



Hip dysplasia has been associated with risk factors such as breech presentation, female gender or family history. However, external factors, such as the use of baby carriers, seem to influence the development of the hip in the first months of life. The aim of this study is to evaluate the position of the hips of babies placed in different types of baby carriers by ultrasound image.
MethodAn ultrasound study of the hips of healthy babies between 1.5 and 3.5 months of age was carried out, when the children were carried in three different baby backpacks, which provide different degrees of support for the babies’ thighs. All hips were type I according to the Graf classification.
Graf's alpha angle, acetabular coverage and distance to the pubis were assessed at baseline (examination table) and when the children were carried in the three different backpacks.
ResultsIn all cases, the babies showed normal values in the three studied parameters, without statistically significant differences between any of the situations. There were also no differences in the ultrasound parameters related to the sex, age or weight of the baby.
ConclusionsThe right hip of the babies shows normal ultrasound parameters when placed in any of the baby carriers studied.
La displasia de cadera se ha asociado con factores de riesgo como la presentación de nalgas, el sexo femenino o los antecedentes familiares. Sin embargo, factores externos, como los sistemas de porteo, parecen influir en el desarrollo de la cadera en los primeros meses de vida. El objetivo del presente trabajo es valorar por imagen ecográfica la posición de las caderas en bebés colocados en diferentes tipos de mochilas portabebés.
MétodoSe ha realizado un estudio ecográfico de las caderas de bebés sanos entre 1,5 y 3,5meses de edad, cuando el niño es porteado en tres diferentes mochilas portabebés que proporcionan diferentes grados de sujeción de los muslos del bebé. Todas las caderas eran tipoI de Graf.
Se han valorado tres parámetros ecográficos: el ángulo alfa de Graf, la cobertura acetabular y la distancia a pubis en situación basal (mesa de exploración) y en las tres diferentes mochilas de porteo.
ResultadosEn todos los casos los bebés mostraron valores de normalidad en los tres parámetros estudiados, sin diferencias estadísticamente significativas entre ninguna de las situaciones. Tampoco se encontraron diferencias en los parámetros ecográficos relacionadas con el sexo, la edad o el peso del bebé.
ConclusionesLa cadera derecha del bebé mantiene unos parámetros ecográficos de normalidad cuando es colocada en cualquiera de los modelos de mochila estudiados.
Baby-wearing has been present in any number of cultures over the history of Humankind and in today's society, it has gradually been implemented more and more and understood as an improvement in the care and affective relationship with the infant, as well as an advance in convenience and freedom of movement it provides for the parents. There are several carrying methods, such as the wrap, the Mei Tai, the pouch, the sling or the carrier, but parallel to the increased use of all of them, there has been growing concern over the ergonomics of these systems for the child's hips, as well as for the possibility that they may foster the development of hip dysplasia.
Dysplasia of the hip is a modification in the development of the hip that mainly affects the acetabulum and the most important risk factors for which reported in the literature1,2 are breech presentation (relative risk RR 3.75), being female (RR 2.54), being the first pregnancy (RR 1.44), and family history (RR 1.39).
The literature reports that there are external factors related to the position of the hips that affect their development. Carrier systems in which the child's legs are extended in adduction, such as the Navajo Indian system, of wrapping systems, appear to be related with an incidence of hip dysplasia up to 10 times higher.3–12 In contrast, in populations in which babies are worn on the back with their legs in abduction and flexion, the incidence of dysplasia of the hip is very low.13
The position in abduction and flexion of the hips (M position) has been promoted by some baby carriers as being ergonomic and fostering proper hip development. Other carriers in which the legs dangle more and have less of an M position have been criticised for possibly fostering improper hip development.14
Ultrasound is the method of choice for assessing joint congruency and morphology and the acetabular coverage of the hip in babies under the age of 3 months.2,15 The ultrasound scan has numerous advantages over other imaging techniques, as it is a method that is well-tolerated by the babies without requiring sedation, does not use ionising radiation, and can be performed dynamically on the examining table or, as in the case of this study, in the baby carriers themselves.
There is a study that looks at the position of the femoral head in the acetabulum in babies with wrapping systems,16 but despite the fact that nowadays the use of baby carriers is more and more common, there are no studies in the literature that have explored hip position in the different baby carriers using imaging techniques. The objective of this work is to use ultrasound imaging to assess the position of the hips in infants placed in different types of baby carriers.
