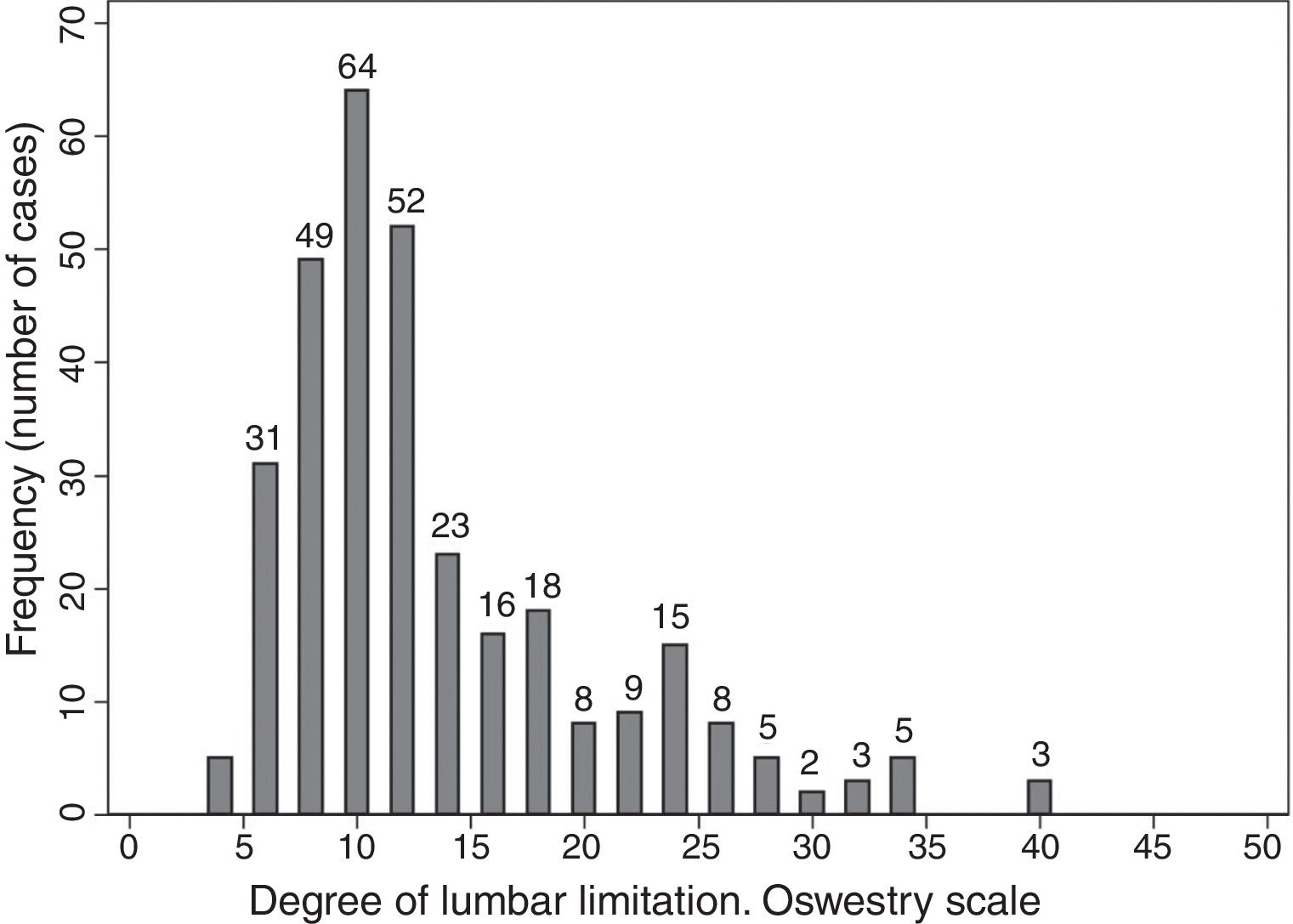
The impact of limitations is evaluated based on the Oswestry back pain disability scale questionnaire, adapted to the Spanish population by Flórez García et al. in 1995.20 The scale has 10 questions with 6 possible answers each, and are scored individually, besides the overall assessment. Each item is scored from 0 to 5, from the lowest to the highest limitation. The scoring system is as follows: the test comprises 10 items, each one has 6 options which are rated from 0 to 5. The maximum total score adding up all the items is 50, and the percentage of limitation/disability is the result of dividing the total score obtained by 50 and multiplying the result by 100. With regards to the classification: 0–20% is minimal functional limitation, 20–40% is moderate functional limitation, 40–60% is intense functional limitation, 60–80% assumes disability, and above 80% is maximum functional limitation (Appendix Banexo 1). The questionnaire presents adequate metrics.21
The impact on temporary disability (TD) is established in terms of the number of back pain episodes resulting in medical leave, as reported by the worker over the last year and the duration expressed in days.
