







Terrible triad of elbow is a complex lesion with a high rate of complications. Our goal is to analyse both clinical results and complications after performing protocolised surgery.
Material and methodsWe performed a prospective longitudinal study using our hospital database. We obtained a total of 62 triads. The initial approach was lateral and when necessary we added a medial approach. We treated 3 main pillars, the radial head, the coronoid process, and the lateral collateral ligament. If needed, we repaired the medial collateral ligament or we performed an external fixator.
ResultsIn our series, the radial head was synthesised in 14 (22.5%), an arthroplasty was performed in 45 (72.5%), and other actions in 3 (5%). The coronoid could be synthesised in 12 (19.3%). In 41 (66.2%) a transosseous suture or an anchor were performed, and in 9 (14.5%) no treatment was given. The LCL was repaired in 100% of cases, in 9 (14%) the MCL had to be repaired, and 22% of the patients required Ex-Fix.
There were 17 (27%) complications. Three (17.5%) cases of infections, 4 (23.5%) neurological lesions, 3 (17.5%) cases of stiffness, 1 (6%) ulnar impaction syndrome, and 1 (6%) case with an intraarticular fragment postoperatively. Four (23.5%) heterotopic ossification, and 1 (6%) osteolysis of radial prosthesis were observed.
Regarding functional results, range of mobility (ROM) of 120°/−20° flexo-extension, and 98°/85° of prono-supination were obtained.
ConclusionsElbow triads are complex lesions where protocolised surgery is necessary, nevertheless the complication rate was 27% in our series.
La tríada terrible de codo es una enfermedad asociada a altas tasas de complicaciones, por ello queremos estudiar los resultados y las complicaciones.
Material y métodosSe ha utilizado la base de datos de nuestro hospital durante 2005-2015, recogiendo características del paciente, de la fractura, de la cirugía y las complicaciones asociadas, así como resultados funcionales y rango de movilidad.
ResultadosSe obtuvieron un total de 62 tríadas, de las cuales 27 (43%) eran mujeres y 35 (56%) eran hombres.
A todos se les realizó un abordaje lateral de Kaplan y en aquellos que lo necesitaron se complementó con un abordaje medial para reparar el LCM. La cabeza radial se sintetizó en 14 (22%) casos, se colocó una prótesis en 45 (74%) de casos y otras actuaciones en 3 (5%) casos. La osteosíntesis de la apófisis coroides se realizó mediante arpón±sutura transósea en 41 (62%) pacientes y mediante síntesis en 12 (19%) casos. En 9 (14%) casos no se realizó ninguna actuación. En el 100% de los casos se reparó el LCL y en 9 (14%) hubo que reparar también el LCM. Un 22% de los pacientes precisaron FE por inestabilidad tras la técnica quirúrgica.
Respecto a resultados, se obtuvo un rango de movilidad de entre 120°/–20° de flexoextensión y 98°/85° de pronosupinación.
En cuanto a complicaciones, obtuvimos un total de 17 (27%).
ConclusionesLas tríadas de codo son lesiones osteoligamentosas complejas donde es necesario realizar una cirugía protocolizada, a pesar de lo cual, existen un 27% de complicaciones.
