





The dorsal wedge calcaneal osteotomy aims to reduce the length of the calcaneus and elevate the insertion of the Achilles tendon, leading to a reduction of Achilles tension in its insertion. The purpose of this study is to assess the clinical and functional results of this osteotomy in patients with insertional Achilles tendinopathy and a high calcaneal inclination angle.
Material and methodsThis is a retrospective study with 18 patients diagnosed with insertional Achilles tendinopathy, who were treated by dorsal wedge calcaneal osteotomy, excision of the wedge and fixation with 2 cannulated screws. The VAS, AOFAS ankle-hindfoot, VISA-A and patient satisfaction scales were performed preoperatively and postoperatively.
The radiological parameters analysed were the calcaneal inclination angle, the calcaneal length and the Fowler–Philips angle.
A statistical analysis was performed.
The mean follow-up was 18.3 months (range 14–36).
ResultsAll patients reported relief from symptoms. The VAS scale improved from 8.25 to 2.16 points; and the AOFAS score rose from 41.5 to 86.5 points (p<.05). The presence of tendon spurs on postoperative X-rays was not related to the clinical improvement.
ConclusionsBased on the results that we present, the dorsal wedge calcaneal osteotomy can be considered an alternative procedure for insertional Achilles tendinopathy in patients with a high calcaneal inclination angle. The symptomatic relief of all the patients might be secondary to the reduction of the tendon tension in its insertion.
La osteotomía calcánea con cuña de sustracción dorsal tiene como objetivo reducir la longitud del calcáneo, elevando la inserción del tendón de Aquiles, reduciendo así la tensión en su inserción por la verticalización del calcáneo. El objetivo del estudio es evaluar los resultados clínicos de esta osteotomía en pacientes con tendinopatía insercional de Aquiles y un ángulo de inclinación del calcáneo elevado.
Material y métodosEstudio retrospectivo de 18 pacientes con diagnóstico de tendinopatía insercional del tendón de Aquiles.
Realizamos una doble osteotomía calcánea en forma de cuña dorsal, exéresis de esta y síntesis con 2 tornillos canulados. Se evaluaron los resultados clínicos-funcionales mediante las escalas EVA, AOFAS, VISA-A y satisfacción del paciente pre- y posquirúrgicas.
Los parámetros radiológicos analizados fueron el ángulo de inclinación del calcáneo, la longitud del calcáneo y ángulo de Fowler-Philips.
Se realizó un análisis estadístico mediante Stata 15.
La media de seguimiento fueron 18,3 meses (rango 14-36).
ResultadosTodos los pacientes presentaron mejoría objetiva de los síntomas y de las escalas EVA (de 8,25 a 2,16 puntos) y AOFAS (de 41,5 a 86,5 puntos) con significación estadística (p<0,05). La persistencia de calcificaciones intratendinosas en las radiografías postoperatorias no influyó en la mejoría sintomática.
ConclusionesCon los resultados obtenidos consideramos que la osteotomía calcánea con cuña de sustracción dorsal es una técnica alternativa válida en el tratamiento de la tendinopatía insercional de Aquiles, sobre todo en los casos con un ángulo de inclinación del calcáneo elevado.
Dorsal wedge calcaneal osteotomy was described by Zadek for the treatment of Achilles bursitis in 1939 and was later popularised by Keck and Kelly for the treatment of the Haglund triad or syndrome (insertional Achilles tendinopathy [IAT], Haglund's disease and retrocalcaneal bursitis).1–3 Despite being a standard technique, the results published in the literature with this technique for the Haglund triad or for IAT are still practically non-existent.
The technique described by Zadek for Achilles bursitis consists of resection of the bursa and an osteotomy with incomplete dorsal wedge at plantar level, with osteoclasia on removing the wedge. The osteotomy closure is performed through the tendon and the periosteum. The objective was to reduce the length of the calcaneus and elevate the insertion of the Achilles tendon (Fig. 1).

The dotted lines show the dorsal wedge calcaneal osteotomy for the Haglund triad. The purpose of this osteotomy is to elevate the point of insertion of the Achilles tendon and anteriorise posterosuperior tuberosity of the calcaneus. Shortening of the calcaneus and elevation of the point of insertion of the Achilles tendon reduces the pressure on the Achilles tendon insertion.
This study modifies the technique initially described on completing the plantar osteotomy and synthesizes it with 2 cannulated pins.1
The aim of the study was to analyse clinical, functional and radiological outcomes of the Zadek osteotomy modified in patients with insertional Achilles tendinopathy.