Protocols are used in Occupational Medicine for specific health surveillance of workers and are approved by the Ministry of Health, Consumption and Social Welfare, in terms of the risk or risks of the worker at the job site, pursuant to Article 22 of the Law of Prevention of Occupational Hazards and Technical Note on Prevention 959 of the INSST.22–24
Statistical analysisIn order to assess the characteristics of the population, the participants were grouped according to the type of work (manual and non-manual). The frequencies of the categorical variables of the questionnaire and the central tendency and standard deviation measures were estimated as quantitative variables. In order to compare the percentages among groups of the different variables the χ2 and the Student t-test were used to compare measurements. The distribution of our population was described using a frequency histogram, based on the level of low back pain according to Oswestry. In order to estimate the association between the type of work and the disability, a multiple lineal regression approach adjusted by age and gender was used, and a β coefficient and its 95% confidence interval were obtained. The level of statistical significance in all cases was p < 0.05. The statistical analysis was conducted using STATA version 12.0 software.
Results349 patients participated, of which 197 were males (56.4%) and 152 females (43.6%) with a mean age of 44 years (SD: 6.9); 44.9 years in males (SD: 6.8) and 43 in females (SD: 7.0). The level of education was: elementary 47.4%, middle education 31.5% and higher education 21.1%.
The differences found in the participating population based on the type of work performed are shown in Tables 1, 2, and 3.
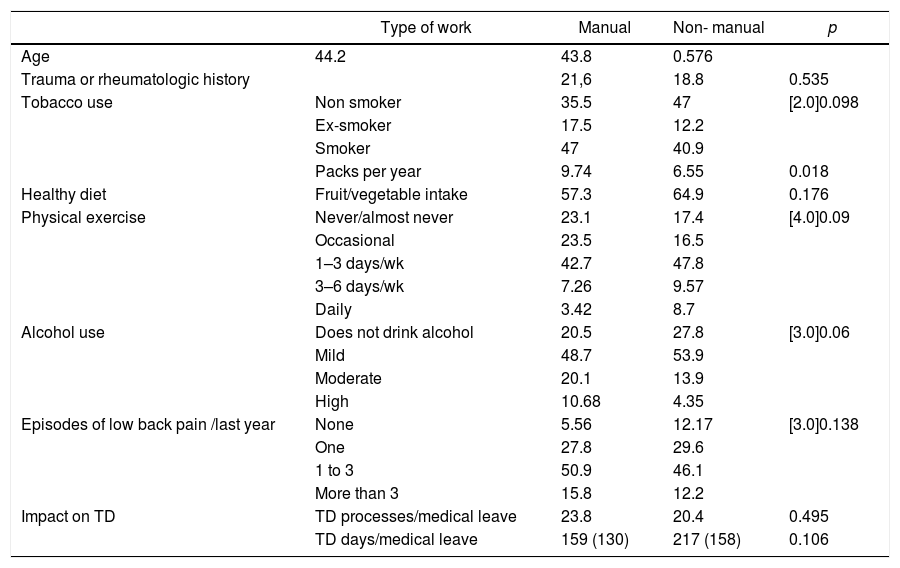
Percentual relationship of the type of work with personal variables.
| Type of work | Manual | Non- manual | p | |
|---|---|---|---|---|
| Age | 44.2 | 43.8 | 0.576 | |
| Trauma or rheumatologic history | 21,6 | 18.8 | 0.535 | |
| Tobacco use | Non smoker | 35.5 | 47 | [2.0]0.098 |
| Ex-smoker | 17.5 | 12.2 | ||
| Smoker | 47 | 40.9 | ||
| Packs per year | 9.74 | 6.55 | 0.018 | |
| Healthy diet | Fruit/vegetable intake | 57.3 | 64.9 | 0.176 |
| Physical exercise | Never/almost never | 23.1 | 17.4 | [4.0]0.09 |
| Occasional | 23.5 | 16.5 | ||
| 1–3 days/wk | 42.7 | 47.8 | ||
| 3–6 days/wk | 7.26 | 9.57 | ||
| Daily | 3.42 | 8.7 | ||
| Alcohol use | Does not drink alcohol | 20.5 | 27.8 | [3.0]0.06 |
| Mild | 48.7 | 53.9 | ||
| Moderate | 20.1 | 13.9 | ||
| High | 10.68 | 4.35 | ||
| Episodes of low back pain /last year | None | 5.56 | 12.17 | [3.0]0.138 |
| One | 27.8 | 29.6 | ||
| 1 to 3 | 50.9 | 46.1 | ||
| More than 3 | 15.8 | 12.2 | ||
| Impact on TD | TD processes/medical leave | 23.8 | 20.4 | 0.495 |
| TD days/medical leave | 159 (130) | 217 (158) | 0.106 | |
IT: Temporary disability; wk: week.
