






We performed an epidemiological study of the traumatic injuries during the XVI South American U-17 Football Championship, 2015.
Material and methodsObservational surveys submitted by the 10 teams’ medical services of 220 players. Thirty-five games were held and 116 goals (3.31 per game) were recorded.
Results103 lesions, i.e., 2.94 per game or 32.7 injuries per 1000min, were recorded. Fifty-six were from direct contact and 66 required treatment. 36% were punished by the referees and 26% of injuries led to a yellow or red card. Injuries were most common in the ankle (15 cases), Achilles tendon (14 cases) and thigh (14 cases), followed by trauma to the knee and foot (7 cases each), face and the lumbar region (6 cases each), being rare in the upper extremity.
ConclusionInjuries during Soccer World Cup are difficult to predict and prevent, but serious injuries are rare. It is necessary to establish protocols that get adequate health care at all levels to solve problems arising, both in training and during the competition, and be prepared to solve the serious problems that may arise.
Estudio epidemiológico de las lesiones traumáticas producidas durante el XVI Campeonato Sudamericano de Fútbol Sub-17 en 2015.
Material y metodologíaEstudio observacional de las encuestas enviadas por los servicios médicos de 220 jugadores, de los 10 equipos participantes en el campeonato. Se celebraron 35 partidos y se anotaron 116 goles (3,31 por partido).
ResultadosSe registraron 103 lesiones, es decir, 2,94 lesiones por partido o 32,7 lesiones por cada 1.000min de juego. Cincuenta y seis fueron por contacto directo y 66 requirieron tratamiento. El 36% de las lesiones fueron sancionadas con falta y el 26% de las lesiones vieron también tarjeta. Las lesiones fueron más frecuentes en el tobillo (15 casos), problemas del tendón de Aquiles (14 casos) y en el muslo (14 casos) seguidos por traumatismos en la rodilla y en el pie (7 casos cada uno), la cara y la región lumbar (6 casos cada uno), siendo poco habituales en la extremidad superior.
ConclusiónLas lesiones durante un campeonato mundial de fútbol son difíciles de prever y de evitar, si bien las lesiones graves son raras es cada vez más necesario establecer protocolos de actuación que consigan una buena asistencia médica a todos los niveles para resolver los problemas que se producen, tanto en los entrenamientos como durante la competición, así como estar preparados para solucionar los problemas graves que puedan surgir.
Football is the most widely played sport among young people under the age of 18 years, and it is also the most popular, with more than 250 million federated players.1,2 It is therefore not surprising that a high number of injuries occur, while on the other hand international bodies have run injury prevention campaigns. These campaigns centre especially on muscle and tendon injuries,3–7 and although they have been universally disseminated and are said to have been beneficial, there is no scientific evidence that they reduce the number of injuries.
Nevertheless, in spite of the importance of the large number of injuries which arise, many of which prevent doing sports, the sports injury data collection system is difficult and non-uniform. Many authorities either do not follow the established protocols or simply lack data. The majority of authors agree on the location of injuries and the nature of the same. Muscle and tendon injuries are the most common, although opinions on them differ widely. It must be taken into account that training injuries are most common preseason, and that they tend to fall in number during the season itself.8
Championships provide an opportunity to analyse the injuries that occur, when they occur and their severity and affect on players. This study analyses the injuries suffered by footballers during the 16th South American Under-17 Championship.
Material and methodWe collected data on the incidents and physical activity of the players in the 16th South American Under-17 Championship. This was held in Paraguay from 4 to 29 March 2015. All of the players were 16 or 17 years of age. 35 games were played and 116 goals were scored (3.31 per match). The average number of minutes played amounted to 343 (SD: 235), with a range from 810 to 3min (Table 1).