Materials and methodsLevel IV. Retrospective case series (iv).
Observational retrospective study of 18 patients who presented with posterior talalgia located in the insertion of the Achilles tendon.
The mean age of the patients was 49 years, 11 of them were women. All of them were diagnosed using nuclear magnetic resonance (NMR) of the IAT. Tendinous calcifications were observed in the X-rays and in the NMR of all of them.
Prior to surgery, all patients were treated conservatively for a minimum of 6 months with anti-inflammatory therapy, insoles and/or alterations to footwear and physiotherapy (extrinsic exercises of the triceps surae) with no improvement of symptoms.
Inclusion criteria (should meet with 3):
- –
Clinical: clinical signs of the IAT.
- –
NMR: signs of IAT in NMR.
- –
Radiography: inclination angle of the calcaneus in a lateral X-ray of the weight-bearing foot equal to or above 20°.
Exclusion criteria were patients with:
- –
Clinical signs of non-insertional tendinopathy or of the body of the Achilles tendon.
- –
Neurological pes cavus.
Patients with suspected neurological pes cavus with possible paralysis of triceps surae (diagnosed using an electromyogram) were excluded as it was considered that they would not benefit from the technique described despite having an inclination angle of elevated calcaneus.
The lower limit for indication of this osteotomy used was a radiological inclination of the calcaneus of 20°, with raised angles considered to be from this figure upwards, according to the literature.4,5
Surgical techniqueUnder intraspinal anaesthesia and with the patient in decubitus contralateral to the limb to be operated on, a lateral oblique approach was taken, avoiding the sural nerve, close to the via. The aim of dorsal wedge calcaneal osteotomy is to advance insertion into the posterior tuberosity of the Achilles tendon calcaneus. The first osteotomy is posterior to the subtalar articulation and perpendicular to the weight-bearing surface area. The second osteotomy, 1cm behind the first, is performed to create the dorsal wedge base. The vertex of the osteotomy is completed and located anterior to the plantar tuberosity. Following removal of the wedge, synthesis is performed with 2 6.5mm cannulated pins.
All the patients were immobilised with a 90° brace for 3 weeks, with weight-bearing being authorised with a Walker type boot in the 3rd week and the brace being removed from postoperative week 6.
The American Orthopaedics Foot and Ankle Society Ankle-Hindfoot (AOFAS) scale, the visual analogue scale (VAS), the Victorian Institute of Sports Assessment-Achilles questionnaire (VISA-A) and patient satisfaction were assessed preoperatively and after 6 and 12 months postopratively.6,7
The VISA scale was initially described in 1998 by the Tendinopathy Study Group of the Victorian Institute of Sports Assessment for patellar tendinopathy.8 It was subsequently applied to the Achilles as the VISA-A scale, a reliable tool for assessment of Achilles tendinopathy.9
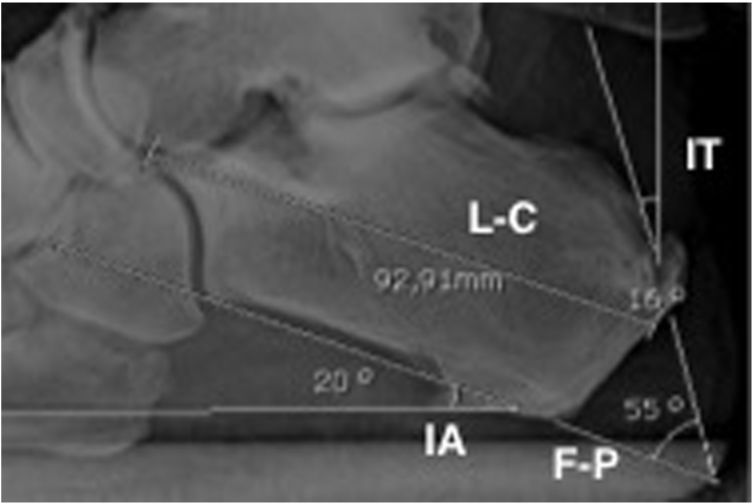
The radiological parameters assessed were (Fig. 2):
- 1.
Calcaneal inclination angle: angle between the plantar surface area of the calcaneus and the apex parallel to the ground.10
- 2.
Fowler–Phillips angle: formed between the posterior surface and the plantar surface of the calcaneus.11
- 3.
Calcaneus length: measured from the most posterior point and the most distal/anterior point of the calcaneus.
- 4.