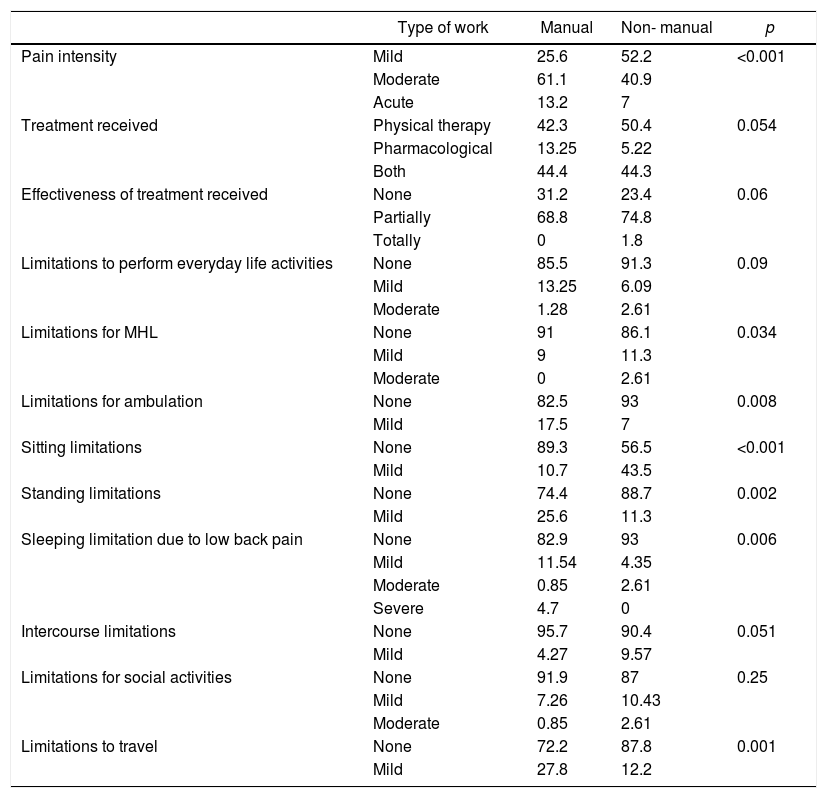
Percentual relationship of the type of work with low back pain-associated clinical variables.
| Type of work | Manual | Non- manual | p | |
|---|---|---|---|---|
| Pain intensity | Mild | 25.6 | 52.2 | <0.001 |
| Moderate | 61.1 | 40.9 | ||
| Acute | 13.2 | 7 | ||
| Treatment received | Physical therapy | 42.3 | 50.4 | 0.054 |
| Pharmacological | 13.25 | 5.22 | ||
| Both | 44.4 | 44.3 | ||
| Effectiveness of treatment received | None | 31.2 | 23.4 | 0.06 |
| Partially | 68.8 | 74.8 | ||
| Totally | 0 | 1.8 | ||
| Limitations to perform everyday life activities | None | 85.5 | 91.3 | 0.09 |
| Mild | 13.25 | 6.09 | ||
| Moderate | 1.28 | 2.61 | ||
| Limitations for MHL | None | 91 | 86.1 | 0.034 |
| Mild | 9 | 11.3 | ||
| Moderate | 0 | 2.61 | ||
| Limitations for ambulation | None | 82.5 | 93 | 0.008 |
| Mild | 17.5 | 7 | ||
| Sitting limitations | None | 89.3 | 56.5 | <0.001 |
| Mild | 10.7 | 43.5 | ||
| Standing limitations | None | 74.4 | 88.7 | 0.002 |
| Mild | 25.6 | 11.3 | ||
| Sleeping limitation due to low back pain | None | 82.9 | 93 | 0.006 |
| Mild | 11.54 | 4.35 | ||
| Moderate | 0.85 | 2.61 | ||
| Severe | 4.7 | 0 | ||
| Intercourse limitations | None | 95.7 | 90.4 | 0.051 |
| Mild | 4.27 | 9.57 | ||
| Limitations for social activities | None | 91.9 | 87 | 0.25 |
| Mild | 7.26 | 10.43 | ||
| Moderate | 0.85 | 2.61 | ||
| Limitations to travel | None | 72.2 | 87.8 | 0.001 |
| Mild | 27.8 | 12.2 |
MHL: manual handling of loads.
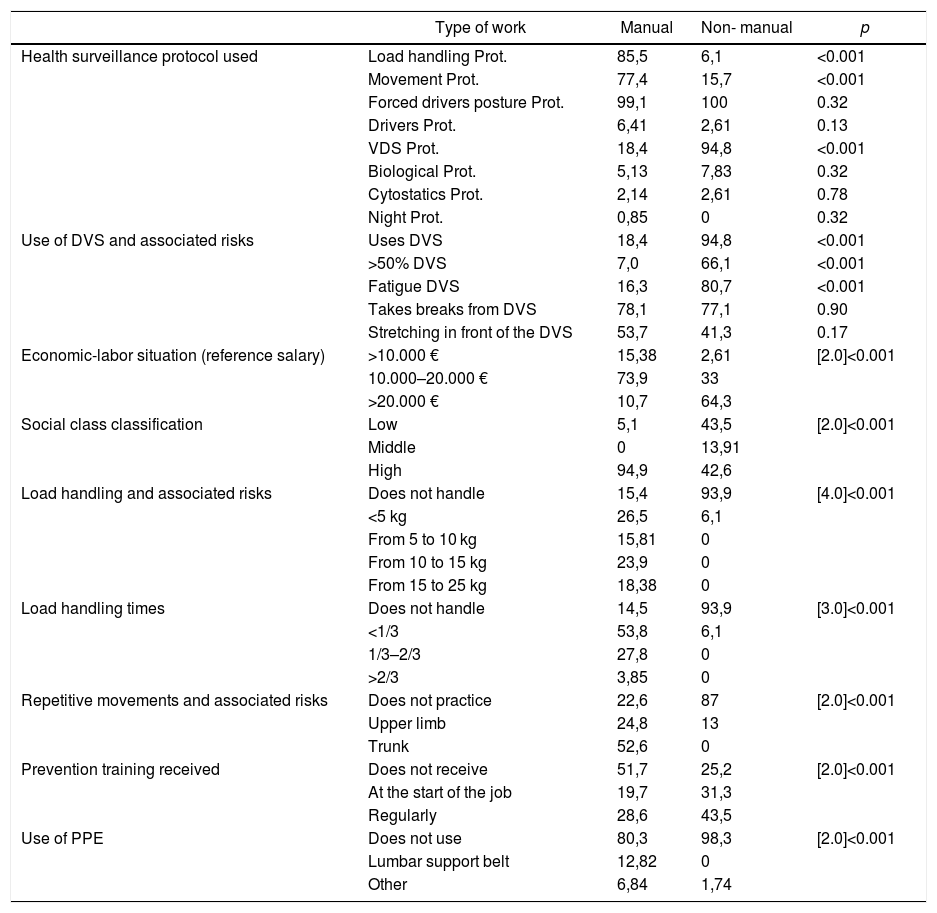
Percentual relationship of the type of work with occupational variables.