Material and methodThis is a prospective study approved by the Ethics Review Board at our hospital (PR-AMI: 94/2017).
Healthy infants of both sexes between the ages of 1.5 and 3.5 months of age were included in the study. This age range is chosen to make examination easier (>1.5m) and for the degree of maturity of the hip (<3.5m), when there may still persist a certain articular laxity and the position adopted in each type of carrier can have a major influence in the development of an immature hip, which is the reason of interest of this study. Infants presenting with any other medical or orthopaedic disorder were excluded. Parents gave their consent to participate in the study and were present during the ultrasound examination.
All ultrasound scans were performed by the same paediatric radiologist using a Siemens S2000 ultrasound device with a multi-frequency linear array set to 9MHz (Siemens Healthineers®, Berlin, Germany). Transverse images were collected using the Graf method because it has been reported to be one of the most valid in the study of hip dysplasia.17
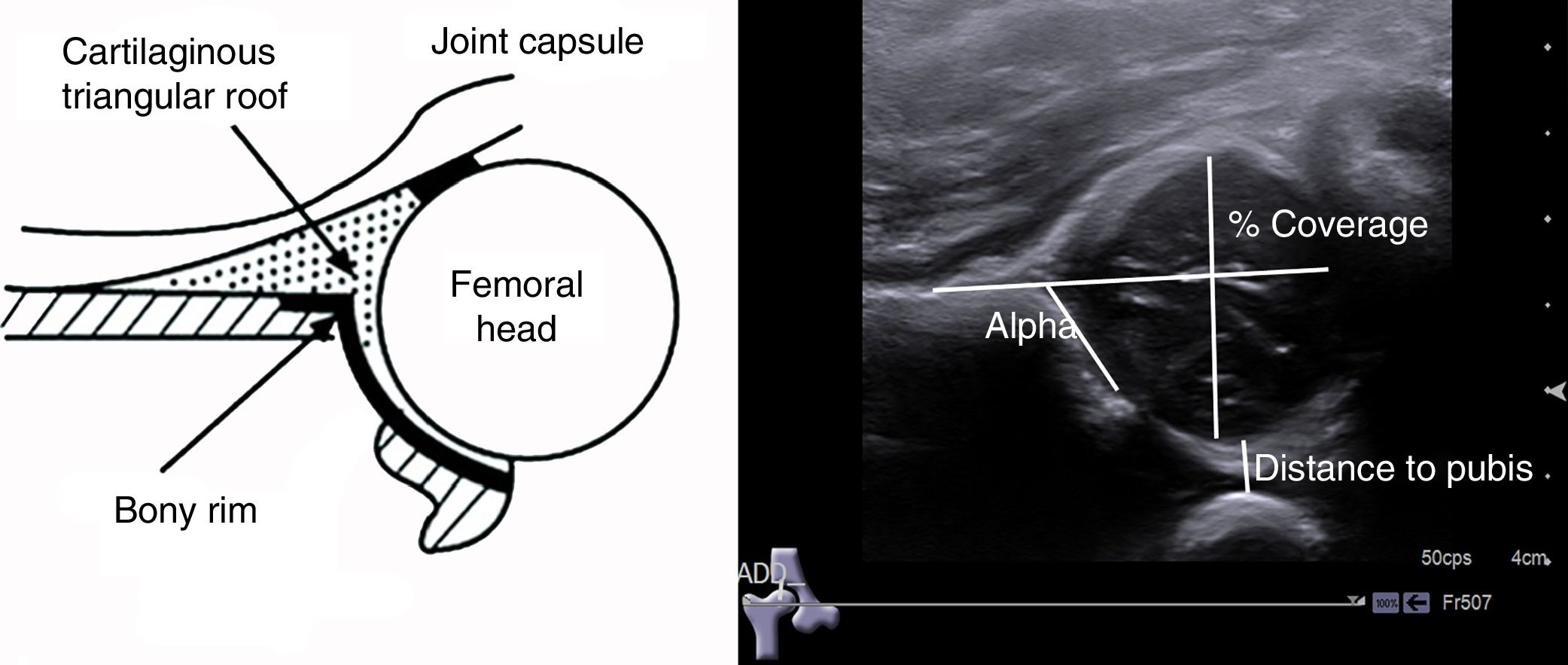
As Graf18 reported, an image of the joint must be attained in the coronal plane that includes the straight line of the iliac bone, the junction of the ilium with the triradiate cartilage and the acetabular labrum. Once the image in the neutral position is obtained, the acetabular morphology, alpha angle, coverage of the femoral head, and the distance from the pubis to the femoral head are assessed (Fig. 1). Graf's alpha angle is calculated by generating an angle between the horizontal line of the ilium and the acetabular roof.

