



Evaluation of clinical and functional outcome of ray resection in paediatric population and description of key aspects of surgical technique.
Material and methodsWe performed a retrospective review of all patients undergoing surgery between 2010 and 2015. Inclusion criteria: one or more ray resections of the hand and a minimum of one year follow-up. Evaluation of clinical characteristics, functional and cosmetic results, complications, need for psychological support and patient or family satisfaction.
ResultsFour patients met the inclusion criteria. The mean age at surgery was 5 years (range, 1–14 years). Aetiology was: fibrolipomatous hamartoma, traumatic amputation, radial deficiency and complex syndactyly. Second ray was resected in three patients and third and fourth ray in one. No finger transfer was performed. No immediate post-operative complications were found at the final evaluation. None of them needed psychological support. All the patients showed excellent clinical and functional results with a high grade of satisfaction.
DiscussionRay resection of the hand has been used as salvage procedure in patients with vascular lesions, tumours, trauma, infections or congenital malformations. There are only a few published studies including small samples in adults or case reports, with no references in the paediatric population.
ConclusionRay resection of the hand is a useful and safe technique in paediatric population, obtaining excellent cosmetic and functional results in those cases in which it is impossible to preserve one or more fingers.
Valoración de los resultados clínicos y funcionales de la resección completa de los radios de la mano en población pediátrica y descripción de los aspectos técnicos más relevantes de la cirugía.
Material y métodoEstudio retrospectivo observacional de pacientes intervenidos en el periodo comprendido entre 2010–2015. Criterios de inclusión: resección de uno o más radios de la mano y seguimiento mínimo de un año. Evaluación de las características clínicas, resultados funcionales y estéticos, complicaciones, necesidad de apoyo psicológico y grado de satisfacción.
ResultadosCuatro pacientes cumplieron criterios de inclusión. La edad media fue de 5 años (rango 1–14 años). Las causas fueron: hamartoma lipofibromatoso, amputación traumática, deficiencia radial y sindactilia compleja. El segundo radio fue resecado en tres pacientes y el tercer y cuarto radio en un paciente. No se realizó transferencia de radios adyacentes. No existieron complicaciones postoperatorias ni durante el seguimiento. Ningún paciente precisó ayuda psicológica. Todos presentaron excelentes resultados estéticos, funcionales y con un alto grado de satisfacción.
DiscusiónLa resección completa de uno o más radios de la mano se utiliza como técnica de rescate en pacientes con lesiones vasculares, tumores, traumatismos, infecciones o malformaciones congénitas. Las publicaciones existentes son pequeñas series en pacientes adultos o casos clínicos aislados, no existiendo apenas referencias en población pediátrica.
ConclusiónLa resección de radios de la mano es una técnica útil y segura en la población pediátrica que proporciona excelentes resultados estéticos y funcionales en aquellos casos en los que es imposible la preservación de uno o varios dedos.
The complete resection of one or several rays of the hand is a technique used in those cases in which due to infection, tumour, trauma or congenital causes it is impossible to preserve the fingers. This was classically indicated in cases of necrosis due to ischaemia, severe dysfunction of the proximal interphalangeal joint and traumatic amputation at the level of the proximal finger in the adult population. This technique has not been very popular due to the resulting loss of strength and associated grasping capacity.1 The presence of a finger that is painful and rigid, with sensitivity alterations and which is either too long or too short may affect hand function and dexterity.
The majority of publications on this technique are about small series of adult patients or isolated clinical cases,1–7 with hardly any references to a paediatric population.8–11 The decision to perform a resection of the rays of the hand is difficult for the surgeon as well as for the patient, and most especially for paediatric patients. The indication of surgery is often rejected at first by the parents, due to its social repercussions and affect on future occupations.
This work aims to evaluate the clinical and functional results of complete resection of the rays of the hand in children, and also describes the most important technical aspects of the surgery involved.
