



The purpose of this work is to study the epidemiology of patients with distal humerus supracondylar fractures in pediatric age treated in a tertiary hospital.
MethodA descriptive study was conducted on the epidemiological characteristics of distal humerus supracondylar fractures in pediatric patients treated in a tertiary hospital from January 1, 2014 to June 30, 2018. The following variables were analyzed: age, side of lesion, sex, type of Gartland’s classification, date of injury, mechanism, place and moment of trauma, therapeutic attitude, complications and associated fractures.
ResultsA total of 140 patients were included in the study, with an average age of 5 years and 3 months. According to Gartland’s classification, 40% of patients with type I fractures were found, 20.7% with type II and 39.3% with type III. Of the total sample, 76 patients (54.3%) were treated surgically and 9 (6.4%) had neurological complications. Likewise, in 135 cases the place of the fall could be identified, most of them (52.1%) in the park with a significantly higher incidence from May to August (45.8%) and the weekends (70.71%).
ConclusionsThe incidence of supracondylar humerus fractures seems to be greater associated with the activity in the parks and, above all, it would be greater during the summer period, in the afternoon and the weekends.
La finalidad de este trabajo es estudiar la epidemiología de los pacientes con fracturas supracondíleas de húmero distal en edad pediátrica atendidos en un hospital terciario.
MétodoSe realizó un estudio descriptivo sobre las características epidemiológicas de las fracturas supracondileas de húmero distal en pacientes pediátricos atendidos en un hospital terciario desde el 1 de enero de 2014 hasta el 30 de junio de 2018. Se analizaron las siguientes variables: la edad, el lado de la lesión, el sexo, el tipo de la clasificación de Gartland, la fecha de la lesión, el mecanismo, el lugar y momento del traumatismo, la actitud terapéutica, las complicaciones y las fracturas asociadas.
ResultadosEn el estudio fueron incluidos un total de 140 pacientes, con una edad promedio de 5 años y 3 meses. Según la clasificación de Gartland, se encontró un 40% de pacientes con fracturas tipo I, un 20,7% tipo II y un 39,3% tipo III. Del total de la muestra, 76 pacientes (54,3%) fueron tratados quirúrgicamente y 9 (6,4%) tuvieron complicaciones neurológicas. Asimismo, en 135 casos se pudo identificar el lugar de la caída, predominando en el parque (52,1%) con una incidencia significativamente más alta de mayo a agosto (45,8%) y los fines de semana (70,71%)
ConclusionesLa incidencia de fracturas supracondíleas de húmero en niños parece estar asociada fundamentalmente a la actividad en los parques y, sobre todo, ésta sería mayor durante el período estival, por las tardes y los fines de semana.
Distal humerus supracondylar fractures are one of the most common fractures in paediatric ages, with a peak of maximum incidence between the ages of 6 and 7 years.1 There are several classifications to describe these fractures and guide their treatment, but the most used in daily clinical practice is Gartland’s classification. The most common mechanism of occurrence is indirect, a fall with the elbow extended, displacing the distal fragment in posteromedial direction. Non- displaced fractures or those with a minimal displacement may be treated conservatively, but when displacement is severe or there is rotation or vascular or nerve compromise they should be stabilised with surgery. Neurovascular complications are the most severe complications, with a frequency of between 5% and 19% of displaced fractures, due to the proximity of structures such as the brachial artery and anterior interosseous nerve.2 They are often combined with fractures of the radius and distal ulnar, at a lower percentage rate.3 The most common complications are varus or valgus deformities of the elbow and mobility limitations.
Increases in the frequency of fractures have usually been associated with holiday periods and leisure activities in the park. However, few studies have scientifically demonstrated these events.4 For this reason the objectives of this article were to:
- –
Study the characteristics of these patients; lesion mechanisms; degrees of fractures according to the Gartland’s classification; the therapeutic attitude and incidence of any complication and associated fracture, during a period of 4.5 years treated in a tertiary hospital.
- –
Determine the time of year, time of day and day of the week when the incidence of supracondylar fractures of elbows in children increase.