Tuberosity inclination angle: defined as the angle between the posterior surface of the posterior tuberosity and the apex perpendicular to the ground.
 was 21.9°. The mean of the Fowler–Phillips (F–P) angle preoperatively was 53.2° and was reduced after surgery. The length of the calcaneus (L-C) lowered after surgery by a mean of 4.8mm. The tuberosity angle inclination (TI) increased after the osteotomy, because the tuberosity was displaced forward.")
The mean of the inclination angle of the calcaneus (IA) was 21.9°. The mean of the Fowler–Phillips (F–P) angle preoperatively was 53.2° and was reduced after surgery. The length of the calcaneus (L-C) lowered after surgery by a mean of 4.8mm. The tuberosity angle inclination (TI) increased after the osteotomy, because the tuberosity was displaced forward.
Radiological parameters were analysed prior to surgery and 6 and 12 months after surgery. Measurements were made by 3 different surgeons, 3 different times for each, separated in time, and aimed at minimising any possible intraobserver and interobserver bias. The mean of the 3 observations was calculated.
Level of postoperative satisfaction was defined as highly satisfactory, partially satisfactory and unsatisfactory and patients were asked whether they would recommend surgery to a family member or a friend.
Statistical analysis of results was performed with Stata 15 (paired Student's t-test), once normal distribution had been verified (using the Kolmogorov–Smirnov test) of study variables. Differences were considered statistically significant when p<.05.
Mean follow-up was 18.3 months (range 14–36 months).
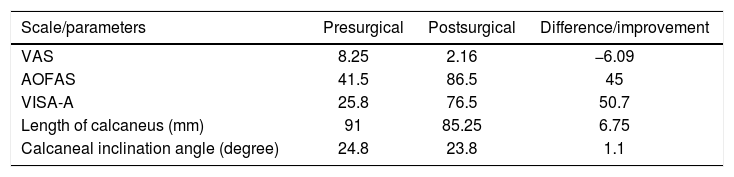
ResultsClinical and functional resultsAll patients improved their score on the visual analogue pain scale after surgery, from 8.25 points preoperatively to 2.16 points postoperatively (p<.01). Hindfoot functionality improved, with an increase in the AOFAS and VISA-A scales one year after the operation of 45 points (p<.01) and 50.7 points (p<.01), respectively (Table 1).
Clinical and functional results.
| Scale/parameters | Presurgical | Postsurgical | Difference/improvement |
|---|---|---|---|
| VAS | 8.25 | 2.16 | −6.09 |
| AOFAS | 41.5 | 86.5 | 45 |
| VISA-A | 25.8 | 76.5 | 50.7 |
| Length of calcaneus (mm) | 91 | 85.25 | 6.75 |
| Calcaneal inclination angle (degree) | 24.8 | 23.8 | 1.1 |
AOFAS: American Orthopaedic Foot and Ankle Society Ankle-Hindfoot score; VAS: visual analogue scale of pain; VISA-A: Victorian Institute of Sports Assessment-Achilles questionnaire.
Length of calcaneus: measurement of the total length of the calcaneus in radiography.
Postoperative improvement on the VAS scale and on the AOFAS and VISA-A scales was statistically significant (p<.01). The difference in calcaneus length (shortening) was statistically significant (p<.025).
There was no statistically significant difference (p>.05) between the preoperative calcaneal inclination angle which was 24.8°, and the postoperative angle which was 23.8°.