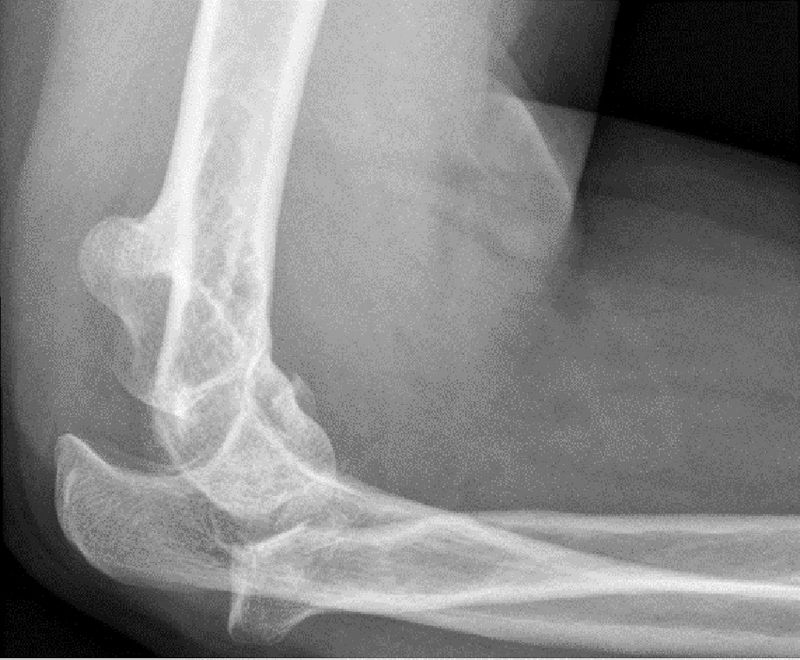
Terrible triad of elbow is the combination of elbow dislocation, radial head fracture and coronoid process fracture15 (Fig. 1). It is a complex injury involving bony and ligamentous elements, which necessitates a comprehensive and protocolised approach. Despite this, it is still an injury with a high rate of complications (including instability, stiffness, premature arthrosis or chronic pain.1,2,6,7,22,24,26,28

Although much has been reported in the literature on this subject many points of controversy remain regarding different approaches, whether or not to synthesise fractures of coronoid process which only affect the tip, and whether the medial collateral ligament (MCL) should be systematically repaired or not.
ObjectiveThe objective of our study was to apply protocolised surgical treatment for these injuries and analyse the clinical results and complications obtained.
Material and methodsA retrospective study using the database of our hospital, between the years 2005 and 2015. A total of 62 triads was obtained, collecting patients’ demographic data, fracture data (Mason and O’Driscoll classification), surgical data (approach, radial head treatment), coronoid process, lateral collateral ligament [LCL] and MCL) and associated complications, both intraoperative and during follow-up. Functional results were collected using the Mayo Elbow Performance Store (MEPS).10
Surgery performed in all cases followed a protocolised surgical technique which is detailed below.
Surgical techniqueIn all cases antibiotic perioperative prophylaxis with 2g of intravenous cephazolin was administered.
The patient was positioned in supine position with a side table and ischaemia cuff at axillary level.
Initial approach was always the Kaplan lateral approach (Fig. 2), between the extensor carpi radialis longus and the extensor communis digitorum, which provided better viewing of the radial head and the coronoids.