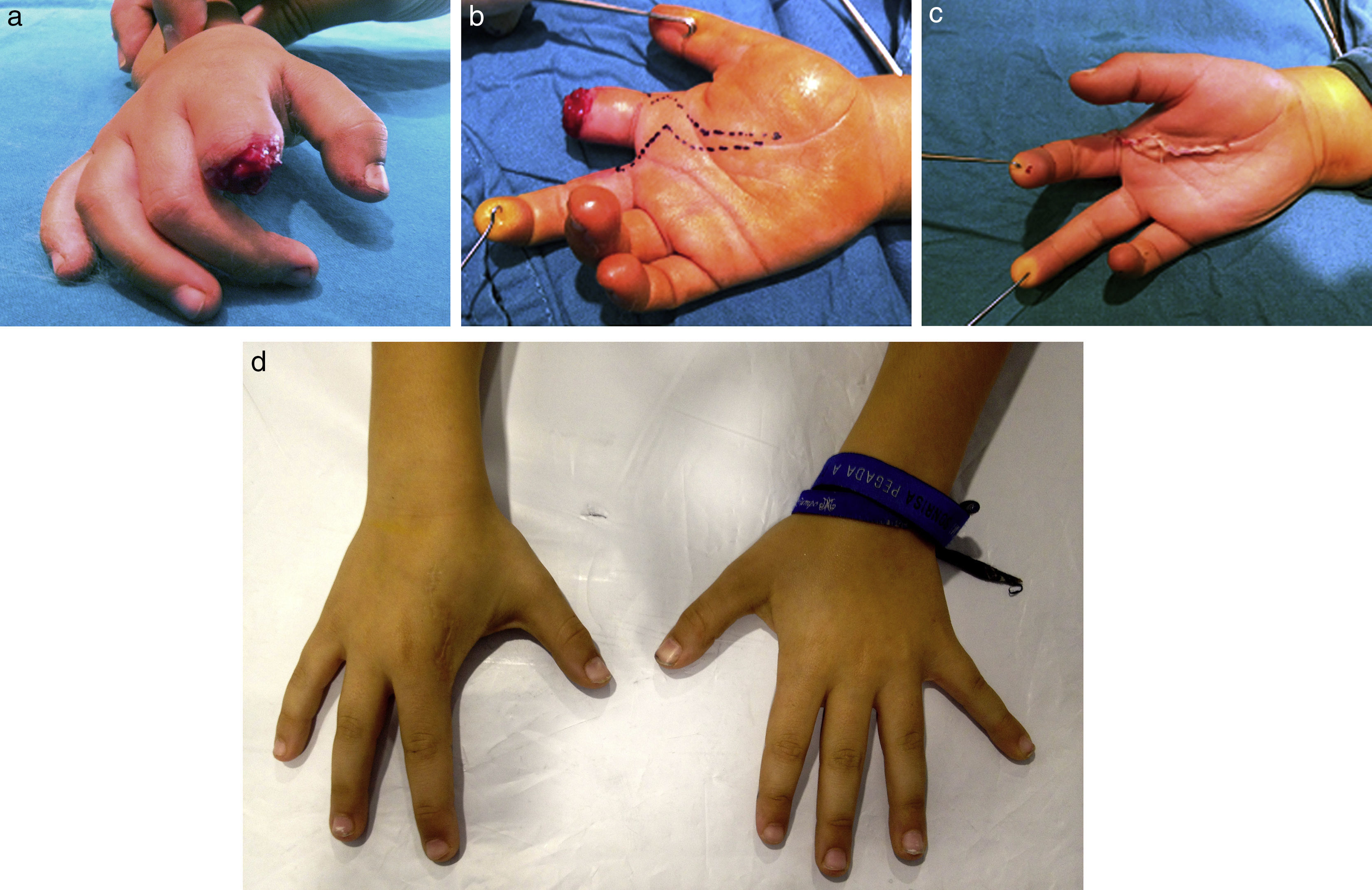
Material and methodA retrospective observational study of 4 patients operated in our hospital from 2010 to 2015. The inclusion criteria were: paediatric patients operated for the resection of one or more rays in the hand and with a follow-up period longer than one year. The average age of the patients was 5 years old (range 1–14 years). The reason for resection was macrosyndactyly associated with lipofibromatosis (Flatt type I macrodactyly), the after-effects of complex syndactyly, ray deficiency and traumatic amputation of the index finger following an animal bite (Fig. 1). In three of the patients ray resection was undertaken as the initial procedure, and in one case it was a secondary procedure. Surgery took place under general anaesthetic with an ischaemia sleeve. Skin flaps were designed including the ray to be resected, preventing scarring over the commissure. Finger veins and arteries were ligated and cut. The nerves were isolated and cut proximally in the fat of the palm to prevent neuromas. In all cases an extraperiostic resection was performed of the ray, including the metacarpal, while preserving its base with the tendon insertions of the extensor carpi radialis longus or extensor carpi radialis brevis. The resection was distal to proximal and from the radial to the ulna, with shears. In the volar approach the superficial and deep flexor tendons were cut proximal to their insertion in the lumbrical muscles. The proximal resection made it possible to retract the tendons proximal to the carpal tunnel, thereby preventing compressive symptoms and fibrosis. In the cases of resection of the second ray the neurovascular commissural package for the middle finger was preserved. In no case was adjacent tendon and/or ray transfer performed as the remaining rays were left parallel. In one patient with the resection of two rays the deep transverse metacarpal ligament was repaired using Ogino's technique, with the aim of keep the correct hand alignment and morphology. In no case was it necessary to disarticulate the whole metacarpal. The skin was closed without tension. The patients were immobilised with a dorsal antebrachial splint with the hand in the intrinsic-plus position. The splint was removed two weeks after the surgery to check the surgical wound, after which it was kept on for two more weeks. Passive rehabilitation exercises commenced one month after surgery to prevent postoperative rigidity.