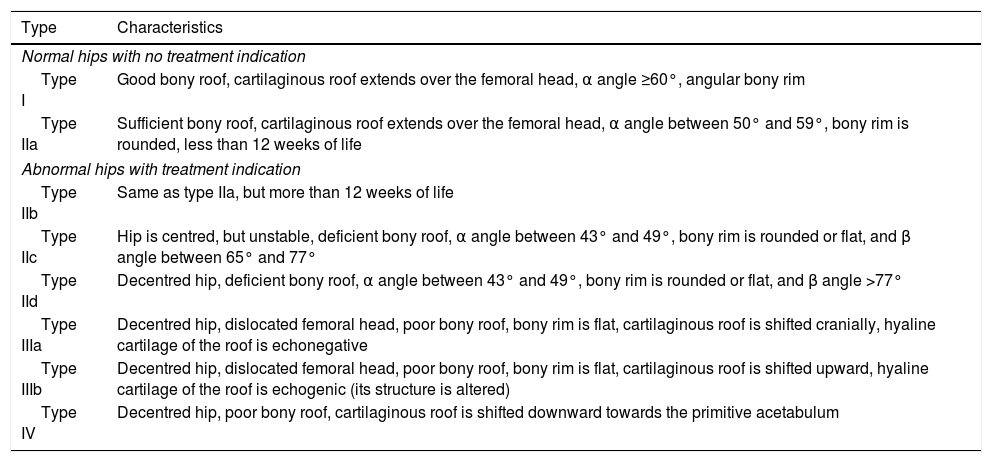
Ultrasound images were obtained of the hips of the infants placed in four situations: on the examining table and carried in three different types of commercial carriers. The situation on the examining table was the baseline examination and was performed at rest and in adduction stress and served to appraise the presence or absence of dysplasia of the hip. Following Graf's classification (Table 1),19 only infants meeting the following criteria were included: type I hips, alpha angle of more than 60°, acetabular coverage >50%, and distance to pubis ≤4mm. Babies with type IIa hips and alpha angles of between 50° and 59° were excluded because, while deemed normal in babies of less than 3 months of age, they may require treatment once they are more than three months old.20–22
Graf's ultrasound classification of hips at birth.
| Type | Characteristics |
|---|---|
| Normal hips with no treatment indication | |
| Type I | Good bony roof, cartilaginous roof extends over the femoral head, α angle ≥60°, angular bony rim |
| Type IIa | Sufficient bony roof, cartilaginous roof extends over the femoral head, α angle between 50° and 59°, bony rim is rounded, less than 12 weeks of life |
| Abnormal hips with treatment indication | |
| Type IIb | Same as type IIa, but more than 12 weeks of life |
| Type IIc | Hip is centred, but unstable, deficient bony roof, α angle between 43° and 49°, bony rim is rounded or flat, and β angle between 65° and 77° |
| Type IId | Decentred hip, deficient bony roof, α angle between 43° and 49°, bony rim is rounded or flat, and β angle >77° |
| Type IIIa | Decentred hip, dislocated femoral head, poor bony roof, bony rim is flat, cartilaginous roof is shifted cranially, hyaline cartilage of the roof is echonegative |
| Type IIIb | Decentred hip, dislocated femoral head, poor bony roof, bony rim is flat, cartilaginous roof is shifted upward, hyaline cartilage of the roof is echogenic (its structure is altered) |