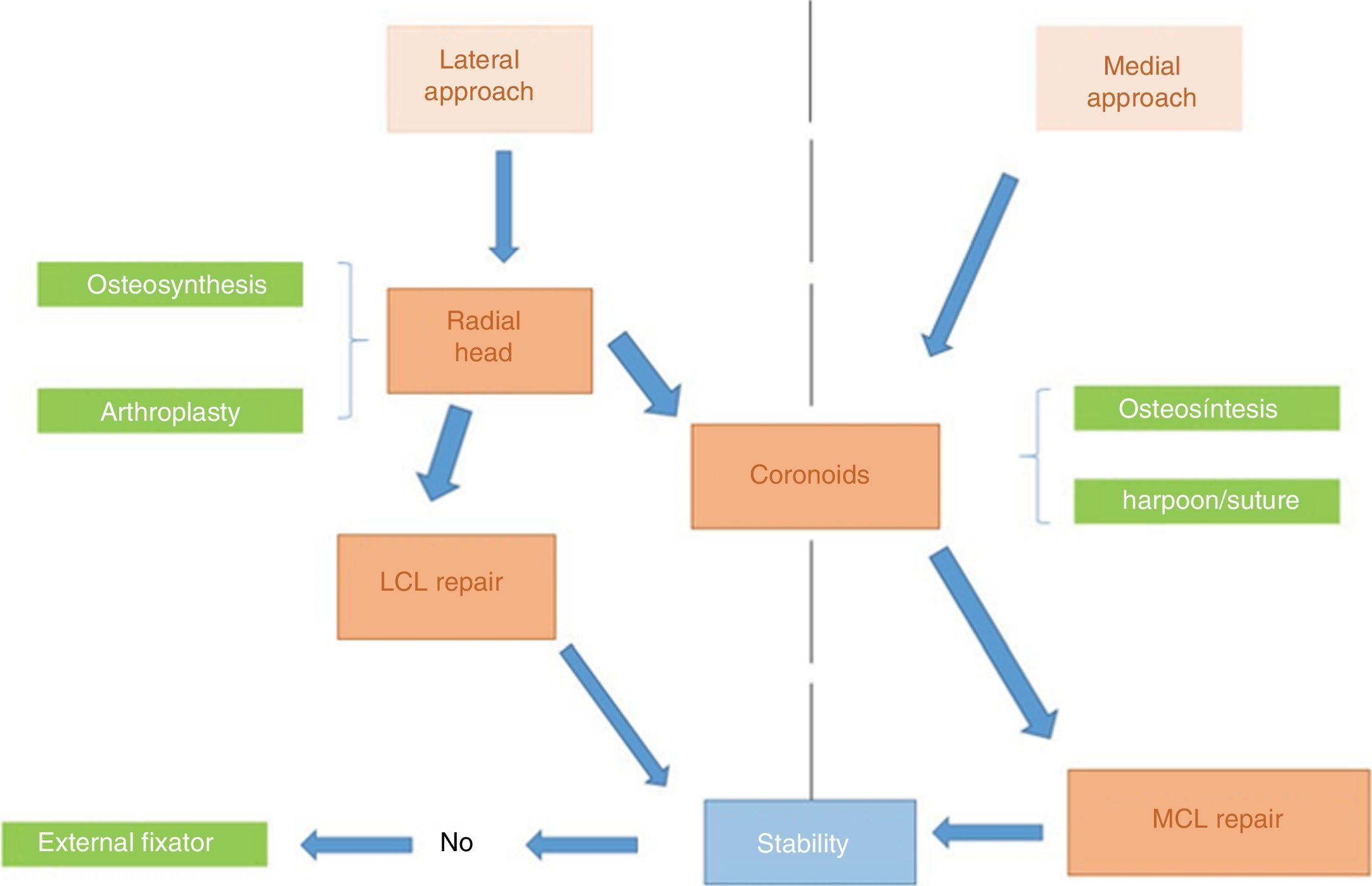
The 3 essential pillars of treatment of these lesions are coronoid process, radial head and LCL.
If lateral access allows for coronoid approach (especially in cases where the radial head is prosthesis) we repair it from this approach. In O’Driscoll types ii or iii, where a lateral approach is insufficient for performing osteosynthesis, we complement this with a medial approach. The repair technique of the coronoid process essentially depends on its size, if there is sufficient entity, synthesis may be made with cannulated screws or a plate, but if there were process tip fractures (O’Driscoll type i), a transosseous suture was performed or a re-anchoring of the anterior capsule using harpoon sutures.
Once the lateral approach has been used, this access route enables us to assess the possibility of synthesising the radial head. In cases where this was possible it was synthesised either with cannulated screws or with plates (Fig. 3). When comminution of the radial head made synthesis impossible, a radial head prosthesis was inserted.

The LCL was repaired using harpoon sutures in all cases, anchored at humeral level, since the majority of extractions occur in its proximal insertion.
Once the 3 essential pillars have been repaired we may assess the stability of the elbow with intraoperative scope (appropriate ulnar humeral reduction) and clinical control (elbow stability during a flexion extension arc of 20–130°18) (Fig. 4). If the elbow remains unstable when performing these 2 tests, we would proceed in 2 different ways.
- –
In those cases where we had already used the coronoid process approach with a medial approach, we would proceed to repair the MCL using harpoon suture.
- –
In those cases where only a lateral approach had been made, we would insert an external fixator.