 Traumatic amputation following animal bite. (b) Surgical image with skin flap design. (c) Postoperative image. (d) Clinical appearance after 5 years evolution.")
A subjective and functional evaluation was undertaken in all cases. The parents were given a questionnaire for the subjective evaluation, on cosmetic appearance, sensitivity, the presence of pain in the surgical scar, cold intolerance and degree of satisfaction with the surgery (0: very satisfied, 1: satisfied, 2: dissatisfied and 3: very dissatisfied). The history also shows capacity for performing basic everyday activities (writing, handling toys and using scissors) in four degrees (0: without difficulty, 1: slight difficulty, 2: moderate difficulty and 3: incapacity). All of the patients were offered psychological help.
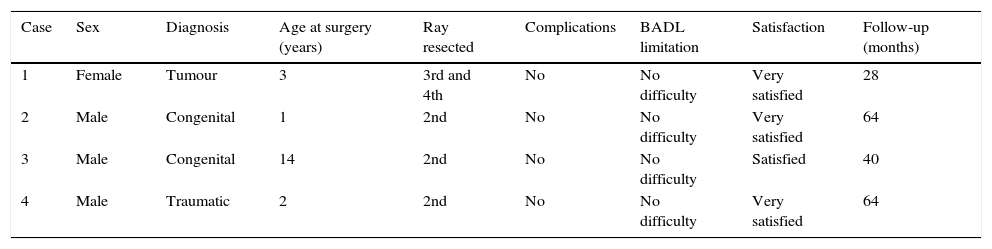
ResultsFour patients fulfilled the inclusion criteria. The average age was 5 years old (range 1–14 years old). The follow-up lasted for 48 months (range 28–64 months). Three patients were male. The right hand was involved in all cases. Respecting the aetiology, in one case this was a tumour (Flatt type I macrodactyly), in two cases it was congenital malformation (hypoplasia of the index finger secondary to ray deficiency and the after-effects of complete-complex syndactyly), and with one case of traumatic amputation due to animal bite. The second ray was resected in three patients and the third and fourth rays were resected in one patient. No adjacent rays were transferred. No complications arose during the postoperative period or during the follow-up. No patient eventually had pain in the surgical scar or any increase in cold sensitivity. No patient had limitations in the performance of their everyday and school activities. The majority of the patients stated they were limited in their use of scissors but not for eating or writing. No patient needed psychological assistance. All of the patients were found to feel a high level of satisfaction with the cosmetic results (Table 1).
Demographic and clinical data.
| Case | Sex | Diagnosis | Age at surgery (years) | Ray resected | Complications | BADL limitation | Satisfaction | Follow-up (months) |
|---|---|---|---|---|---|---|---|---|
| 1 | Female | Tumour | 3 | 3rd and 4th | No | No difficulty | Very satisfied | 28 |
| 2 | Male | Congenital | 1 | 2nd | No | No difficulty | Very satisfied | 64 |
| 3 | Male | Congenital | 14 | 2nd | No | No difficulty | Satisfied | 40 |
| 4 | Male | Traumatic | 2 | 2nd | No | No difficulty | Very satisfied | 64 |
The resection of one or more complete rays of the hand is used when it is impossible to preserve a functional finger due to vascular causes, a tumour, trauma, infection or congenital deformity. In 1924 Bunnell described this technique as a rescue treatment in a patient who presented an alteration in a proximal interphalangeal joint.