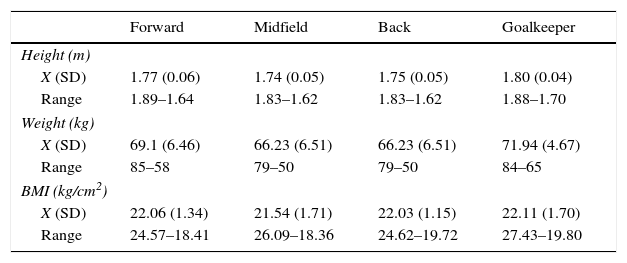
Anthropometry of footballers according to their position in the field.
| Forward | Midfield | Back | Goalkeeper | |
|---|---|---|---|---|
| Height (m) | ||||
| X (SD) | 1.77 (0.06) | 1.74 (0.05) | 1.75 (0.05) | 1.80 (0.04) |
| Range | 1.89–1.64 | 1.83–1.62 | 1.83–1.62 | 1.88–1.70 |
| Weight (kg) | ||||
| X (SD) | 69.1 (6.46) | 66.23 (6.51) | 66.23 (6.51) | 71.94 (4.67) |
| Range | 85–58 | 79–50 | 79–50 | 84–65 |
| BMI (kg/cm2) | ||||
| X (SD) | 22.06 (1.34) | 21.54 (1.71) | 22.03 (1.15) | 22.11 (1.70) |
| Range | 24.57–18.41 | 26.09–18.36 | 24.62–19.72 | 27.43–19.80 |
220 players in 10 different teams took part. The competition started with two groups containing five teams each. All of the teams in each group played against each other in a league system. The best three teams from each group classified for the final phase. This consisted of another league in which all of the teams played each other. In the case of a points draw in any position, classification was based on the following criteria, in decreasing order: goal difference, number of goals scored and the result of a match played between drawn teams decided by a draw.
The forwards scored 49 goals, midfield players scored 39 and defence players scored 13. During the championship 144 yellow cards and 11 red ones were shown. The forwards were shown 33 yellow cards and one red card; defenders were shown 57 yellow cards and 7 red cards, while midfield players were shown 53 yellow cards and 3 red ones, while the goalkeepers were only shown one yellow card.
The average height of players was 1.76m (SD: 0.06), with a range from 1.60m to 1.90m. Their average weight was 67.93kg (SD: 6.33), with a range from 50kg to 85kg. Their average body mass index was 21.88cm/kg2 (SD: 1.49), with a range from 18.36cm/kg2 to 27.42cm/kg2 (Table 2).
Minutes played according to players’ positions in the field.
| Minutes played | Total | Forward | Midfield | Back | Goalkeeper |
|---|---|---|---|---|---|
| X (SD) min Range min | 810–3 | 268 (211) 759–9 | 336 (226) 796–7 | 405 (231) 810–3 | 354 (285) 810–90 |
| 0 | 24 | 2 | 3 | 7 | 12 |
| <90 | 33 | 13 | 10 | 4 | 6 |
| 91–180 | 32 | 10 | 13 | 7 | 2 |
| 181–270 | 36 | 3 | 15 | 18 | 0 |
| 271–360 | 30 | 10 | 13 | 5 | 2 |
| 361–450 | 8 | 2 | 3 | 3 | 0 |
| 451–540 | 10 | 1 | 4 | 5 | 0 |
| 541–630 | 12 | 4 | 3 | 5 | 0 |
| 631–720 | 25 | 4 | 10 | 11 | 4 |
| >720 | 10 | 1 | 4 | 4 | 1 |
The medical services of the participating teams sent in a survey of incidents after each training session and match. The data were analysed and processed by the Medical Commission of Conmebol (the South American Football Confederation). This first study only counted the incidents which occurred during each official match. Anything which occurred during the championship that required treatment by a team's medical service was defined and treated as an incident. We performed a descriptive statistical study of the height, weight and BMI of the players in the championship and the injuries which occurred in the games.
Results103 injuries were recorded, i.e., 2.94 per match or 32.7 injuries per 1000min play. 56 injuries were due to direct contact; 27 (36%) were punished by the referees and 26% of injuries led to a yellow or red card from the referee. 66 (64%) injuries required treatment on the pitch or immediately afterwards.
