


Osteosynthesis hardware removal is one of the most frequent practices in Orthopaedic electives surgeries and is usually carried out guided under fluoroscopy. There are other tools such as ultrasound that allow us to visualise the hardware with the advantage of being free of ionising radiation and with better availability. The objective of our study is to analyse the results obtained in patients undergoing hardware removal in the operating room under ultrasound assistance and local anaesthesia.
Material and methodsA descriptive study was carried out collecting variables such as demographic data, reason for the removal, pain during the procedure and in subsequent days, as well as the duration and rate of success of the procedure and the degree of satisfaction.
ResultsWe obtained a 100% success in ultrasound-guided extraction without the need for conventional radiology, with a mean VAS of 1.91 and need for subsequent analgesia in 36.4% of the cases, with syndesmotic dynamisation being the most frequent reason for intervention.
ConclusionUltrasound is a useful tool in osteosynthesis hardware removal, and that may be sufficient by itself; also saving health personnel and patients from ionising radiation resulting from the use of conventional fluoroscopy.
La extracción de material de osteosíntesis es una de las prácticas más frecuentes en los quirófanos de traumatología, y habitualmente se realiza guiado bajo escopia. Otras herramientas más accesibles, como la ecografía, permiten la visualización del material con la ventaja de evitar las radiaciones ionizantes. El objetivo de nuestro estudio es analizar los resultados obtenidos en pacientes intervenidos de extracción de material de osteosíntesis en el quirófano bajo asistencia ecográfica y anestesia local.
Material y métodosSe realizó un estudio descriptivo recogiendo variables como los datos demográficos, el motivo de la extracción, el dolor durante el procedimiento y en días posteriores, así como la duración y el éxito del procedimiento y el grado de satisfacción.
ResultadosSe obtuvo un éxito en la extracción ecoguiada sin precisar radiología convencional del 100%, con una EVA media de 1,91 y necesidad de analgesia posterior en el 36,4%, siendo la dinamización sindesmal el motivo más frecuente de intervención.
ConclusiónLa ecografía supone una herramienta útil en la extracción de material de osteosíntesis, la cual permite ahorrar al paciente y al personal sanitario las radiaciones ionizantes consecuencia del uso de la fluoroscopia convencional.
Osteosynthesis hardware removal (OHR) is one of the routine surgical processes that a trauma surgeon performs in their daily practice, and can exceed 5% of scheduled interventions.1 The indication for extraction is usually based on discomfort related to the location of the osteosynthesis hardware without this, in principle, being attributed to another cause, and is not regularly recommended by any guideline in asymptomatic patients. The segment in which they are most commonly performed is the distal leg, in the ankle region (4.2% of the total). Despite being routine operations, they are not risk-free and complications have been reported, such as neurovascular injury or of other noble structures, such as ligaments and tendons, as well as other adjacent problems, including haematomas or seromas.2 The traditional extraction technique is performed in the operating room under local anaesthesia. Scopy is usually, albeit not necessarily used, as an accessory tool to verify the position of the osteosynthesis hardware and to be able to locate and remove it faster and with less soft tissue injury.3 However, it is not the only imaging test available. Others exist, such as ultrasound, which also has the advantage of avoiding ionising radiation and the expense of radiology technical staff in the operating room, since it may be performed in the outpatient department.4–6
The objective of our study was to analyse the outcomes obtained in patients operated on for ultrasound-guided osteosynthesis hardware removal in the operating theatre (instead of conventional plain X-ray) and local anaesthesia. We assessed its efficacy, complications and patient comfort to determine whether it could be used as another alterative in these cases.
Material and methodsThis study was conducted and prepared in keeping with the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) statement initiative. We present a descriptive study of the patients who underwent surgery in our centre for ultrasound-guided osteosynthesis hardware removal between September 2022 and January 2023. The following data were collected: sex; age; reason for osteosynthesis hardware; type of hardware and reason for removal; time from the initial surgery to extraction; pain during the intervention measured using the VAS scale; need for postoperative analgesic medication; duration of the removal procedure; prescribed prophylactic antibiotic treatment; incidences in the surgical wound, and degree of satisfaction with the procedure.