- –
Studying the epidemiology of this type of fracture could help to guide paediatricians, traumatologists, physiotherapists and carers with regards to the therapeutic approach to be followed in these situations and improve primary prevention in the future.
This descriptive, observational and retrospective study includes all patients under 15 who were attended for supracondylar fractures of distal humerus in the Outpatients Department of a tertiary hospital during a 4.5-year period (1st July 2014–30th June 2018). Data were collected from the electronic clinical files and the picture archiving communications system (PACS) with respect to age, gender, affected side, date, time and day of the lesion, type of Gartland’s classification, mechanism, therapeutic approach, complications and associated fractures.
The criteria followed for treatment indication were: type I and type II fractures which did not require reduction were treated conservatively; type II fractures required closed reduction, type III fractures and those in flexion treated with closed reduction +/– fixation with percutaneous Kirschner pins, reserving open reduction for irreducible fractures.
To assess the function of the elbows in patient follow-up after treatment a goniometer was used to measure the digress of flexion, extension and pronosupination. Similarly, a goniometer was used to assess possible residual deformity in valgus or varus, measuring the degrees of the humerus-radius-ulnar angle and comparing them with the contralateral elbow.
Statistical analysis was performed with the BM SPSS Statistics programme, version 22. The alpha significance level considered was .05. Descriptive statistics was performed (mean, standard deviation, confidence interval [CI]). The non parametric Chi test or the Pearson test was used to confirm separation or non separation of the different variables from one another.
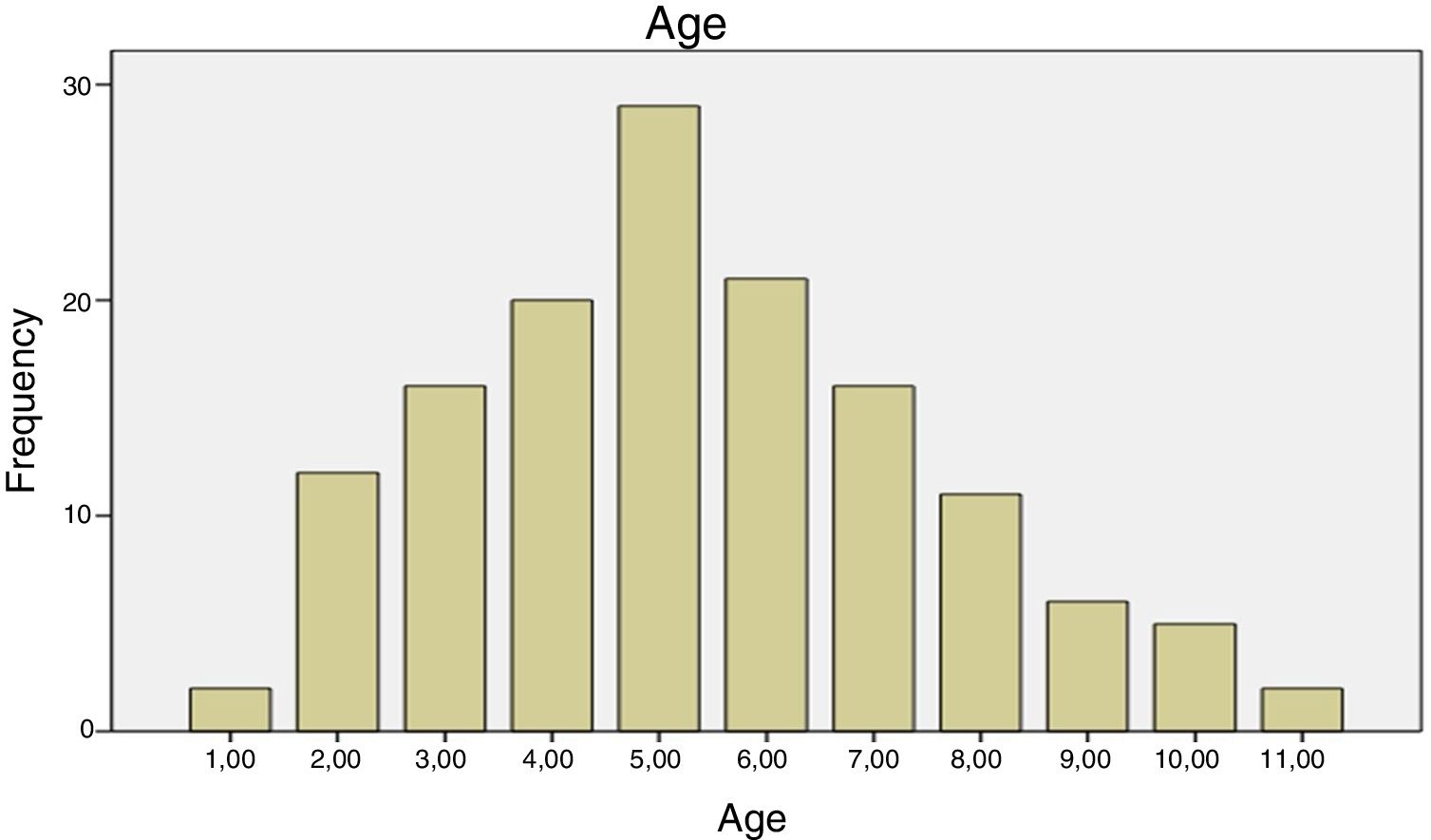
ResultsFollowing the application of inclusion criteria, data from a total of 140 patients were analysed, with a mean age of 5 years and 3 months (1–11; 95% CI, 5–5 m,7) (Fig. 1).