During the championship there was one anterior cruciate ligament rupture, two torn muscles, 8 strained muscles, 6 sprains, one cranioencephalic trauma without loss of consciousness, two lacerations and 48 bruises (Fig. 1). The ankle was the most frequent location of injuries (15 cases), followed by Achille's tendon problems (14 cases) and thigh injuries (14 cases), after which come knee and foot injuries (7 cases each), the face and lumbar region (6 cases each). Injuries were less frequent to the shoulder (2 cases), the ribs (2 cases), the wrist, hand or abdominal region (with one case each) (Fig. 2).
Discussion

Although the injuries suffered by footballers during different championships have been described in publications, it must not be forgotten that they are a heterogeneous group of players with very different histories.9 In the 2014 World Cup McCall et al.10 stated that the majority of teams implemented a protocol to prevent injuries. This may be compared to the fact that 84% of juvenile football teams only have a first-aid bag, most of which are poorly equipped and maintained. In 60% of occasions it is the trainer who gives first aid.11
It is known that there are many different causes for the injuries suffered during games. The players in a winning team have a higher risk of suffering an injury.12 Injuries occur most frequently at specific moments of a match, more specifically 5min after the referee has shown a red or yellow card, after another injury or when a goal is scored. However, the highest number of injuries occur in the last 15min of the first half. The number of injuries is also linked to the number of fouls in a match; there were fewer injuries due to fouls (20.6/1000h of play) than injuries that occurred without contact of any kind, and this was observed at all positions in the field.13,14
There are several injury prevention programmes, and they are based on different principles. Although there is interest in these programmes, they have not been proven to have any effect. Impellizzeri et al.15 state that the “FIFA 11+” programme improves neuromuscular control and increases the strength of the knee flexors, and it does not prevent injuries; Steffen et al.16 found no differences between injuries to the legs depending on whether or not a prevention protocol was applied. In a revision of the literature Van Beijsterveldt et al.17 found six studies with contradictory results; two studies show a statistical fall in the number of injuries, while the other four show a preventive effect without statistical value. De Hoyo et al.18 analysed 36 young players (U-17 and U-19) and found that players following the programme spent fewer days without playing due to injury per 1000h of play, and that their muscular capacity also improved.
Youth football is becoming increasingly demanding because professional teams tend to sign up younger and younger players, and they try to follow the most talented ones. This is why championships of players under 20 years of age of both sexes are becoming more frequent and competitive. In the 2009–2010 season Van Beijsterveldt et al.19 compared the injuries suffered by 456 amateur Dutch players and 217 professionals. He found very similar injury rates in both groups. Bollars et al.20 compared the incidence, location, duration and severity of injuries in Belgian footballers of all types, male and female, in two seasons 10 years apart. They found a fall of 21.1% in the number of injuries in the second season, most especially in winter. In both seasons they found a peak in the number of injuries in the first three months. Tourny et al.14 analysed 618 injuries suffered by young football players aged from 12 to 20 years. They found that an average of 137 players were injured per season (66 of the younger players and 71 of the older ones). More injuries occurred in games than in training sessions. 77% of injuries occurred without contact in the younger players and in 65.6% of injuries for the older ones. Injuries affected the younger players in the thigh (23%) and hip (19%), while 32% of injuries in the older players were to the thigh and 20% were to the ankle.
The Medical Committee of the UEFA has published studies monitoring 1743 players in 27 teams and 10 different countries over 11 years (2001–2012). In total they found 8029 cases of sports inactivity due to injury. On average each player suffered two injuries per season, with 50 injuries per team. The number of ligament injuries fell during the study period, while the number of muscle and severe injuries remained constant, as did the injury rate during this time.21 On the other hand, Waldén et al.22 analysed ankle injuries in the same sample. They found that ankle sprains accounted for half of all ankle injuries, while the ankle impingement syndrome was very rare among professional footballers, in spite of what has been described. The majority of ankle injuries occurred due to fouls during games.
Gajhede-Knudsen et al.23 observed that Achille's tendon injuries amounted to 3.8% of all injuries. They are more frequent in older players, and recurrence is more frequent when players do not rest for long. In our study ankle, calf, Achille's tendon and foot injuries accounted for one third of all the injuries during the championship.