| Type of work | Manual | Non- manual | p | |
|---|---|---|---|---|
| Health surveillance protocol used | Load handling Prot. | 85,5 | 6,1 | <0.001 |
| Movement Prot. | 77,4 | 15,7 | <0.001 | |
| Forced drivers posture Prot. | 99,1 | 100 | 0.32 | |
| Drivers Prot. | 6,41 | 2,61 | 0.13 | |
| VDS Prot. | 18,4 | 94,8 | <0.001 | |
| Biological Prot. | 5,13 | 7,83 | 0.32 | |
| Cytostatics Prot. | 2,14 | 2,61 | 0.78 | |
| Night Prot. | 0,85 | 0 | 0.32 | |
| Use of DVS and associated risks | Uses DVS | 18,4 | 94,8 | <0.001 |
| >50% DVS | 7,0 | 66,1 | <0.001 | |
| Fatigue DVS | 16,3 | 80,7 | <0.001 | |
| Takes breaks from DVS | 78,1 | 77,1 | 0.90 | |
| Stretching in front of the DVS | 53,7 | 41,3 | 0.17 | |
| Economic-labor situation (reference salary) | >10.000 € | 15,38 | 2,61 | [2.0]<0.001 |
| 10.000–20.000 € | 73,9 | 33 | ||
| >20.000 € | 10,7 | 64,3 | ||
| Social class classification | Low | 5,1 | 43,5 | [2.0]<0.001 |
| Middle | 0 | 13,91 | ||
| High | 94,9 | 42,6 | ||
| Load handling and associated risks | Does not handle | 15,4 | 93,9 | [4.0]<0.001 |
| <5 kg | 26,5 | 6,1 | ||
| From 5 to 10 kg | 15,81 | 0 | ||
| From 10 to 15 kg | 23,9 | 0 | ||
| From 15 to 25 kg | 18,38 | 0 | ||
| Load handling times | Does not handle | 14,5 | 93,9 | [3.0]<0.001 |
| <1/3 | 53,8 | 6,1 | ||
| 1/3–2/3 | 27,8 | 0 | ||
| >2/3 | 3,85 | 0 | ||
| Repetitive movements and associated risks | Does not practice | 22,6 | 87 | [2.0]<0.001 |
| Upper limb | 24,8 | 13 | ||
| Trunk | 52,6 | 0 | ||
| Prevention training received | Does not receive | 51,7 | 25,2 | [2.0]<0.001 |
| At the start of the job | 19,7 | 31,3 | ||
| Regularly | 28,6 | 43,5 | ||
| Use of PPE | Does not use | 80,3 | 98,3 | [2.0]<0.001 |
| Lumbar support belt | 12,82 | 0 | ||
| Other | 6,84 | 1,74 |
PPE: personal protection equipment; Prot.: protocol; DVS: data visualization screen.
There was a higher consumption of tobacco in terms of packs/year and alcohol among the manual workers (p < 0.05) and more physical exercise among the non-manual workers (p < 0.05). No significant differences were observed with regards to the type of work according to age, gender or lifestyle, between the manual/non-manual workers, or with regards to temporary disability.
Manual workers exhibited a higher low back pain intensity (p < 0.05) and they use medications more often. The non-manual workers do more physical therapy and get more effective results from their therapies. Manual workers use more medicines, either alone or combined with physical therapy, though the results are not conclusive. The limitations for handling of loads and sitting are more significant among the non-manual workers (p < 0.05), while manual workers experience more limitations for ambulation and standing (p < 0.05). Manual workers experience more limitations for traveling (p < 0.05). The results are non-conclusive in terms of limitations for sexual intercourse as a result of low back pain, though there is a tendency to be higher among the non-manual workers.
For health surveillance purposes, manual handling of loads (MHL) and repetitive movement (RM) protocols are administered to manual workers; and the data visualization screen (DVS) is used for non-manual workers (p < 0.05) since more than 50% of their workday is spent in front of the screen; the most usual complaint is fatigue (p < 0.05).
Manual workers are required to handle heavier loads and longer exposure (p < 0.05) and their economic condition is worse than that of the non-manual workers (p < 0.05). Non-manual workers have a worse social class categorization (p < 0.05).
Manual workers do more repetitive movements of the trunk and upper limbs than the non-manual (p < 0.05) and receive less prevention training than the latter (p < 0.05). In the case of non-manual workers, prevention training is administered at the start of their employment and periodically to update their knowledge. The use of personal protection equipment, particularly the lumbar support belt is more frequent among manual workers (p < 0.05).