| Type IV | Decentred hip, poor bony roof, cartilaginous roof is shifted downward towards the primitive acetabulum |
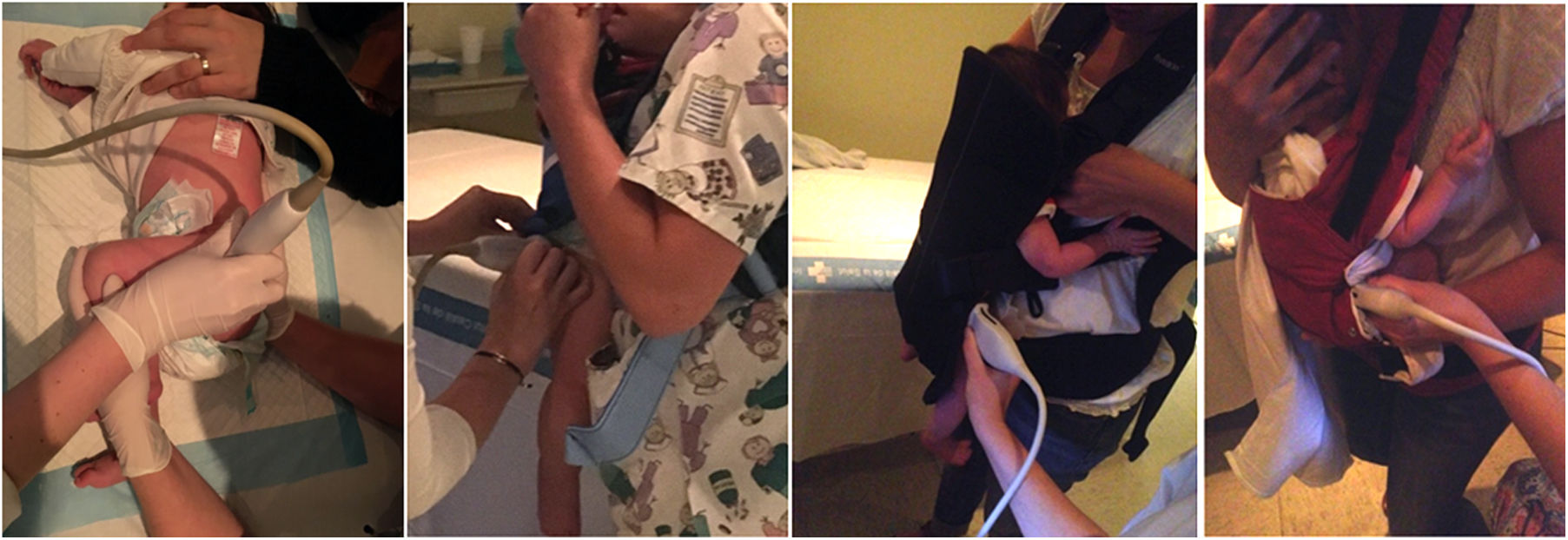
The carriers studied were Babyjörn Original (Babyjörn®, Solna, Sweden), Babyjörn One (Babyjörn®, Solna, Sweden), and Manduca (Wickelkinder GmbH®, Marburg, Germany) (Fig. 2). The infants were placed in the baby carriers as per the manufacturer's instructions and bearing in mind the infant's weight.

An ultrasound scan of both hips was obtained on the examining table and only the right hip was scanned in the baby carriers. The study was initiated with the child on the examining table in all cases, then with the infant in the Babyjörn Original baby carrier, and later, in the other two carriers.
A univariate (mean, standard deviation, and 95% CI) and a multivariate (non-parametric for related data) study were carried out among the types of carrier, taking into account age, weight, and gender.
ResultsA total of 15 infants were included: 5 males and 10 females. The mean age was of 65 days (between 48 and 98) and mean weight was 5.2kg (between 3.5 and 6.6kg).
The baseline ultrasound scan revealed a mean alpha angle of 65.2° (standard deviation [SD] 4.5°) on the right side and 68.0° (SD 3.7°) on the left; mean acetabular coverage was 61.6% (SD 7.4%) on the right side and 60.2% (SD 7.0) on the left, and mean distance to pubis was 3.0mm (SD 0.6mm) on the right side and 3.0mm (SD 0.6mm) on the left. There were no significant differences between the right side and the left on any of the three ultrasound parameters (p=.6, p=.2, and p=.2, respectively).
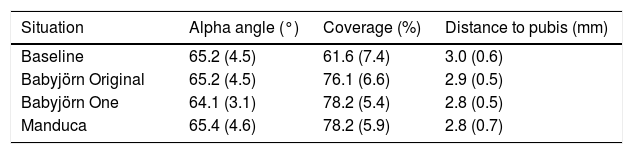
The alpha angle values were always more than 60° in all the carriers and no significant differences were revealed among them or with the baseline position (Table 2).