Sixty nine (49.6%) patients were male and 81 fractures (57.9%) occurred on the left side. No statistically significant differences were found between males and females, nor fracture side. There were no simultaneous bilateral lesions, although there was one case of a fracture in both elbows with a differential period of 2 years. Only one fracture was by flexion mechanism (.7%). No statistically significant differences were found between gender and flexion/extension lesional mechanism. Out of the 140 lesions, 40%, 20%, 7% and 39.3% of the fractures were type I, II and III of Gartland’s classification, respectively. All fractures were closed.
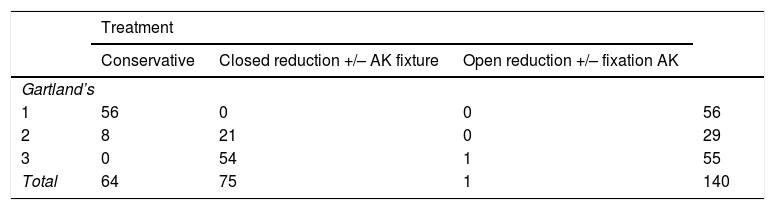
Seventy six patients (54.3%) were surgically treated. All Gartland’s type III fractures (55 fractures) were treated using reduction and fixation with percutaneous Kirschner pins. Only in one case of this group was it necessary to perform open reduction. Twenty one of the Gartland’s type II (72.4%) fractures required manipulation under general anaesthesia with or without fixation with Kirschner pins. Therefore Table 1 shows the association between the type of fracture and the treatment carried out (Pearson Chi-square [4] = 109.332; p < .001).
Association between type fracture type according to Gartland’s classification (severity) and type of treatment used.
| Treatment | ||||
|---|---|---|---|---|
| Conservative | Closed reduction +/– AK fixture | Open reduction +/– fixation AK | ||
| Gartland’s | ||||
| 1 | 56 | 0 | 0 | 56 |
| 2 | 8 | 21 | 0 | 29 |
| 3 | 0 | 54 | 1 | 55 |
| Total | 64 | 75 | 1 | 140 |
Pearson Chi-square (4) = 109.332; p < .001.
Among the patients who required fixation with Kirschner pins (70), in 50 cases (71.4%) treatment with 2 lateral pins was sufficient. In 16 cases fixation with medial pins was necessary, pointing out that, in one of them, the lesional mechanism of which was by flexion, 3 lateral pins were inserted and one medial and in another case, which was not operated on in our hospital, fixation with 2 medial and 2 lateral pins was necessary.