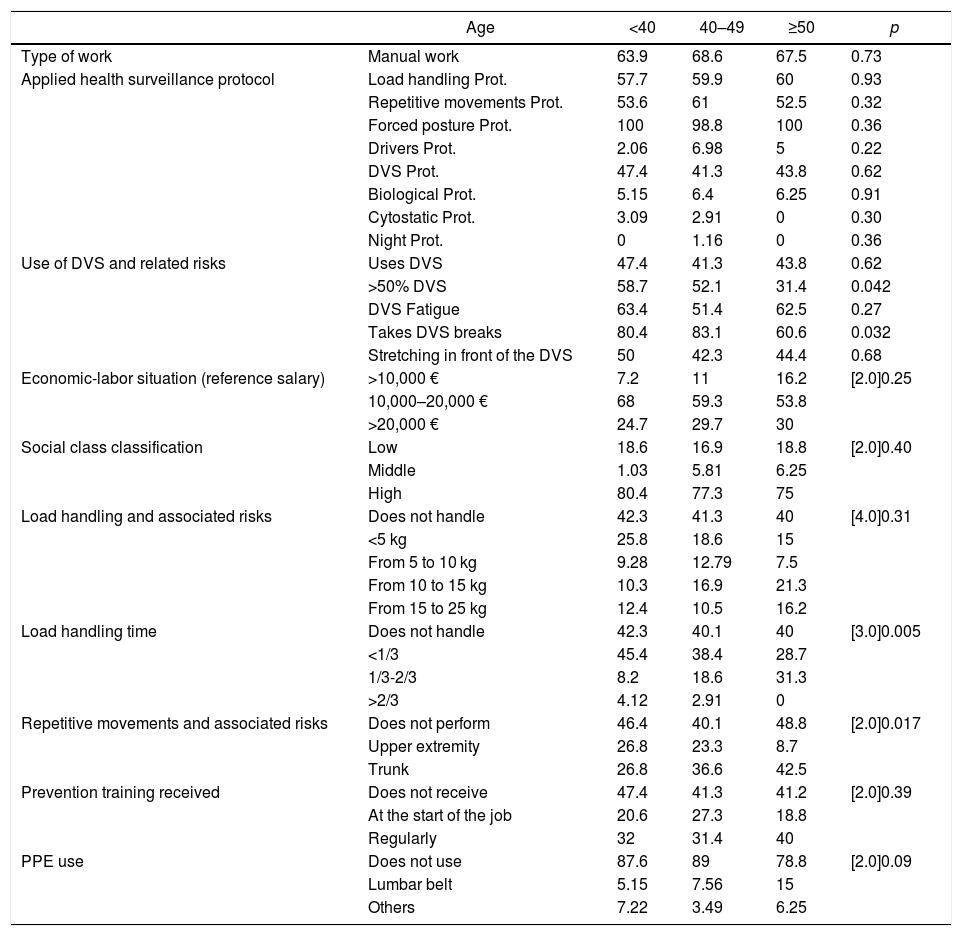
The differences found among the participating population based on age and occupational variables are illustrated in Table 4.
Percentual relationship of age with occupational variables.
| Age | <40 | 40–49 | ≥50 | p | |
|---|---|---|---|---|---|
| Type of work | Manual work | 63.9 | 68.6 | 67.5 | 0.73 |
| Applied health surveillance protocol | Load handling Prot. | 57.7 | 59.9 | 60 | 0.93 |
| Repetitive movements Prot. | 53.6 | 61 | 52.5 | 0.32 | |
| Forced posture Prot. | 100 | 98.8 | 100 | 0.36 | |
| Drivers Prot. | 2.06 | 6.98 | 5 | 0.22 | |
| DVS Prot. | 47.4 | 41.3 | 43.8 | 0.62 | |
| Biological Prot. | 5.15 | 6.4 | 6.25 | 0.91 | |
| Cytostatic Prot. | 3.09 | 2.91 | 0 | 0.30 | |
| Night Prot. | 0 | 1.16 | 0 | 0.36 | |
| Use of DVS and related risks | Uses DVS | 47.4 | 41.3 | 43.8 | 0.62 |
| >50% DVS | 58.7 | 52.1 | 31.4 | 0.042 | |
| DVS Fatigue | 63.4 | 51.4 | 62.5 | 0.27 | |
| Takes DVS breaks | 80.4 | 83.1 | 60.6 | 0.032 | |
| Stretching in front of the DVS | 50 | 42.3 | 44.4 | 0.68 | |
| Economic-labor situation (reference salary) | >10,000 € | 7.2 | 11 | 16.2 | [2.0]0.25 |
| 10,000–20,000 € | 68 | 59.3 | 53.8 | ||
| >20,000 € | 24.7 | 29.7 | 30 | ||
| Social class classification | Low | 18.6 | 16.9 | 18.8 | [2.0]0.40 |
| Middle | 1.03 | 5.81 | 6.25 | ||
| High | 80.4 | 77.3 | 75 | ||
| Load handling and associated risks | Does not handle | 42.3 | 41.3 | 40 | [4.0]0.31 |
| <5 kg | 25.8 | 18.6 | 15 | ||
| From 5 to 10 kg | 9.28 | 12.79 | 7.5 | ||
| From 10 to 15 kg | 10.3 | 16.9 | 21.3 | ||
| From 15 to 25 kg | 12.4 | 10.5 | 16.2 | ||
| Load handling time | Does not handle | 42.3 | 40.1 | 40 | [3.0]0.005 |
| <1/3 | 45.4 | 38.4 | 28.7 | ||
| 1/3-2/3 | 8.2 | 18.6 | 31.3 | ||
| >2/3 | 4.12 | 2.91 | 0 | ||
| Repetitive movements and associated risks | Does not perform | 46.4 | 40.1 | 48.8 | [2.0]0.017 |
| Upper extremity | 26.8 | 23.3 | 8.7 | ||
| Trunk | 26.8 | 36.6 | 42.5 | ||
| Prevention training received | Does not receive | 47.4 | 41.3 | 41.2 | [2.0]0.39 |
| At the start of the job | 20.6 | 27.3 | 18.8 | ||
| Regularly | 32 | 31.4 | 40 | ||
| PPE use | Does not use | 87.6 | 89 | 78.8 | [2.0]0.09 |
| Lumbar belt | 5.15 | 7.56 | 15 | ||
| Others | 7.22 | 3.49 | 6.25 |
PPE: personal protection equipment; Prot.: protocol; DVS: data visualization screen.