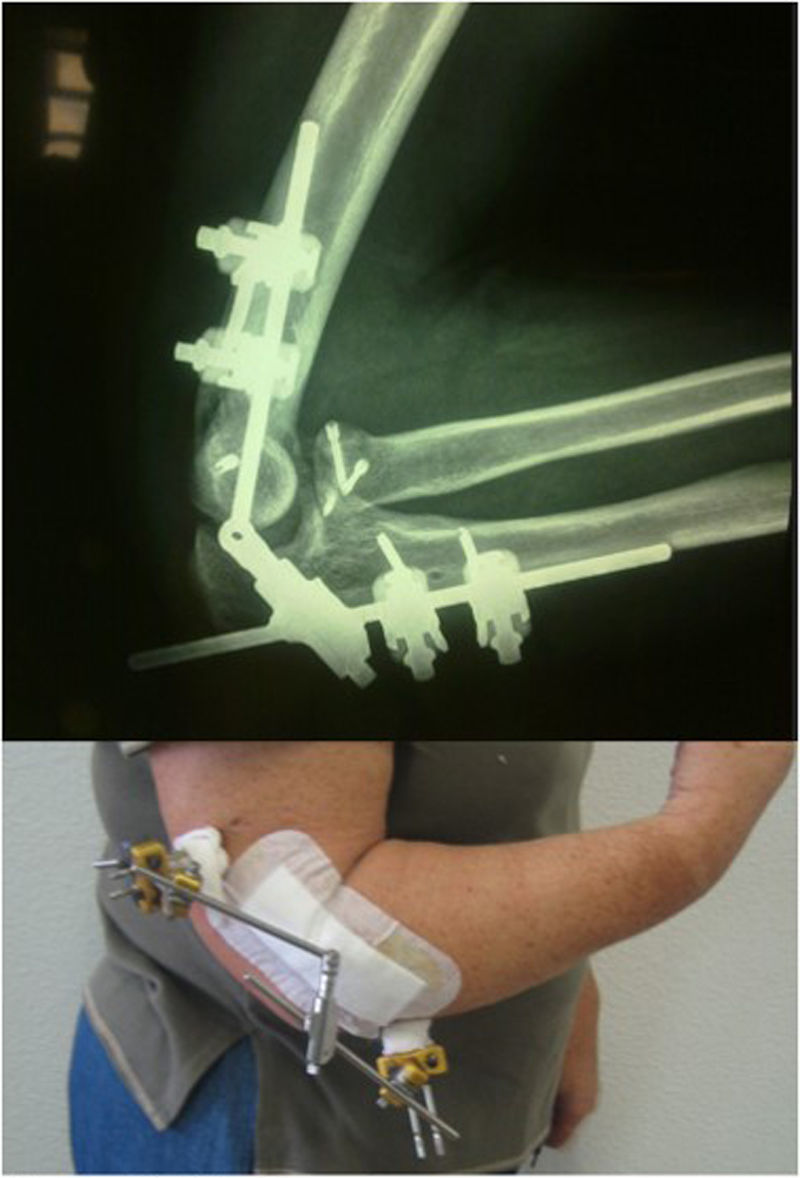
Lastly, if we had repaired the radial head, the coronoid process, the LCL and the MCL, and the elbow remained unstable, we would also proceed with an external fixator (Fig. 5).
Results
Mean age was 49 years, with a range between 17 and 78 years. Mean follow-up time was 18 months (with a minimum follow-up of 12 months and a maximum of 36 months).
Out of the total patients, 27 (44%) were women and 35 (56%) were men. The most common lesional mechanisms was falling from the individual's own height, although in up to 28% of cases high energy trauma (traffic accidents, hastiness, bicycle accidents, etc.) was the cause.