The medical histories of 9 patients (4.9%) recorded the detection of neurological compromise, either on initial examination or after treatment. All the patients with neurological lesions presented with Gartland’s type III fractures. Seven patients presented with a median nerve paresis, which was present since examination in the emergency unit. One of the patients presented with paralysis of the median nerve and of the ulnar nerve associated with the introduction of a medial Kirschner pin. In our series, there was only one isolated nerve lesion of the radial nerve. The majority of children recovered elbow function between the first and second month after surgery. Only in one of the cases was recovery delayed until 6 months. In our series no medical history included any cases of vascular compromise (absence of pre/post reduction pulse), or compartmental syndrome. Four of the patients included in the study (2.8%) presented with changes to the consolidation in the humerus-radial-ulnar axis, comparing clinically with the contralateral side measured with a goniometer. These changes in axis did not require any surgical treatment.
Finally, one patient presented with a loss of reduction immediately after surgery which required a further operation for closed reduction and fixation with pins. However, despite the whole procedure, they did not present with any vascular or neurological complications. Therefore, our study did reflect a statistically significant association between the severity of the fracture and the complications which could present during the patient’s evolution (Pearson Chi-square [6] = 22.17; p = .01).
In our series, the association of supracondylar fracture of the elbow with a fracture of the forearm only occurred in 4 patients (2.8%), with surgical treatment being necessary using fixation with pins at wrist level on a single occasion. However, no significant association was observed between the severity of the fracture, according to Gartland’s classification and the associated fractures (Pearson Chi-square [4] = 5.045; p = .283)
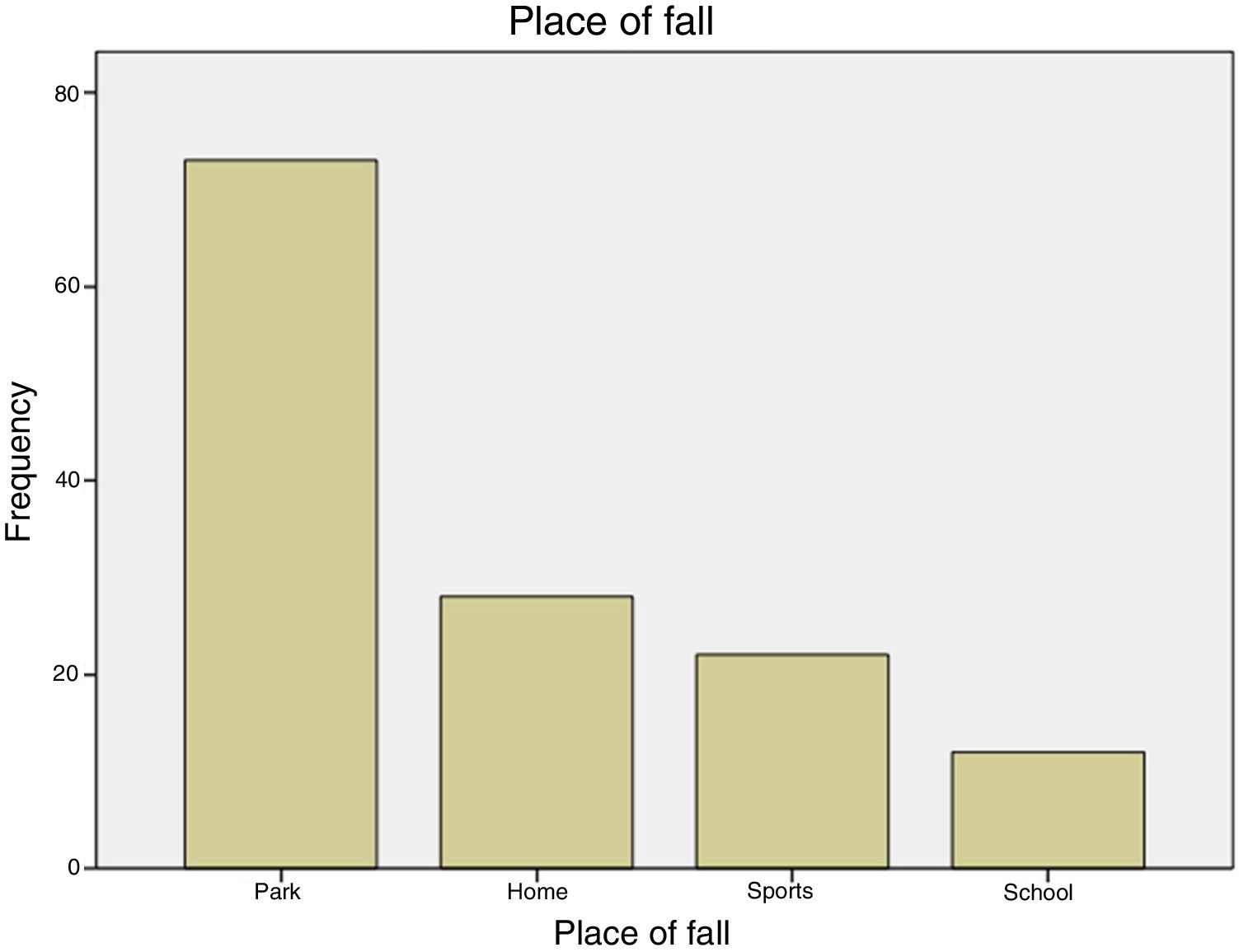