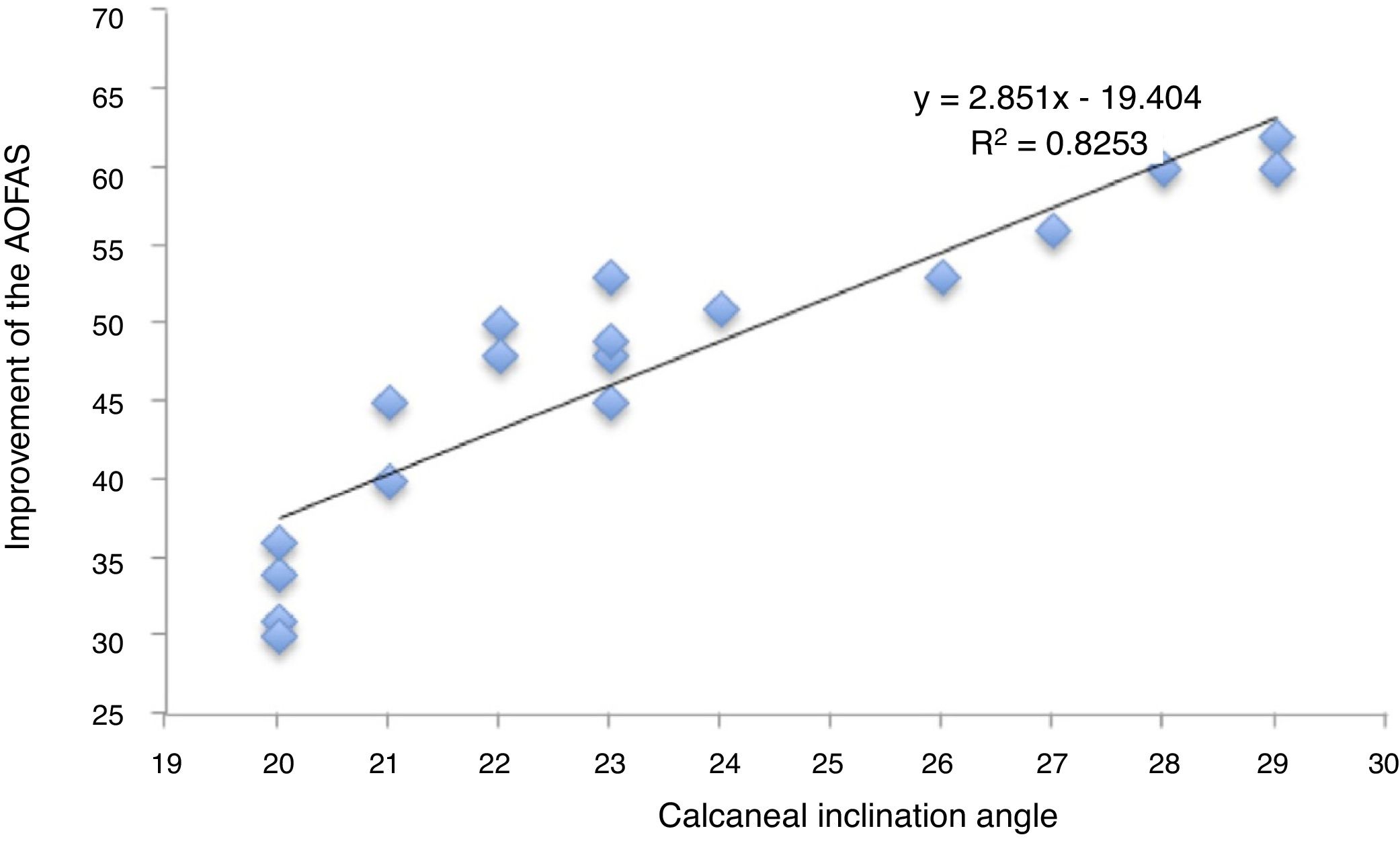
The patients with a greater angle of calcaneal inclination prior to surgery presented with better postoperative functional results (AOFAS and VISA-A) results. In contrast, cases with an angle close to the indicated limit (20–21°) presented with a lower postoperative score on the functional assessment scales. The ratio between the calcaneal inclination angle and the improvement on the AOFAS scale (y=2.851x−19.404, R2=.8253) was statistically significant (Fig. 3).

The Fowler–Phillips angle mean was 53.2° preoperatively (range: 49.1–53.7°); and dropped to 37.4° postoperatively (range 32.8–42).
The mean length of the presurgical calcaneus was 90.23mm (range: 85.31–95.01) and postsurgical was 85.41mm (range: 80.4–90.4mm), with mean shortening of the calcaneus of 4.81mm (p<.01).
Tuberosity inclination angle prior to surgery was 16.4° and rose to 32.4° after osteotomy, due to the anterior transfer of tuberosity (p<.001).
Insertional intratendinous calcifications visible on X-rays prior to surgery were not surgically resected but remained until the end of follow-up (Fig. 4). The persistence of calcination did not correlate with clinical improvement.
Satisfaction
Fifteen of the 18 patients (83%) stated that they would recommend surgery to a family member or a friend who had the same problem.
These same 15 patients rated their outcomes as highly satisfactory. The remaining 3 patients were partially satisfied and there were no unsatisfied patients.
ComplicationsAll the complications were minor. There were 2 cases with sural neuritis symptoms which were spontaneously resolved and one case of a delayed wound healing.
In 2 cases we observed a proximal migration of posterior tuberosity of the calcaneus, secondary to the performing of a complete plantar osteotomy. This migration in both cases was under 5mm with respect to the cortical plantar, with no correlation with poorer clinical or functional outcomes.