Regarding the age of presentation, we present four cases of resection of one or two rays of the hand in a paediatric population with an average age of 5 years old. The majority of publications are about adult patients.2,3,9,12–16 There are hardly any published cases of paediatric cases, and those which exist are isolated cases8,10 or paediatric patients in a larger series.9,17
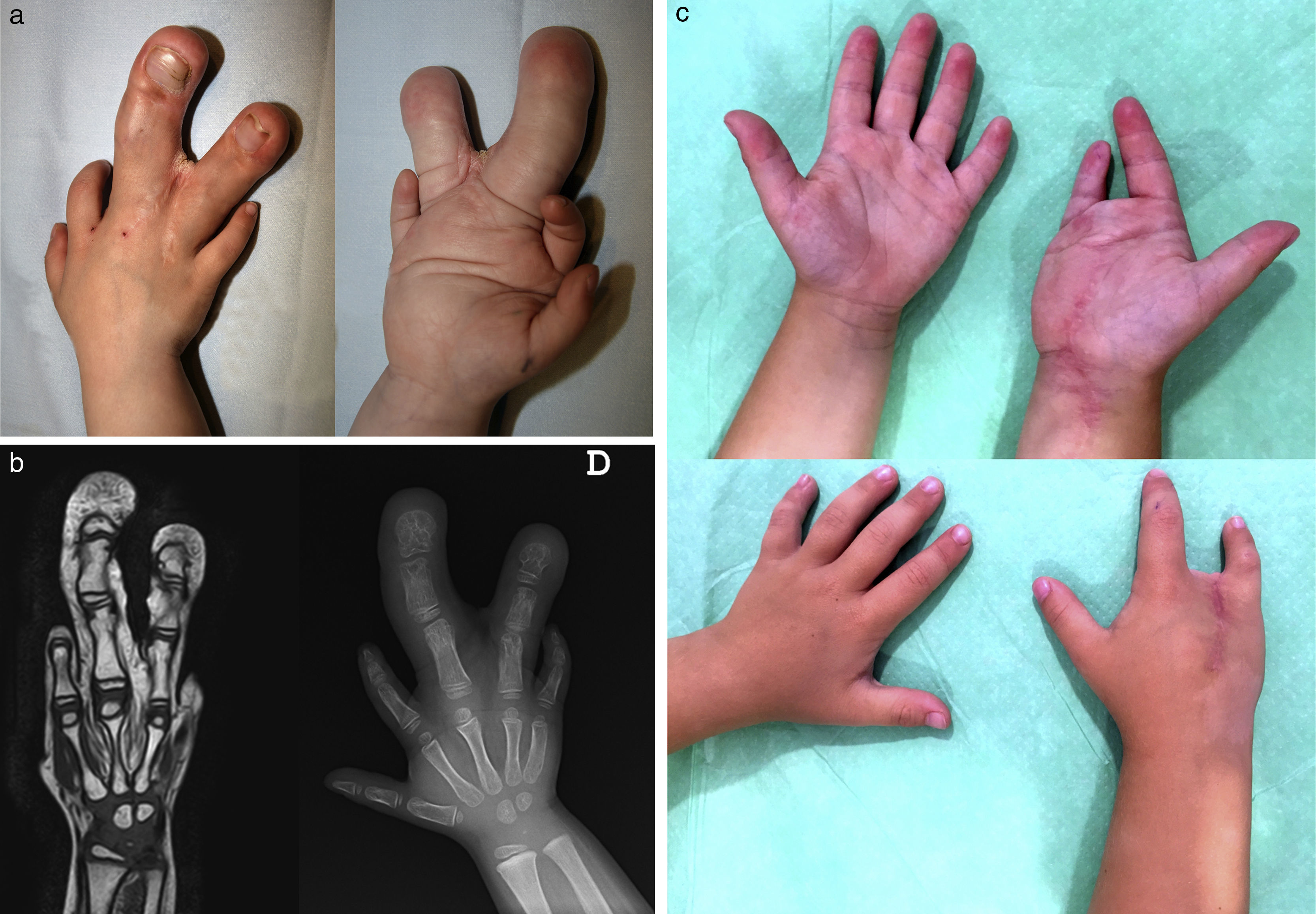
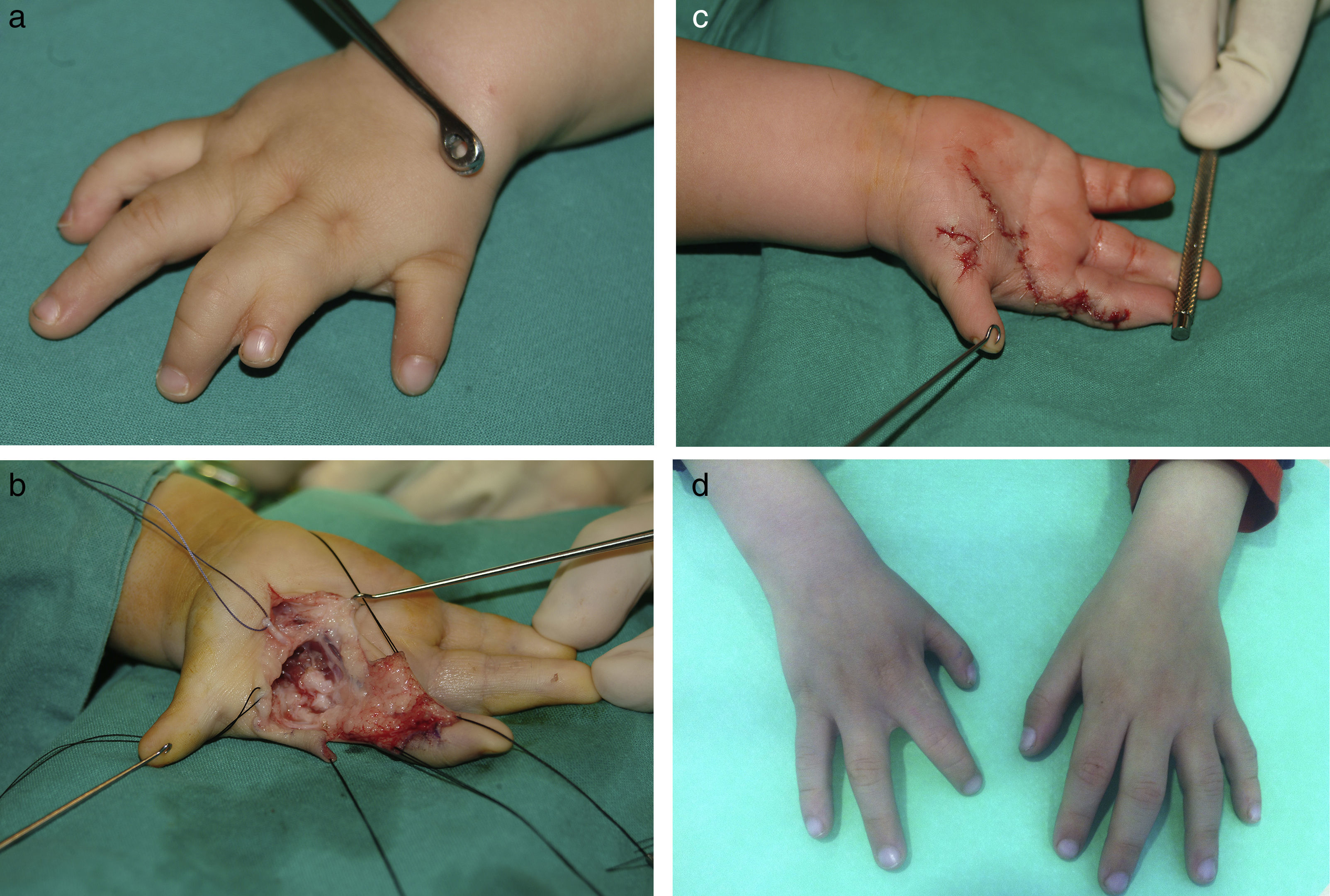
Numerous authors have used this technique to treat tumoural lesions by resecting one ray6 or several rays.4,5 The majority of publications on macrodactylya are isolated cases in the adult population.12–15 Two series exist in the paediatric population,9,17 and these present lipofibromatous hamartomas in which resection of the ray was not performed as the primary procedure, together with an isolated case of resection of the first and second rays in association with the transfer of the middle finger.8 The indications for hand ray resection in cases of macrodactylya are when deformity is progressive or when it is necessary to perform several surgical operations with the result of a rigid and hardly functional finger. In the series of Cerrato et al.17 the results of a retrospective study of 21 paediatric patients with hand macrodactylya are shown. Gluck and Ezaki11 used this technique to treat macrodactylyas in which the size of the affected finger was far larger than the size of their parent's finger, as we did in our case (case 1). Hand ray resection has also been used as the primary procedure or as a rescue therapy following traumatic amputation or severe trauma of the fingers.2,7,16,18 One patient (case 4) suffered traumatic amputation at the level of the proximal interphalangeal joint following a horse bite. The finger was completely traumatised and the wound looked anfractuous, so that it was decided not to re-implant it. The majority of works in paediatric populations are about operations due to congenital malformations9 or tumours.8,17 We present two patients with congenital malformations. One patient had rigidity of the index finger following complete-complex syndactyly (Fig. 2). Another patient presented ray deficiency with hypoplasia of the index finger associated with syndactyly (Fig. 3). In both cases it was decided to resect the index finger and reconstruct the first commissure.