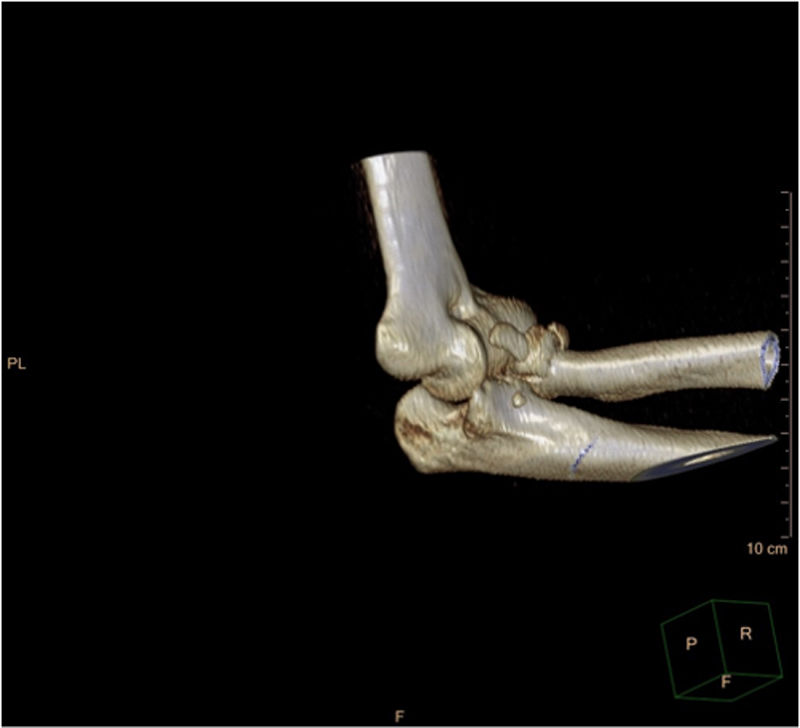
In all cases an X-ray was performed (anteroposterior and lateral projection) with additional computerised axial tomography (CAT) always being performed postreduction (Fig. 6).

In all cases a lateral Kaplan approach was performed, with the addition of a medial approach in 9 (14%) of cases.
In our series, the radial head was synthesised in 14 (22.5%) of cases, arthroplasty was performed in 45 (72.5%) with a pyrocarbon modular prosthesis (AscensionOrthopedics®) (Fig. 7) and no action was taken in 3 (5%) cases. The coronoid process was synthesised in 12 (19.3%) cases, with an (Acumed®) plate in 6 cases or with HCS (DePuy-Synthes®) screws or Acutrak (Acumed®) screws, in accordance with the senior surgeon's preference in the remaining cases. In 41 (66.2%) patients a transosseous suture was performed and in 9 (14.5%) no suture of this type was required.

In 100% of cases the LCL was repaired and in 9 (14%) the MCL had to be repaired as well due to insufficient stability. Furthermore, 22.5% of the patients required an EF due to instability, following all previously described procedures.
As we can see, the lesional spectrum is extremely wide, despite the fact that the injuries are encompassed within the terminology “terrible triad of elbow”, and there is a great variety of surgical techniques. We therefore consider that protocolised treatment should serve as a guide for taking one route or another, depending on the characteristics of each case.
In the immediate postoperative period the arm was kept immobile with a brachial antebrachial splinter at 100° extension and with the wrist in a neutral position for 3 weeks. After this, active assisted exercises of flexion and extension were allowed, avoiding the last 30° of extension. At week four the patient was referred for physiotherapy so as to progress with their range of movement. It should be taken into account that the post-surgical protocol was variable depending on the degree of stability obtained during surgery, to the extent that those who presented with high intraoperative stability were kept immobilised one or 2 weeks more.
Regarding functional results, a range of movement between 120°/−20° of flexoextension and 98°/85° of pronosupination and clinical assessment using the MEPS scale, obtained mean values of 92, being higher than or equal to 90 points in 54 (87.1%) of cases, between 75 and 89 points in 6 (9.7%) cases, between 60 and 74 points in 2 cases (3.2%) and below 60 points in no cases.
With regards to complications we obtained a total of 17 (27%) complications of different types. In 3 (17.5%) of cases infections were observed, 4 (23.5%) neurological lesions which consisted of 2 ulnar nerve entrapments and 2 radial nerve entrapments. There were 3 (17.5%) cases of stiffness, one (6%) ulnar impaction syndrome and one (6%) case where it was post-surgically observed that an intra-articular fragment had remained. From a radiologic viewpoint, 4 (23.5%) heterotopic ossifications were observed and one (6%) case of osteolysis of the radial prosthesis. In total, 6 further operations were performed, bringing the rate of reintervention to 9.6%. Two of these interventions were arthrolysis (arthroscopies or open surgery), 3 extractions of matter and one case of ulnar shortening after ulnar impaction syndrome.
