



The Pellegrini–Stieda sign is a calcification of the medial collateral ligament of the knee after trauma. The presence of symptoms associated with radiological findings is known as Pellegrini–Stieda syndrome. Pain is the main element that characterizes the disease. Treatment ranges from rest, physical therapy, use of NSAIDs, glucocorticoid injection, and even surgery in severe and recalcitrant cases.
El signo de Pellegrini–Stieda es la calcificación del ligamento colateral medial de la rodilla posterior a trauma. La presencia de síntomas asociados a los hallazgos radiológicos se conoce con el nombre de síndrome de Pellegrini–Stieda. El dolor es el principal elemento caracterizador de la enfermedad. El tratamiento varía desde reposo, fisioterapia, uso de antiinflamatorios no esteroides, infiltración con glucocorticoides hasta cirugía, en casos severos y recalcitrantes.
A 51-year-old male patient who 12 years ago presented traumatic twisting of the right knee; a rupture of the anterior cruciate ligament was diagnosed by MRI, which was managed conservatively with NSAID, immobilization and physical therapy with complete resolution of his clinical picture. Five years later the patient began having pain in both knees, mainly in the right, that was exacerbated with physical activity and improved with rest at the beginning of the clinical picture. Subsequently, it became permanent and for this reason various types of NSAIDs were prescribed without having achieved pain control for several years. The patient consulted to Rheumatology where the diagnosis of osteoarthritis of the knees was considered, but in view of the finding of pain localized in the inner side of the right knee.
It was performed a MRI scan that reported: thickened and irregular anterior cruciate ligament with poor definition of its fibers and apparent intrasubstance cicatrization, osteophytes in the medial femorotibial compartment and in the inferior pole of the patella, intrasubstance chondromyxoid degenerative changes of the posterior horn of the medial meniscus; similar findings in the articular cartilage of the medial tibial plateau and the posterior region of the femoral condyle, in addition to the existence of a bone fragment of 11mm in length on the inside of the medial collateral ligament (Fig. 1). With the above-mentioned findings it was considered that the patient coursed with a knee osteoarthritis secondary to traumatic meniscal injury and a Pellegrini–Stieda syndrome (PSS), therefore, it was performed lateral infiltration in the medial collateral ligament, physical therapy, and acetaminophen 1g TID with partial improvement of his pain.

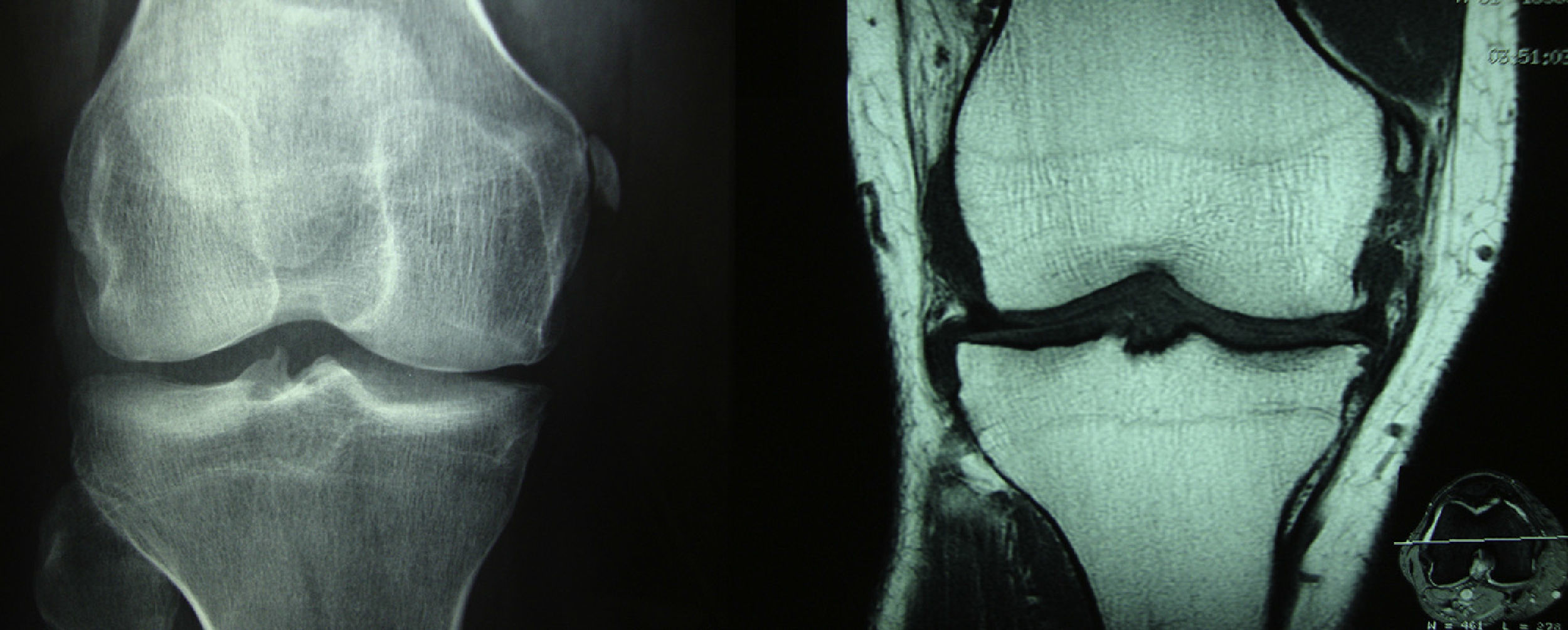