Our study centred on a group of elite young players who hardly differ from older professionals. Hammes et al.24 found no differences in the frequency and location of injuries between different age groups. They only found that fewer injuries occurred during training sessions (4.5/1000h) than during competition (24.7/1000h). Nor did Svensson et al.25 find differences in the number of injuries in players older and younger than 23 years of age, although the older ones had more Achille's tendon injuries. Suzue et al.26 sent a questionnaire to 113 youth football teams with 1162 players during the regional championship. This asked about pain during matches, while training or afterwards. Those players who said they had pain were subjected to ultrasound or X-ray examination, depending on the location and type of pain. They found 547 players (47.1%) with pain, of which 4% had positive findings in the lumbar region of the spinal column, 5.3% had findings in the hip, 40.1% in the knee, 23.7% in the ankle, 45.7% in the heel and 18.2% in other parts of the foot. The imaging examination of 106 players showed osteochondrosis in 75.5% of young players with pain. In 49 cases this corresponded to Sever's disease, in 13 to Osgood–Schlatter's disease, in 12 to a split kneepan, Sinding–Larsen–Johansson's syndrome in 10, osteocondritis dissecans of the distal femur in one case and spondylolysis in 3.
Faude et al.2 analysed 53 publications on sports problems in young footballers. The incidence of injuries in training was constant among players aged from 13 to 19 years, with a frequency of 1–5 injuries/1000h. The number of injuries during matches increased with age, from 15 to 20/1000h play in footballers above the age of 15 years. From 60% to 90% of all injuries were classified as traumatic, while approximately 10–40% were caused by overload. The majority of injuries (60–90%) were located in the lower limbs, and the ankle, knee and thigh were the parts affected most often. The frequencies of upper limb or head involvement were higher in the studies that only analysed injuries in matches, and this finding agrees with those of our study. Approximately half of the injuries led to the ceasing of sports activities for one week, while one third led to a rest period of from 1 to 4 weeks. From 10% to 15% of all the injuries were considered to be severe.
Bastos et al.27 studied 301 football players with an average age under 15 years, of whom 24.25% suffered at least one injury. The tallest players suffered more injuries (62.5%) than the shorter ones (37.5%) and they were also more frequent in players who had been training continuously for more than five years (69.65%) compared with those who had trained for a shorter time (30.35%). Kristenson et al.28 also found that the injury rate increases with age, peaking in players aged 30 years.
It is estimated that from 2% to 20% of all football injuries are fractures, one third of which are located in the lower limbs, although they are more frequent in boys younger than 15 years of age.2 A Belgian retrospective study29 located 1600 fractures, 3% of all injuries, in the legs, while ankle fractures are the most frequent (37%), followed by foot fractures (33%) and those in the tibia (22%). The least common were fractures of the tibula (9%). Fractures of the upper limbs in young football players in Holland increased considerably from 1988 to 2009, with an increase of 19.4% in players aged from 5 to 19 years, 73.2% in those aged from 11 to 14 years and 38.8% in those aged from 15 to 18 years.30
Injuries also varied depending on the position played. Goalkeepers play under special conditions and have a tendency to suffer acute injuries of the abductor muscles and ones due to overload in the hips and pubis, while ischiotibial muscular injuries are very rare.31 The position played influences the type of injury, and during matches young players are more likely to be injured in the cornerback position (30.4%), while older players are more likely to be injured in midfield positions (26.6%) and the centre-backs (23.1%). Using goalkeepers as the benchmark, Kristenson et al.28 found that backs have an injury index of 1.91, centre field players 1.78 and forwards 1.82.