DiscussionIn order to understand the approach to this lesion, we have to understand its physiopathology. Two types of stabilisers have been described: dynamic, which are those muscles that cross over the elbow joint and static. In addition to this, static stabilisers comprise those with greater entity or primary which are: the ulnar-humeral (the most important), the LCL, especially the lateral ulnar collateral fascicle, and the MCL, mainly the anterior fascile. The radial humeral joint, musculature inserted into the epycondyle and epitrochlear with a flexion pronator and extension supinator function and the joint capsule are considered secondary stabilisers.28
Although several studies describe conservative treatment in selected cases,3,12 our criteria is that this is a lesion requiring surgical treatment for bony lesions and for ligamentous lesions. There is consensus in the literature regarding the bases for appropriate treatment of the terrible triad of elbow being appropriate restoration of the bone and ligamentous elements so as to provide the elbow with enough stability to start exercising early movements.1,4,6,18,24
Although there is some consensus regarding the establishment of steps during terrible triad of elbow surgery, many controversial points remain, such as the approach route, whether the coronoid process should be repaired, or in which cases it would be necessary to repair the MCL.
The 2 most commonly used approaches are the Kaplan and Kocher approaches, which both allow for the radial head to be reached and synthesised, although repair of the LCL is easier from a Kocher approach since with the Kaplan approach difficulties may arise in repairing this ligament on having to liberate the residual part of the extensor digitorum communis of the epicondyl. Both approaches pose a risk to the posterior interosseous nerve, although we may reduce the risk, pronating the forearm to its maximum. On occasions, surgery should be complemented with a medial approach, either because we do not succeed in gaining access to the coronoid process through lateral approach, or because we wish to repair the MCL for greater elbow stability. If the fragment of the coronoid process is very large, it is usually necessary to raise the flexor carpi ulnaris, including the proximal flexor pronator mass.5,8
With regard to the radial head, the most frequent location of fractures is its anterior lateral quadrant.30 The current consensus is to maintain the radial head to achieve elbow stability,16,17,25 and therefore the option of its resection is rejected, but it is not yet clear which surgical technique is most recommendable. Warren et al.33 studied 24 elbows. They performed synthesis in 13 and arthroplasty in 11, but no statistically significant differences were found.
However, in general clinical practice, arthroplasty is reserved for fractures which may not be reconstructed, either because there are 3 or more fragments, because they are highly comminuted or because the joint surface has been greatly compromsed.17 There are many different implants on the market, the most highly used at present are the metallic implants, which provide good stability to the elbow and have good long-term results. Complications of this type of prosthesis are connected to the loosening of it and erosions of the humeral condyl, which appear to be related to the over dimensions of the implant head and high location of it. For this reason we should select smaller head sizes.13,31 Recently, Gauci et al.9 studied 65 patient s with radial head arthroplasy, out of which 92% presented with reabsorption at radial neck level but they did not present with mechanical failure and remained stable one year postoperatively. This was related to stress shielding, but without clinical repercussion. However radial head prostheses made of other materials such as silicon, have been withdrawn due to silicon synovitis and a high rate of implant rupture.32 In our series we initially tried synthesis of the radial head and if this was not possible due to extensive comminution, we opted for radial head arthroplasty. In our series we obtained a similar percentage of postoperative complications (35% in synthesis and 26% in arthroplasty). However, we consider that we should continue long-term follow-up to discern whether there are differences between both treatments.
Another key discussion relates to the treatment of coronoid process fractures. Traditionally, they were classified according to the Regan and Morregy23 classification but the O’Driscoll et al.20 classification is now used increasingly, based on CAT findings.