At the left side on the AP radiography of the knees is observed calcification of the medial collateral ligament in its proximal portion, in addition to a decrease in the medial femorotibial space. At the right side in the coronal acquisition with T1 information of the knee becomes evident an ossification in the proximal end of the medial collateral ligament, in relation with an old-injury, configuring a Pellegrini–Stieda lesion. Osteoarthritic changes with formation of marginal osteophytes in the medial compartment are also observed.
Pellegrini in 1905 was the first to describe the sign of Pellegrini–Stieda1 and, subsequently, in 1908 Stieda reported the first series of 5 cases.2 The radiological sign of Pellegrini–Stieda is the proximal calcification of the medial collateral ligament of the knee, after a direct or indirect trauma thereof. The radiological findings plus the clinical symptomatology of pain and restriction in the ranges of motion are known under the name of PSS.3 The incidence of the PSS is unknown, but the preponderance in the male gender between 25 and 40 years of age is clear,4 being rare in children and older people. There is always a relationship with a trauma on the knee or in a distant site such as the skull or the vertebral column,5 but the repetitive traumatic antecedent is not necessary for its appearance. Calcification may occur in the month following the trauma and, in some cases, it has exceptionally spontaneously disappeared.6 The pathophysiology of the disease is also unclear. The trigger for the PSS could be an avulsion of the medial femoral condyle or a tear of ligaments, tendons (ischiocondylar portion of the adductor magnus). It is postulated that soft tissue edema and the subsequent deposition of hydroxyapatite or calcium pyrophosphate is generated after a traumatic injury. The majority of patients are asymptomatic. In the clinical examination can be found pain localized in the medial aspect of the knee and limitation of the flexion–extension movements of the joint. On conventional radiology can be observed a linear or curved calcification that starts from the origin the medial collateral ligament and that may extend almost to the insertion thereof.7 Mendes et al., described 4 types of ossification: I: beak-shaped with inferior orientation and union to the femur, II: drop-shaped with inferior orientation and parallel to the femur, III: elongated with superior orientation, IV: with superior orientation and inferior attached to the femur.8 The treatment of the PSS is usually conservative. Measures such as rest, physical therapy, steroids and lidocaine injections have been successfully used. In severe cases where there is limitation in the movements of damage of the medial collateral ligament, surgical excision of the calcification and ligament repair have been performed with good outcomes. Their removal in early stages of the disease is not recommended because of the high risk of relapse.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors declare they do not have any conflict of interest.
Please cite this article as: Restrepo JP, Molina MP. Síndrome de Pellegrini–Stieda: más allá que un signo radiológico. Rev Colomb Reumatol. 2016;23:210–212.