Cranial injuries are rare in football although they are potentially important. Nevertheless, facial injuries are very common. Contusions in football are very rarely accompanied by a loss of consciousness. Although referees punish jumping with the arms open with a foul and yellow card, the most frequent contusions are impacts on the face of an opposing player. Nevertheless, doctors have to act immediately when there is a loss of consciousness. It is therefore fundamental to diagnose the degree of severity and prevent subsequent consequences, so that it is necessary to ensure that players return to play safely. In case of cranial contusion the player should never return to play on the same day even when there are no symptoms and the results of clinical examination are normal.32
Although injuries to the knee joint are not the most frequent they attract the attention of specialists more, as some of them require surgery. Lundblad et al.33 describe injury of the collateral medial of the knee as the most common injury among professional footballers. He found 346 injuries, 70% of which were due to contact during 1,057,201h of play (0.33/1000h). The injury index in matches was 9 times more frequent than it is in training, and the average recovery time before playing again was 23 days. 24% of meniscus injuries were to the internal meniscus, 8% were to the external meniscus and from 20% to 30% were associated with ligament injuries.34 Analysing two Belgian football seasons 10 years apart, there were 9971 knee injuries, with a significant fall in the number of injuries, as they fell from 1.5/100 players in the year 2000 to 1.2/100 players in 2010. 6% of all knee injuries were breakages of the cross anterior ligament, and these increased slightly between the first and second seasons from 0.081 to 0.084 per 100 players.35 Little can be done to prevent injuries of the anterior crossed ligament.36 The Swedish registry of anterior crossed ligament injuries37 states that the ratio of women to men stands at 42:58. Breakage of the ligament occurred during a football match in 36% of cases in women and in 49% of cases in men.
Muscle and ligament injuries are the most frequent.38 Hallen and Ekstrand39 followed up 89 professional European football teams for 12 years. They found that a negative MR was associated with less time off playing (6 days). 83% of ischiotibial injuries were in the femoral biceps m., while 12% affected the semimembranous m. and 5% the semitendinous m. Recurrence was more likely in injuries of the femoral biceps m. (18%). Pubalgia led to an average time off playing of 9 days, in comparison with ischiotibial injuries (13 days), the quadriceps (12 days) and the calf muscles (13 days). To return to the UEFA registry collected over eleven seasons, Ueblacker et al.40 followed up 1981 players in 31 football teams. They found 2287 muscle injuries in the thigh (25% of all the injuries) of which 88% were due to indirect injury and 12% were caused by contact. The indirect injuries led to longer periods of inactivity, at 18 days, compared to 7 days in the case of direct injuries. Hägglund et al.41 analysed muscle injuries in the UEFA registry and identified 2123 muscle injuries. Injuries to the abductor muscles (56%) and the quadriceps muscle (63%) were the most frequent injuries in the kicking leg. The intrinsic factors associated with muscle injury were a previous injury, older age and the kicking leg. Injuries also varied over the length of the season and depend on the position of the player. Older players suffered twice as many injuries, and the dominant leg also suffered more injuries. Injuries to the quadriceps muscle occurred more frequently in the preseason, while the abductors, ischiotibial and calf muscles were injured more often during the season.41 Prevention programmes are controversial. In a study of 20 teams with 296 players 6.2% suffered an ischiotibial injury, and no differences were found depending on whether or not groups had included the preventive programme.42
Another factor that may be mentioned in order to comprehend the high number of injuries which occur is the number of matches each team plays per season. Bengston et al.43 collected data prospectively on the number of matches lost per injury in 27 teams over 11 seasons. Matches were grouped according to the days rested before the next match. In the European League there were more lost matches the shorter the recovery time. The total number of injuries and muscle injuries increased for league matches with 4 or more days rest in comparison with periods of 6 days or more.
Football injuries are hard to foresee and prevent. They are very common and although severe injuries are rare, it is increasingly necessary to establish protocols for action to ensure good medical attention at all levels. This has the aim of resolving problems that may arise in training as well as during matches, as well as being prepared to deal with any severe problems that may occur. On the other hand, when talking about injuries in football the tendency is to always think of trauma. However, medical incidents requiring suitable attention are as or more frequent.
Level of evidenceLevel IV.
Ethical responsibilitiesThe protection of persons and animalsThe authors declare that no experiments using human beings or animals took place for this research.
Data confidentialityThe authors declare that this paper contains no patient data.
The right to privacy and informed consentThe authors declare that this paper contains no patient data.
Conflict of interestThe authors have no conflict of interests to declare.
Please cite this article as: Pangrazio O, Forriol F. Epidemiología de las lesiones sufridas por los jugadores durante el XVI Campeonato Sudamericano Sub-17 de Fútbol. Rev Esp Cir Ortop Traumatol. 2016;60:192–199.