Type I fractures (those affecting the coronoid process tip) are often difficult to synthesise but according to some authors should be repaired since they are lesions which also affect the anterior capsule and may lead to instability in the anterior posterior plane.18 Synthesis of these small fragments may be achieved through harpoon or transosseous Lasso type sutures.11 Other authors consider that this type of lesions which only affect the most distal part of the coronoid process do not lead to instability in themselves and therefore when the radial head and LCL are repaired this would suffice.21 The type II fractures (antero-medial surface) and iii (base of the coronoids) are larger fractures, and we frequently have to resort to a medial approach and to preshaped screws or plates for proper synthesis. Grant et al.11 analysed a total of 40 elbows, where a Lasso type suture was performed (28) or synthesis with harpoon suture or screws (12). We found that those which were sutured were more stable, and those which were synthesised with screws had a greater tendency to implant failure and for those where anchorage was implanted there was a higher rate of pseudoarthrosis, which was statistically significant. In their work they concluded that the best results were achieved with Lasso type suture, but this was possibly due to the fact that this technique was used in smaller lesions which therefore had a lower instability component.
In our opinion O’Driscoll type I coronoid process should always be repaired when possible (e.g. if we resect the radial head for implantation of a prosthesis) and always in cases of instability after the radial head and LCL have been repaired.
LCL is a primary elbow stabiliser in the lateral area and we therefore always repair it. The most common lesion is a proximal avulsion at humeral level which occurs in 52% of cases. Avulsions of the humeral epicondyl (8%), intrasubstance ruptures (29%), avulsion in the distal ulnar (5%), avulsion in the proximal ulnar (2%) or a combination of them (5%)19 may also occur.
Lastly, there is no consensus as to whether the MCL should be systematically repaired. Several authors have found higher rates of heterotopic calcifications and lower ranges of movement in patients in which this ligament has not been repaired and they therefore recommend a “prophylactic” repair to improve postoperative results and to avoid the complications derived from ulnar neuropathy.29 Furthermore, there are authors who do not find any differences in the functionality scales and in the movement ranges and who therefore question the need for this repair.14 We have opted to repair it in the cases in which we have performed a medial approach to synthesise the O’Driscoll type II and III coronoid process lesions. In these cases we repaired the MCL with harpoon sutures.
When we have performed all these operations and if appropriate stability has not yet been obtained, some consensus exists for the use of an external fixator. Usage percentages vary between 8% and 26% according to the references,2,10,11,26 which is similar to the data found in our study.
In our series we observed that the higher the classification by Mason or O’Driscoll (Table 1) the higher the increase in the external fixator rate, which may help us to plan preoperatively. The more complex the fracture, the higher the rate of external fixators required. The exception to this was that no O’Driscoll type iii fracture needed an external fixator, the explanation for which may be that the fragment was larger, and once synthesised achieved greater stability than in types I and II, which were smaller fragments and more difficult to synthesise accurately.
The most common complication was that relating to heterotopical calcifications (12–43% depending on the series), but there were no related factors from a demographic viewpoint or surgical viewpoint or from time of surgery,27 with all data being similar to ours.
Notwithstanding, the clinical results which were assessed using the MEPS scale are satisfactory. This is so partly because the complications were temporary (neurapraxias) and because although complete mobility was not obtained, a useful range of movement for the patient's daily activities was.
ConclusionsTerrible triad of elbow are complex bony and lagmentous lesions where it is necessary to perform protocolised surgery but where there is still a complication rate ranging between 0% and 54%, depending on the study,2 and which was 27% in our series with the majority being minor or temporary.
Treatment should be sequential and its objective is to maintain a reduced, stable joint. The radial head must be synthesised and should this not be possible, prosthesis introduced. The coronoid process fracture should be synthesised when possible and the larger its size the more so. The lateral ligamenous complex must always be repaired and when there is residual instability the use of an external fixator should be assessed.
Level of evidenceLevel of evidence iv.
FinancingNo type of financing was received for the undertaking of this article.
Conflict of interestsThe authors have no conflict of interests to declare.
Uncited reference
34.
Please cite this article as: Álvarez Muñoz M, Pardo García JM, García Lamas L, Porras Moreno M, Jiménez Díaz V, Cecilia López D, et al. Tratamiento quirúrgico protocolizado de las tríadas terribles de codo. Resultados y complicaciones. Rev Esp Cir Ortop Traumatol. 2019;63:281–288.