 After-effects of complex syndactyly. (b) Intraoperative image. (c) Results after 3 years evolution.")
 Ray deficiency associated with syndactyly. (b) Intraoperative image. (c) Postoperative image. (d) Clinical results after 5 years evolution.")
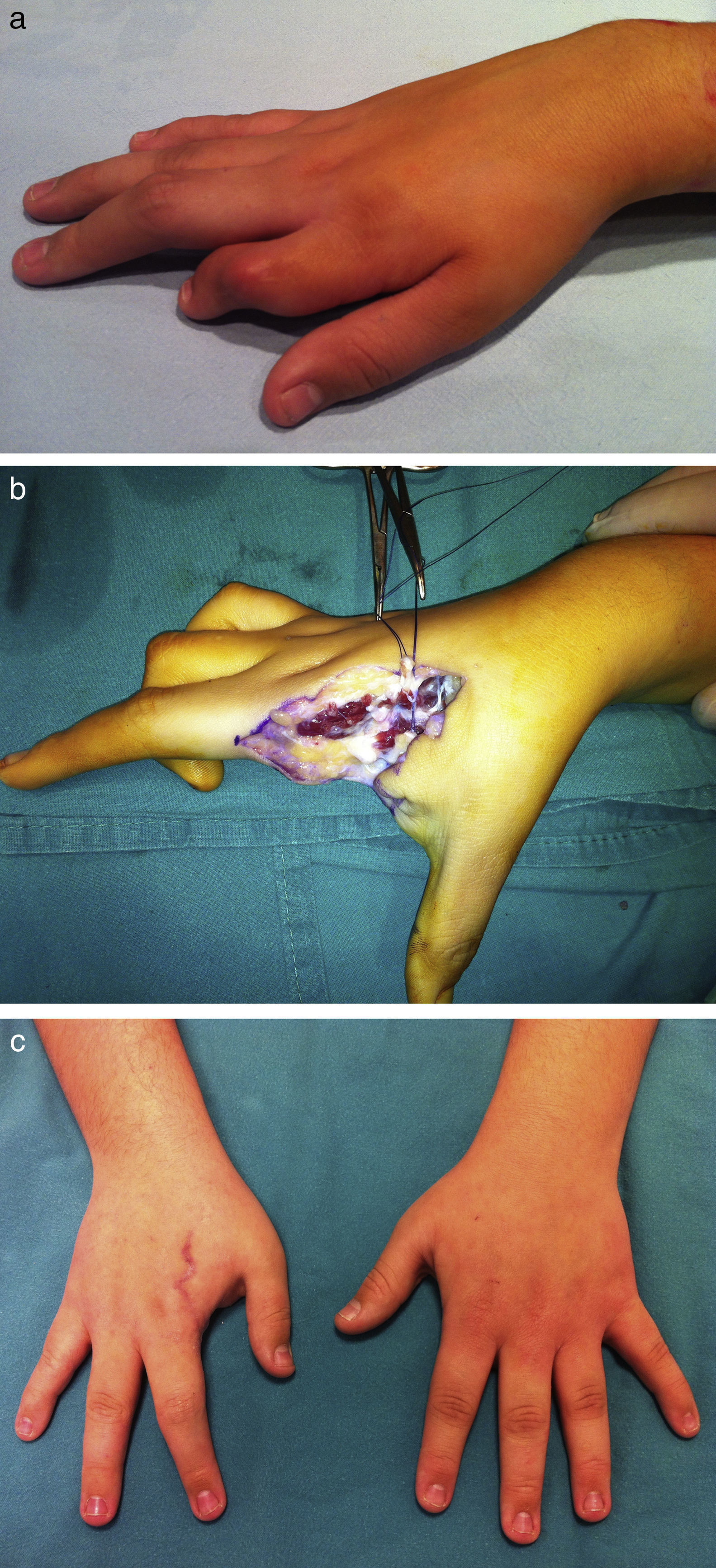
In our series we present three cases of resection of the second ray of the hand, this being the ray that is the most frequently involved in the majority of series.3,6 As other authors1 observe, the operated patients transferred the skills and abilities of the resected ray to the adjacent rays, above all for the pincer movement of the first and third rays. In one patient the third and fourth rays were resected due to Flatt type I macrodactyly (case 1). There are three works in the literature on two-ray resections4,8 and partial resections of the hand.4,5 These publications describe resections of the second-third ray and the fourth-fifth ray4,5 as well as resection of the first and second ray with transfer of the middle finger.8 No cases are described in the literature of resection of the third and fourth ray (Fig. 4).
 Macrodactyly due to lipofibromatous hamartoma. (b) X-ray image and magnetic resonance image. (c) Results after 2 years evolution.")
The majority of the works in adults show acceptable functional results in terms of strength, hand grasping capacity and early resumption of work. In paediatric patients we observed poor acceptance of the condition in the initial months, with a tendency to hide the hand and avoid using it in play. This attitude disappeared after a few months, without any restrictions being observed for play and/or school activities (Figs. 2 and 3).
Numerous ray resection techniques have been described. Some authors have shown the benefits of ray resection to be associated with the transfer of the adjacent metacarpals, suggesting an improvement in the cosmetic appearance and capacity to use scissors.19 Other authors have preferred to perform a disarticulation at the carpal–metacarpal level to prevent the dorsal protrusion of the metacarpal following incomplete resection,1 although this has the disadvantage of causing chronic wrist pain due to exposure of the joint cartilage. In our series we performed one ray resection while preserving the metacarpal base to keep the tendon insertions if the extensor carpi radialis longus and brevis. In the case of the patient with resection of two rays of the hand associated with macrodactyly (case 1), the transverse deep metacarpal ligament was also reconstructed to keep hand anatomy, giving a highly satisfactory cosmetic and functional result.