Younger workers are more exposed to DVS to do their work, spending over 50% of their workday in front of the screen (p < 0.05); additionally, they adopt preventive measures of scheduled breaks (p < 0.05). The handling of loads is irregularly distributed among the various age groups, although there is a tendency to evenly distribute the work load when there is no MHL and to increase with age, but in cases of higher loads, it is mostly observed among the youngest as well as among the oldest. Repetitive movements of the upper limbs are more frequent among younger workers and of the trunk in older workers.
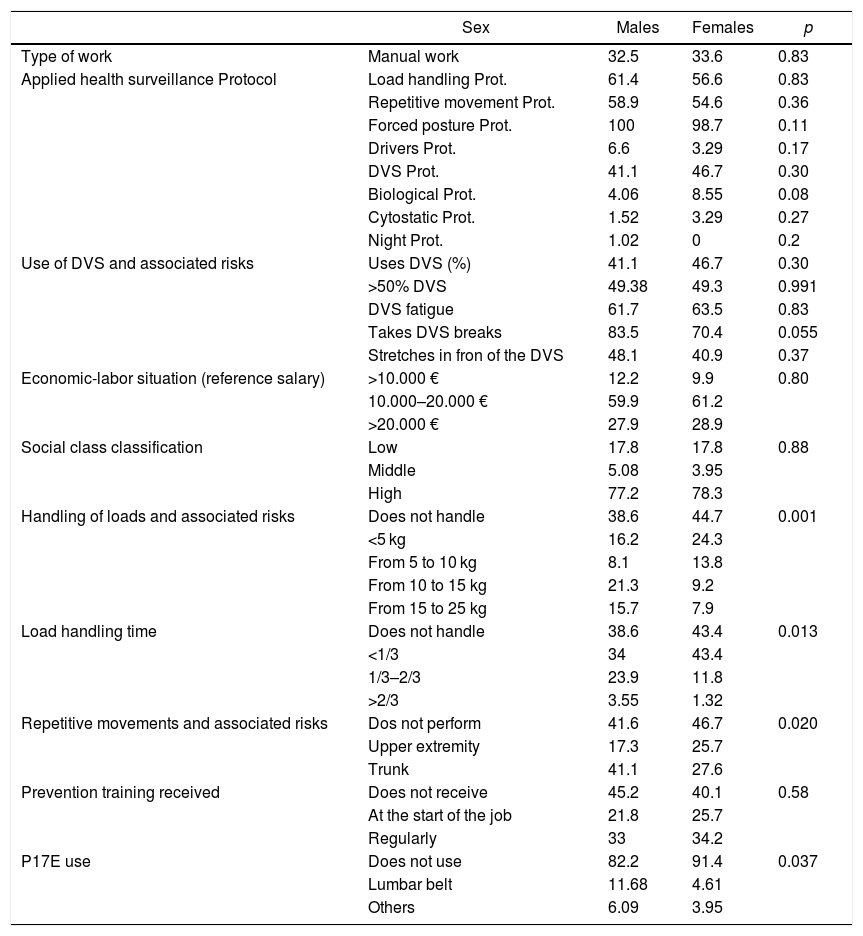
The differences found in the participating population in terms of gender and work variables are illustrated in Table 5.