No relapses occurred.
DiscussionThe aetiology and pathogenesis of the IAT is still unknown. However, several factors, such as hindfoot alignment (pes cavus) could impact the mechanics of the foot.12 For this reason the osteotomy described in this study is one option for the treatment of IAT secondary to vertical calcaneus or with an inclination angle of elevated calcaneus.
There are many surgical procedures described for the treatment of IAT, including debridement of the degenerative tendon together with de-insertion and reinsertion with bone anchorage; the increase with the flexor hallucis longus tendon; calcaneoplasty or exostectomy; removal of the retrocalcaneal bursa and calcaneal osteotomy. Although debridement and exostectomy are more standard techniques no consensus or therapeutic algorithm has yet been reached regarding the best surgical technique.
The literature published on treatment for IAT with Zadek's isolated osteotomy is scarce. Georgiannos et al. published the results of a retrospective study in 64 athletes treated with this technique, but this was combined with a second osteotomy of Haglund tuberosity (exostectomy) to the calcaneal osteotomy.10,13
Comparative studies with other more standard techniques are scarce and have small sample sizes. Taylor presented the comparative results of a Zadek osteotomy with that of posterosuperior calcaneal tuberosity resection,14 obtaining favourable results in both groups but without any statistically significant differences.
With regard to surgical techniques, Boffelli et al. described the importance of performing the first osteotomy perpendicular to the plantar surface to rotate posterior tuberosity. However, in their technical description, the vertex of the wedge was proximal to the calcaneal plantar tuberosity.15 Our technique differs to these authors, as we consider the vertex of the distal osteotomy to the plantar tuberosity, to avoid a biomechanical overload at osteotomy site and particularly during supported walking stages.
Regarding wedge thickness, the literature mentions the extraction of the dorsal base wedge of 7–15mm.1,16 The wedge extracted in this study was similar in all cases (1cm approximately). However, the fact that differences were obtained in the shortening of the calcaneus could be secondary to technique errors such as: a variation in the size of the saw cut, different inclination of the osteotomy or minor differences in wedge measurement. This bias was useful in identifying a statistical correlation between the shortening of the calcaneus and postoperative functional improvement (AOFAS y VISA-A), concluding that the larger the wedge removed, the better the functional results.
According to Maynou et al., referral for a complete or incomplete osteotomy at cortical plantar level would depend on the calcaneal inclination angle.16 In our study, we considered that incomplete osteotomy could be the cause of a secondary fracture on closure, and it was therefore decided to complete the osteotomy in all cases.
Similarly, to Watson et al., we believe that a calcaneal inclination angle above 20° would be the only preoperative radiographic parameter to consider for osteotomy referral, and that the Fowler–Philips angle may not be necessary since it does not affect the process of taking clinical decisions.4
The shortening of the calcaneus minimises the posterior lever arm of the gastrocnemius-Achilles-calcaneal system and could be beneficial for patients with excessive Achilles insertional pressure.
ConclusionsZadek type dorsal wedge calcaneal osteotomy is a surgical technique to consider in patients with IAT and an elevated calcaneal inclination angle (above 20°). This surgical procedure in selected patients has favourable clinical and functional outcomes and is considered a valid alternative in the IAT therapeutic algorithm.
By extracting a dorsal base calcaneal wedge, we raise the point of insertion of the Achilles tendon, displacing posterior tuberosity, we shorten the calcaneus and improve the posterior lever arm and tendon pressure on insertion, thereby lessening the pain in Achilles tendon insertion.
LimitationsThe main limitations of this study are that it is an observational study with retrospective data collection and a small sample size. However, results are similar to those described in the literature.
Randomised prospective studies with group control or comparisons with other techniques are required to obtain outcomes with a higher statistical consideration.
Level of evidenceLevel of evidence IV – Case series.
Conflict of interestsThe authors have no conflict of interests to declare. The authors did not receive any financial help, did not sign any agreements whereby they received benefits or fees from any commercial entity, nor did they receive any specific subsidy from public sector, private sector or non-profit-making entities.
Please cite this article as: López-Capdevila L, Santamaria Fumas A, Dominguez Sevilla A, Rios Ruh JM, Pich Aguilera E, Boo Gustems N, et al. Osteotomía calcánea con cuña de sustracción dorsal como tratamiento quirúrgico en la tendinopatía insercional de Aquiles. Rev Esp Cir Ortop Traumatol. 2020;64:22–27.