The place where the trauma occurred was included in the medical history of 135 patients (95.74%). Most fractures (52,.%) happened in the park, but it is difficult to pinpoint what type of game was involved since this is not reflected in the electronic medical file. Twenty per cent of fractures occurred at home, in falls from tables, chairs, sofas or beds. 16.29% of falls were related to accidents when playing sports, mostly falls from playing football. Lastly, only in 12 cases (8.8%) did the fall occur at school (Fig. 2). There was no statistically significant association between the severity of the fractures, according to Gartland’s classification and the place where they happened (Pearson Chi-square [6] = 5.423; p = .491).

With regard to the time of day when the falls occurred and were attended in the emergency unit, this was recorded in 133 cases. The period between 3 pm and 10 pm stands out, encompassing 60.71% of fractures. Considering that classes in our area are from 8:00 until17:00 h, 67.66% of fractures happened outside school hours. However, there was no statistically significant association between the type of Gartland’s and the time of day (morning, afternoon or evening) when the fall occurred (Pearson Chi-square [4] = 1.705; p = .790).
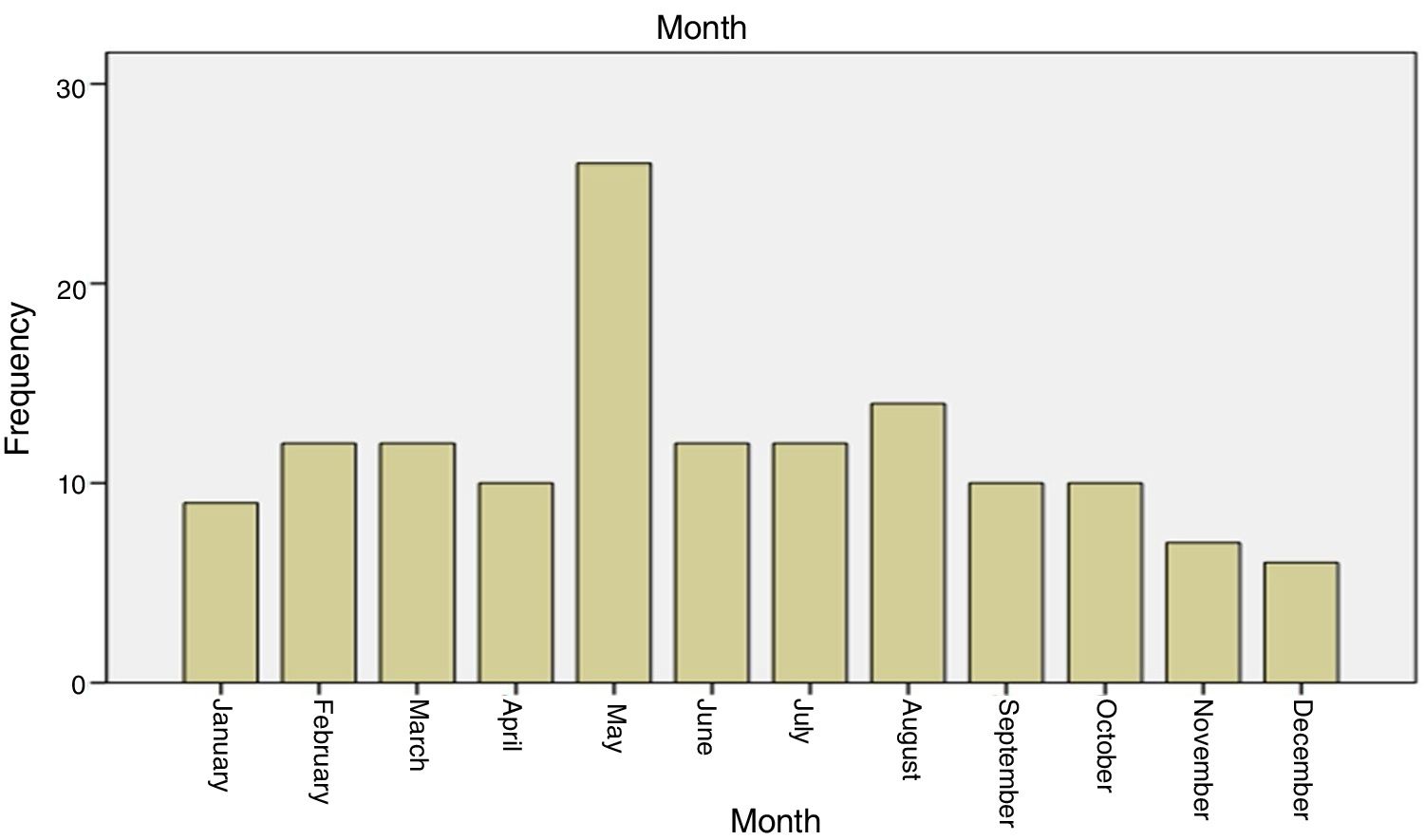
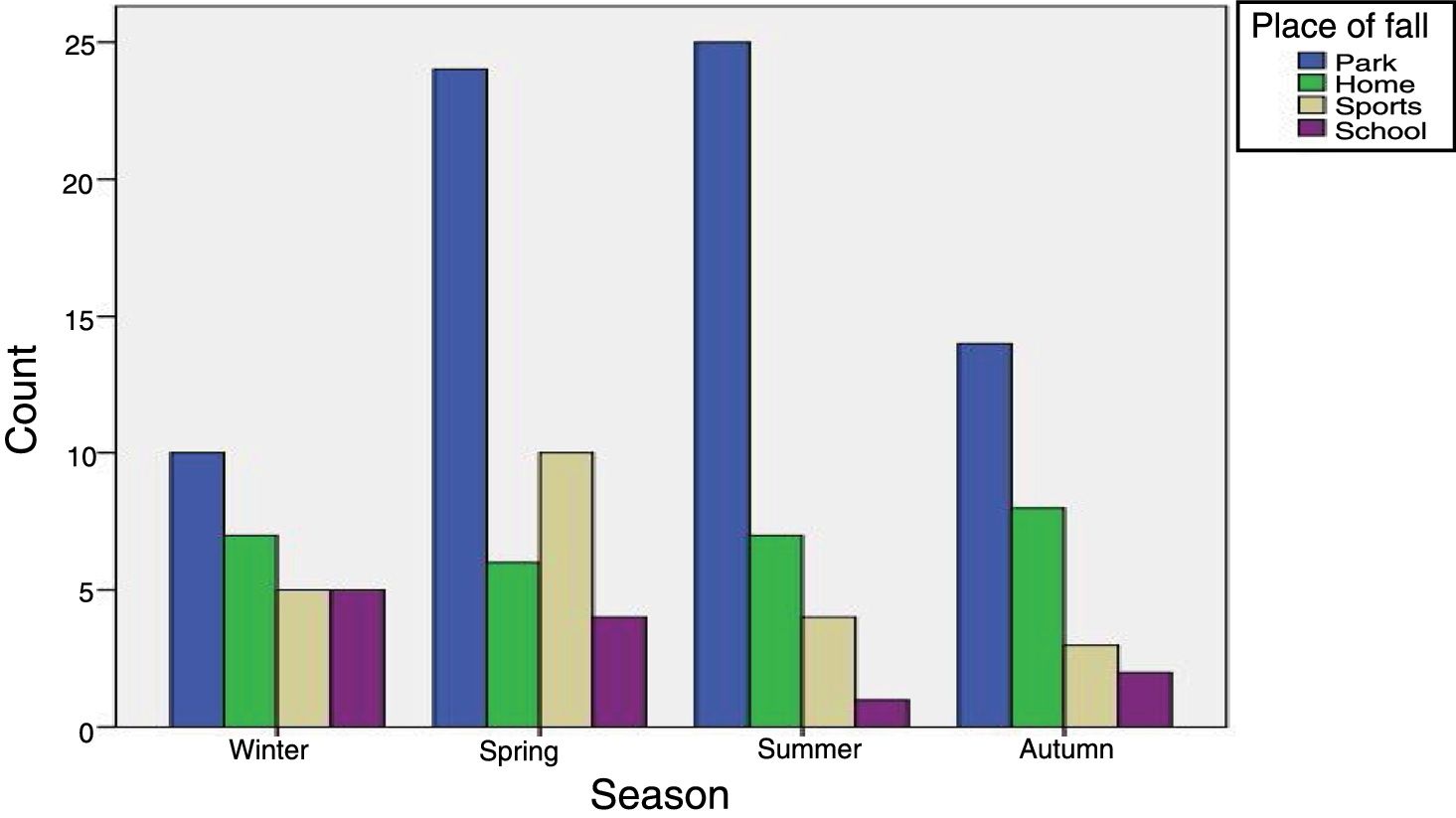
One hundred and twenty seven patients were identified in the school age cohort (between 3 and 11 years old). Sixty nine fractures occurred during the period between May and September. The average amount of falls during the end of Spring and Summer was higher than during Autumn and Winter, with a higher incidence in May compared with the other months, at a rate of 18.43% fractures (Figs. 3 and 4).


Finally, the day of the week in which the fracture took place was considered and a study was made of which days the highest incidence of this type of fractures was recorded. Friday, with 34 fractures, was the day of the week when most fractures occurred. During the week-end, from Friday to Sunday, 51.4% of fractures were recorded. If we include the early morning of Monday in the register, this percentage would increase to 70.71%. The rate of fractures recorded was therefore significantly higher during the week-end than the rest of the week.