Percentual relationship of gender with occupational variables.
| Sex | Males | Females | p | |
|---|---|---|---|---|
| Type of work | Manual work | 32.5 | 33.6 | 0.83 |
| Applied health surveillance Protocol | Load handling Prot. | 61.4 | 56.6 | 0.83 |
| Repetitive movement Prot. | 58.9 | 54.6 | 0.36 | |
| Forced posture Prot. | 100 | 98.7 | 0.11 | |
| Drivers Prot. | 6.6 | 3.29 | 0.17 | |
| DVS Prot. | 41.1 | 46.7 | 0.30 | |
| Biological Prot. | 4.06 | 8.55 | 0.08 | |
| Cytostatic Prot. | 1.52 | 3.29 | 0.27 | |
| Night Prot. | 1.02 | 0 | 0.2 | |
| Use of DVS and associated risks | Uses DVS (%) | 41.1 | 46.7 | 0.30 |
| >50% DVS | 49.38 | 49.3 | 0.991 | |
| DVS fatigue | 61.7 | 63.5 | 0.83 | |
| Takes DVS breaks | 83.5 | 70.4 | 0.055 | |
| Stretches in fron of the DVS | 48.1 | 40.9 | 0.37 | |
| Economic-labor situation (reference salary) | >10.000 € | 12.2 | 9.9 | 0.80 |
| 10.000–20.000 € | 59.9 | 61.2 | ||
| >20.000 € | 27.9 | 28.9 | ||
| Social class classification | Low | 17.8 | 17.8 | 0.88 |
| Middle | 5.08 | 3.95 | ||
| High | 77.2 | 78.3 | ||
| Handling of loads and associated risks | Does not handle | 38.6 | 44.7 | 0.001 |
| <5 kg | 16.2 | 24.3 | ||
| From 5 to 10 kg | 8.1 | 13.8 | ||
| From 10 to 15 kg | 21.3 | 9.2 | ||
| From 15 to 25 kg | 15.7 | 7.9 | ||
| Load handling time | Does not handle | 38.6 | 43.4 | 0.013 |
| <1/3 | 34 | 43.4 | ||
| 1/3–2/3 | 23.9 | 11.8 | ||
| >2/3 | 3.55 | 1.32 | ||
| Repetitive movements and associated risks | Dos not perform | 41.6 | 46.7 | 0.020 |
| Upper extremity | 17.3 | 25.7 | ||
| Trunk | 41.1 | 27.6 | ||
| Prevention training received | Does not receive | 45.2 | 40.1 | 0.58 |
| At the start of the job | 21.8 | 25.7 | ||
| Regularly | 33 | 34.2 | ||
| P17E use | Does not use | 82.2 | 91.4 | 0.037 |
| Lumbar belt | 11.68 | 4.61 | ||
| Others | 6.09 | 3.95 |
PPE: personal protection equipment; Prot: protocol; DVS: data visualization screen.
In males, handling of loads of more than10 kg is more frequent and for 2/3 of the workday, whilst in women, the load handled ranges from 5 to 10 kg and for not more than 1/3 of their workday (p < 0.05). In terms of RM, women perform more repetitive tasks of the upper limbs, while men do more repetitive tasks involving the trunk (p < 0.05). Personal protection equipment is more often used by men than by women, particular the lumbar protection belt (p < 0.05).
The distribution of the studied population based on the Oswestry limitation scale is illustrated in a histrogram in Fig. 1, indicating low overall values (<20); however, the multiple lineal regression chart shows a higher impact among the manual workers as compared to the non-manual (2 points in the Oswestry scale, which is significant, Fig. 2).
Discussion

The results of this paper show an association between doing manual work and higher lower back pain disability based on the Oswestry scale, regardless of age and gender.
The study on healthy lifestyles and their relationship with the type of work performed, shows no differences between manual and non-manual workers, except for smoking, with higher tobacco use among the manual workers (p < 0.05). Recent studies specifically show that tobacco use has an impact on particular polymorphic disorders leading to vertebral disc degeneration.25
In our study, pain intensity is higher among manual workers, but the TD impact is stronger among the non-manual workers, particularly women, probably because of decreased physical activities, sitting activities associated with office work or similar activities, as indicated by the NCO. The concern of companies about the impact of low back pain is associated with the number of medical leave days. A Swedish study (Västra Götaland) conducted between 2008 and 2011 reflects an average sick leave of 51 days. The study conducted in Spain in 2011 with data from the National Social Security Institute reported a total of 142.239 low back pain episodes, with a mean duration of 43.51 days and a total of 6.188.626 lost work days.26 Therefore, any initiatives to identify the factors affecting the duration of TD and how to reduce such disability represents an added value, both for the employee and for the company and the society, as evidenced in this study, which reported a duration of low back pain episodes exceeding the standard of the National Institute of Social Security of Spain (18.4 days in average).27
Specifically, in terms of health surveillance, the MHL and RM protocols are used in manual workers, while the DVS protocols are used for non-manual workers. This latter group comprises the younger employees and the most frequent complaint among the white collar workers is fatigue. Health surveillance in Spain is done pursuant to the Law for the Prevention of Occupational Hazards, based on the mandatory requirements and adaptation to risk. Our results surprisingly show that preventive training of manual workers is very low, while it is more comprehensive for the non-manual workers — Article 19 of the Occupational Hazards Protection Law; however, the personal protection equipment is commonly used, particularly the lumbar belt.