The limitations of our work are that it lacks objective tests of functionality, as no functional tests have been translated and validated for the paediatric population; the small number of cases included, as these pathologies are not very common in children and the technique is only used in cases in which it is impossible to preserve the finger. We underline that this is the first paediatric series which evaluates the clinical and functional results of complete resection of one or several rays in the hand, in a heterogeneous group of patients.
ConclusionThe complete resection of one or several rays of the hand is a safe and definitive technique in those cases where it is impossible to perform surgery that preserves the finger. The most common reasons for surgery in infancy are tumours, congenital malformations and traumatic amputations. Although the resection of one or more hand rays is rejected at first by the parents, due to its social repercussions and effect on future occupations, the cosmetic and functional results are excellent, with a high degree of satisfaction over the medium term. Long-term studies are necessary, as well as the development of functional evaluation scales that are validated for patients of this type.
Level of evidenceLevel of evidence IV.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed are in accordance with the ethical norms of the relevant human experimentation committee, the World Medical Association and the Helsinki Declaration.
Confidentiality of dataThe authors declare that they followed the protocols of their centre of work on the publication of patient data.
Right to privacy and informed consentThe authors obtained the informed consent of the patients and/or subjects referred to in the paper. This document is held by the corresponding author.
Conflict of interestThe authors have no conflict of interests to declare.
Please cite this article as: Martínez-Álvarez S, Maldonado-Morillo A, Vara-Patudo I, Martínez-González C, Miranda-Gorozarri C. Resección de radios de la mano en pacientes pediátricos. Rev Esp Cir Ortop Traumatol. 2017;61:233–239.