DiscussionThe peak of the rate of supracondylar fractures of the humerus in paediatric age reported in the literature is around 6 years of age. However, in our series this peak occurred at a slightly earlier age (5 years) (Fig. 1). In our study, no predominance of the male sex or laterality described in other series was observed.1,5 Regarding the severity of the fractures, Gartland’s type I fractures predominated, followed by type III. This data is not constant in previously published studies. This variability in type of fracture according to Gartland’s classification may reflect the differences in the level of energy of the activity between the different populations studies or currently higher radiological diagnosis of non-displaced fractures.4 The majority of the supracondaylar fractures in our series were fractures caused by indirect mechanism in extension, similarly to the other published studies.6,7
In the cohort studied, all the type iii fractures and the majority of type II fractures (72.4%) were treated with closed reduction with /without pins, which shows that, the more severe the fracture, the more aggressive the therapeutic approach tends to be. Similarly when a fracture is more displaced the number of complications increases significantly.2,8–12 Of the 84 fractures displaced in extension, a neurological deficit was reported in 9 patients (10.71%), most of which related to the median nerve. All the cases presented with complete recovery after 6 months. Caso-García et al.10 conducted a retrospective study in 188 children with displaced supracondylar fractures of distal humerus. They reported 28 cases (15%) of neurological lesions, with the most frequent being the neuroapraxia of the median nerve. Recovery was spontaneous in all patients in a period under 6 months, similarly to our study. Juan-García et al.11 presented a retrospective study of 130 children treated surgically for displaced supracondylar fractures of distal humerus. The most commonly affected nerves, after surgical treatment, were the median (5 cases) and the ulnar (5 cases), with neuroapraxia resolved in 6 months except in one case. In the study by Díaz-Borjón et al.12 a total of 50 patients with Gartland’s type II and type II supracondylar fractures of the humerus were presented, who had been surgically treated using cross-pin (27 patients) and lateral fixation (23 patients). Six cases of ulnar nerve lesion were found in the group of children operated on with Kirschner cross pins, and it was therefore recommended that the medial epicondylitis be sufficiently palpated to avoid this complication. In our series only one patient presented with iatrogenic ulnar nerve paralysis and they also evolved favourably with spontaneous recovery. In the study by Caso-García et al., involving 188 children with for displaced supracondylar fractures, 23 cases presented with varus of the elbow deformity sequalae (12%). In our series the incidence of this complication was considerably lower: only 4 patients presented with longitudinal deviations of the axis of the elbow, possibly due to an improvement in reduction techniques and stabilization of fractures in recent years.
There are few studies to be found in the literature dealing with the epidemiology of this type of fractures. The most outstanding point is the fact that the most frequent falls occur in the pack rather than in other places.4 In our series, this was confirmed, since 52,.% of falls occurred in the park, followed by falls in the home and during sports, with similar percentages in the last two. It is of note that the home is not a protection factor against fractures, at least not in our series. The least frequent setting for falls leading to supracondylar fractures of the elbow in children is at school. This fact should be noted with precaution since possible bias may exist due to the use of private medical insurances in several grant-maintained and private schools.
Of the 127 patients of school age in our study, 69 fractures took place between May and September, with a peak of incidence in the month of May, probably linked to the increase in the number of children going to the park due to better weather conditions.
Regarding the time of day the highest number of falls was recorded between 15.00 h and 22.00 h (60.7%), i.e. in the afternoon/evening and mainly on week-end days.
Our final point shown by this study is that falls mostly increase at week-ends and from the end of spring onwards, coinciding with summer holidays and better weather conditions. However, Little can be done to reduce the higher incidence at these times, apart from primary preventative measures. These would involve optimising conditions in parks, where most falls occur, and ensuring appropriate supervision of games.13 This could be significant in reducing supracondylar fractures of the elbow in children.14,15
ConclusionIn this study analytical documentation was made on the epidemiology of paediatric supracondylar humerus fractures treated in a tertiary hospital during a period of 4.5 years. It reflects statistically significant results regarding the association between the complexity of the lesion and a higher rate of complications and a more aggressive therapeutic approach.
The results also indicate that activities taking place in centres of leisure such as parks are associated with a higher rate of fractures, and measures need to be taken from the point of view of primary prevention to prevent or at least reduce these fractures. As expected, the rate of patients with distal humerus supracondylar fractures in paediatric age is significantly higher during holiday periods, the summer months and the week-ends, which coincide with days when there is no school
FinancingFinancing was provided by the Orthopaedic and Traumatology Service.
Conflict of interestsNone.
Please cite this article as: Aparicio Martínez JL, Pino Almero L, Cibrian Ortiz de Anda RM, Guillén Botaya E, García Montolio M, Mínguez Rey M F. Estudio epidemiológico sobre fracturas supracondíleas de húmero distal en pacientes pediátricos. Rev Esp Cir Ortop Traumatol. 2019;63:394–399.