Mean and standard deviation of ultrasound parameters of the hips in each situation (hip right measurements).
| Situation | Alpha angle (°) | Coverage (%) | Distance to pubis (mm) |
|---|---|---|---|
| Baseline | 65.2 (4.5) | 61.6 (7.4) | 3.0 (0.6) |
| Babyjörn Original | 65.2 (4.5) | 76.1 (6.6) | 2.9 (0.5) |
| Babyjörn One | 64.1 (3.1) | 78.2 (5.4) | 2.8 (0.5) |
| Manduca | 65.4 (4.6) | 78.2 (5.9) | 2.8 (0.7) |
The acetabular head coverage values were >60% in all the carriers and no significant differences among them were found, although they were higher than in the baseline situation (Table 2).
All the values for the distance to the pubis were <4mm in all the baby carriers with no significant differences in any of them or with respect to the baseline situation (Table 2).
No significant differences were detected for any of the parameters on the basis of age, gender, or weight.
Six infants did not tolerate the repeated ultrasound scans in all three carriers; consequently, images were only attained in these cases in two carriers: in the Babyjörn Original and in the Manduca.
DiscussionThis work objectively studies the position of the hips in infants carried in three different carriers and shows that none of them give rise to differences in the position of the hip according to the three ultrasound parameters studied: the alpha angle, coverage of the femoral head, and distance to the pubis.
Three types of baby carriers have been analysed that place the infant in apparently different positions. The Babyjörn Original carrier apparently positions the legs such that they are freer and in less of an M position as a result of it having less thigh support; less coverage and longer distance to the pubis are therefore to be expected if the legs were truly dangling. The baby's legs are bent more and in the M position in the Babyjörn One carrier. The Manduca carrier places the legs in the M position and appears to bend the legs even further, limiting mobility somewhat more. The ultrasound results, however, reveal no changes in any of the parameters studied; the apparent external position in the three different carriers has no influence in the situation of the hips when analysed on ultrasound scan.
We have detected no gender- or age-related differences, despite the fact that being female or younger might entail greater joint laxity and greater differences on the ultrasound parameters depending on the position adopted in a given carrier.
We have used only baby carriers because they give rise to a more or less fixed position of the infant's hips while being worn, making it possible to obtain homogenous data. With other carrier systems, such as the wrap or the sling, the infant's position must be adjusted each time baby-wearing is begun, meaning that the data regarding hip position provided with these systems are more heterogenous as regards hip position. Furthermore, only three of the carriers on the market have been analysed; consequently, it may be that there are differences in the position of the hips. Nevertheless, models were chosen that show the broad variation that exists on the market.
The work has a series of limitations. First of all, the number of infants analysed is small; nonetheless, the results are very robust and in case was the hip placed outside normal ultrasound parameters.
Assessment was always performed with the baby-wearer standing and none of the images were obtained while moving, given the difficulty in attaining images in the proper projection when the carrier is walking. We do not know if the flexion and extension movements of the carrier's hip can cause changes in the position of the infant's hips. Similarly, images have not been acquired in stress, given that the position of the infant in each carrier is more or less fixed and stable, keeps the hips from moving. Likewise, infants with dysplasia of the hip have not been studied; they might be more sensitive to the different morphologies of the carriers studied but who might also yield greater heterogeneity of results.
The infants exhibited variable tolerance to being placed sequentially in the three carrier devices; as a result, not all of them could be studied in the three carriers. All the infants were examined at baseline, in the Babyjörn Original carrier, and at least one of the other carriers. Despite the fact that a RR of 1.54 of dysplasia on the left side versus the right side has been reported,1 the baseline examination revealed the absence of dysplasia on both sides with no differences in the ultrasound values between the right and left sides. Therefore, only the right side was studied while the child was in the carrier(s), with the aim of decreasing the overall examination time and so that the infant could tolerate the study.
All the carriers studied place the child's hip in an M-position similar to the one caused by the use of a treatment harness for dysplasia. This might account for the low incidence of dysplasia found by Graham in the population of Malawi.11 Nonetheless, there are not studies that support the use of carriers as a substitute for treatment with a harness, nor can we conclude from the present study that they can be used instead of the harness.
We can conclude that the infant's right hip maintains ultrasound parameters that are within normal range when placed in any of the carrier models studied.
Level of evidenceLevel of evidence IV, case series.
Conflict of interestsDoctor Fontecha has participated occasionally as medical consultant in Spain for the Babyjörn company. None of the other authors have any conflict of interests.
Please cite this article as: Fontecha CG, Coma Muñoz A, Catala Muñoz A. Exploración ecográfica de las caderas del bebé en mochilas de porteo. Rev Esp Cir Ortop Traumatol. 2019;63:289–294.