In our study, manual workers handle more loads and with a higher frequency, particularly loadbearing the trunk and the upper extremities, but they receive very little preventive information. Consistent with our results, the survey conducted in Quebec shows differences between men and women with regards to the prevalence of occupational musculoskeletal disorders (MSD), some resulting from differences in exposure at the jobsite and with differences when stratified by gender. However, in this study survey, gender was associated with neck lower extremities pain, but not with lower neck pain. The models stratified by gender, nonetheless, identify associations with each result of specific MSD and a range of personal characteristics and physical and psychosocial exposure at the jobsite for men and women. These differences can only be detected via gender stratification which allows for the identification and understanding of a complete range of associations between occupational exposures and MSD.28
The results of our work show that the economic status is better in non-manual workers, but manual workers are typified according to NCO in higher social classes. This approach of quantifying socioeconomic imbalances and relate them to low back pain has been considered by authors from Nordic countries, when examining the impact of labor characteristics on these imbalances, in which the occupational class was used as an indicator of socioeconomic status. In this study, the socioeconomic gradients marked and rated for MSD pain were more significant in males than in females and the relative differences (prevalence ratios) were higher for low back pain, as were the absolute differences (prevalence differences). The demands of physical labor (physical load) accounted for the proportion of the absolute inequalities of the occupational class in terms of low back pain, and provide the authors with the foundation to argue that the workplace may be an important location to implement preventive strategies that reduce the socioeconomic differences that influence pain in MSD.29 Probably the psychosocial factors, in addition to loading and posture, are the most relevant aspects influencing pain symptoms in both occupational groups. Aspects associated with stress control (job-demand-control) and organizational aspects (organizational justice) have been considered in some specific papers as significant predictors among the non-manual workers, also called white collar, and the so called blue collar workers.
The simultaneous exposure to multiple stress factors in the workplace seems to have a synergistic effect on pain symptoms.30 These results are substantiated by the results of other authors who claim that, notwithstanding the differential distribution of occupational demands, white and blue collar workers present similar health complaints and their health was predominantly dependent on the socioeconomic status; hence, the suggestion is that interventions to improve the general health of workers, should start by making an assessment of their socioeconomic status before assessing their work conditions.31 This is consistent with the results of this study which associates poorer economic conditions with manual workers that physically handle more loads and show an increased prevalence of pain.
In our analysis, the overall effect due to limitations is low in all groups, but when assessing individually the different items in the questionnaire, there are differences according to the type of job. Manual workers experience more limitation in ambulation and standing, while the non-manual workers report less load tolerance and more limitations in the sitting position and for traveling. The new technologies have changed work modalities and sedentarism has increased; but working in a sitting and standing position may cause lumbar discomfort, although the recent epidemiological literature fails to support the popular believe that working in a sitting position is associated with low back pain,32 and that a sedentary lifestyle alone is not associated with low back pain (LBP).33 However, other studies support the fact that for sedentary population, changing body posture may lower the possibility of developing low back pain. There are no studies in the literature on specific populations such as those with pre-existing low back pain, or on the rest time required to help reduce pain. In the future, these will be important research topics on low back pain.34 Office (non-manual) workers, prefer alternating between a sitting and a standing position; however, active breaks may be more effective to reduce muscle fatigue.35
The impact of MSD involves a significant burden on society and specific studies have been conducted to assess these disorders; for instance MAPPING, to assess the impact of MSD on HRQOL in the Italian population, although the questionnaires used (SF-36, EUROQoL-5D and CPG) were different from our questionnaire (Oswestry). The MAPPING study indicates that the MSD conditions, including low back pain, have a clearly detrimental impact of HRQOL and enables the comparison between the burden of MSD versus other frequent chronic conditions.36
No differences were observed between both types of workers with regards to the treatment received and its effectiveness on low back pain; however, there are differences based on the age of the worker (with more physical therapy among the youth and combined therapies with medicines in the older population). The objectives of low back pain therapy, particularly chronic pain, are effective pain control, continuous maintenance of physical activity, prevention of permanent disability, and the re-establishment of the ability to work. Analgesics, non-steroidal anti-inflammatory drugs, and muscle relaxants, reduce pain, while multidisciplinary management programs, individualized and guided physical therapy, cognitive behavioral therapy and short training programs, all help to restore function.37
The sizeable and growing literature on low back pain allows for the evaluation of new risk factors and their impact on the prognosis of a disease that is baffling and difficult to control. There are often challenges in the assessment, diagnosis and treatment and the condition is associated with considerable individual distress and a negative social and labor impact. While the review of new and promising strategies is always interesting, most of the new ideas for low back pain care have failed to be effective when subject to rigorous and repeated independent assessment. The new developments in the area of clinical and epidemiological understanding, and the innovative approaches for medical and non-medical medical management seem to offer now the best opportunities to improve the outcomes.38 One of these new approaches is the preventive intervention implemented from the Occupational Health perspective, in which the joint assessment with the public health system may help to obtain more efficient results and optimize the effort deployed and the benefits in terms of potential costs.
The strength of our results is the approach to low back pain from an occupational perspective — particularly preventive — adjusted to the Spanish legislation, in which the
Oswestry test confirms the association between low back limitations and occupational hazards based on the type of work performed. The limitation of the study when assessing the association is the fact that it does take into consideration the causal etiology, and excludes people under 18 years old and over 65. Moreover, since it is a cross-sectional study, it is impossible to ensure time causality. Our data paves the way for further research, so that other prospective trials may confirm this association.
DisclosuresThe authors have no conflicts of interest to disclose.
The following are Supplementary data to this article:
Please cite this article as: Teófila Vicente-Herrero M, Fuentes STC, Espí-López GV, Fernández-Montero A. Dolor lumbar en trabajadores. Riesgos laborales y variables relacionadas. Rev Colomb Reumatol. 2019;26:236–246.