As an inclusion criterion, patients over 14 years of age were included (with the need to sign an information sheet by a legal guardian or parents for patients aged between 14 and 18 years) with osteosynthesis hardware implanted after a fracture or other condition included in the surgical waiting list for extraction of osteosynthesis hardware with local anaesthesia, as long as at least 6weeks had passed since the initial surgery. Acceptance by the patient and the commitment to carry out a minimum follow-up of 3months from the withdrawal were included as criteria. Only those patients included on the surgical waiting list for the extraction of 1 or 2 screws in the leg segment were considered. The procedure was thoroughly explained to all patients and they signed the relevant informed consent. All techniques were performed under correct asepsis conditions and with resuscitation equipment typical of the operating room environment, with physicians from the anaesthesiology department to minimise possible complications that could have arisen. Simple fluoroscopy was also available in the operating room in case ultrasound visualisation was not possible. After the intervention, all patients received a telephone call from an independent evaluator attached to the responsible medical department and were scheduled for consultation to record the variables included in this study.
Surgical techniqueBefore beginning the procedure, the latest X-rays obtained were analysed to document the position of the osteosynthesis hardware to be removed. Once in the operating theatre, the anaesthesia service monitored the patient (O2, saturation, heart rate, electrocardiography and blood pressure) and channelled a 14-24G peripheral line that was available in case intravenous administration of serum therapy or drugs was necessary. The availability of a fluoroscope was ensured in case ultrasound visualisation of the hardware to be removed was not possible. After this the procedure was as follows:
- 1)
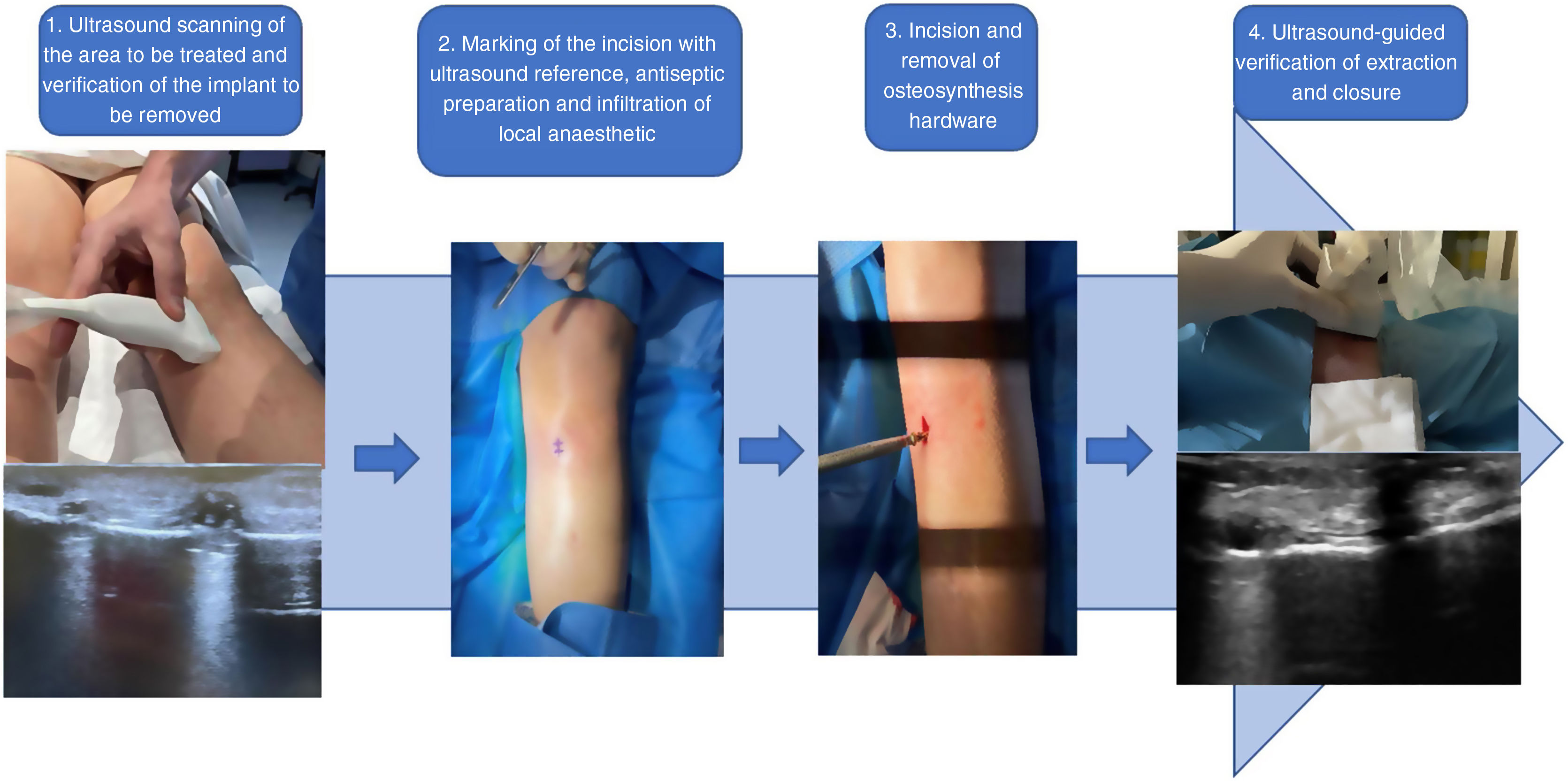
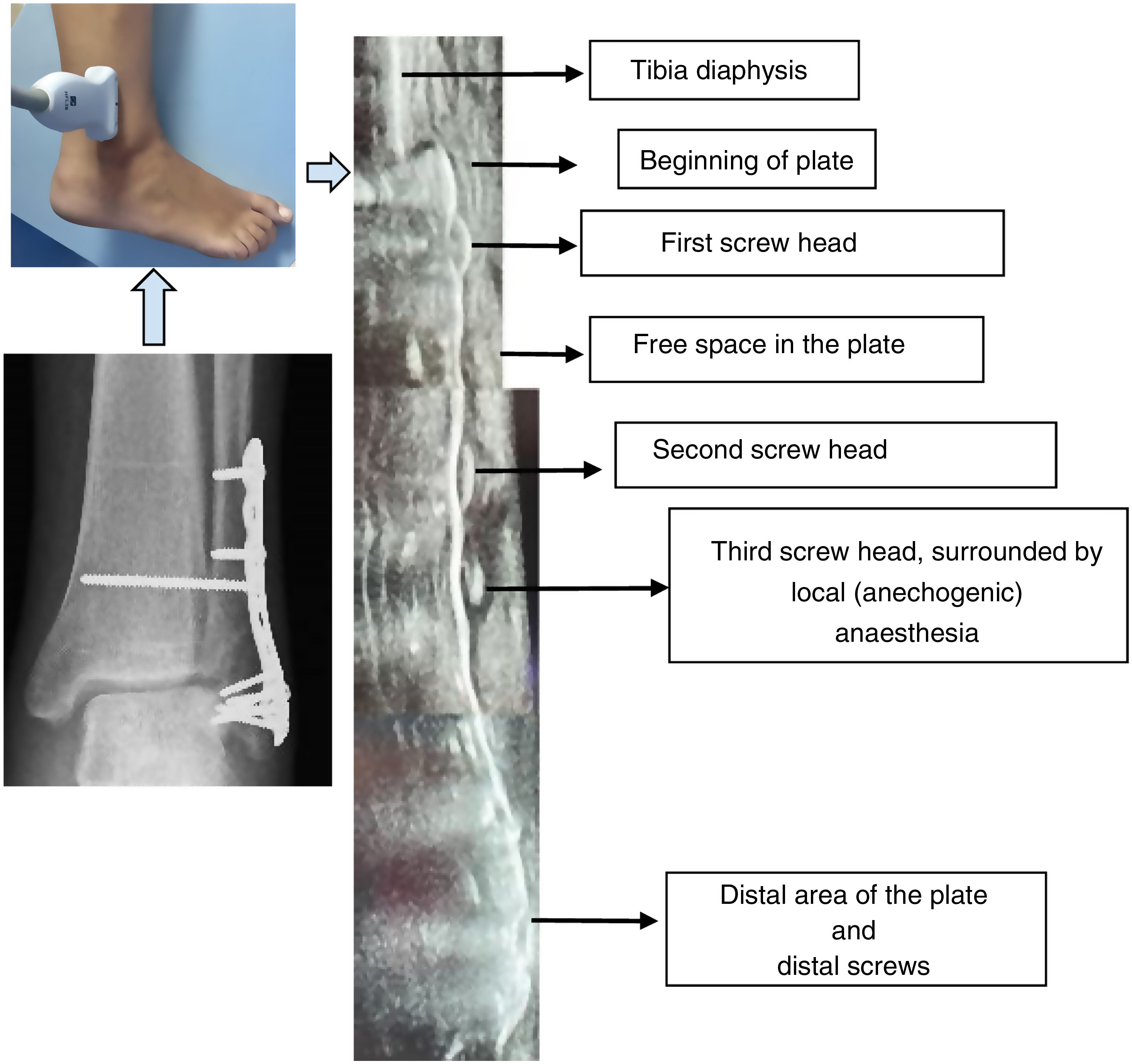
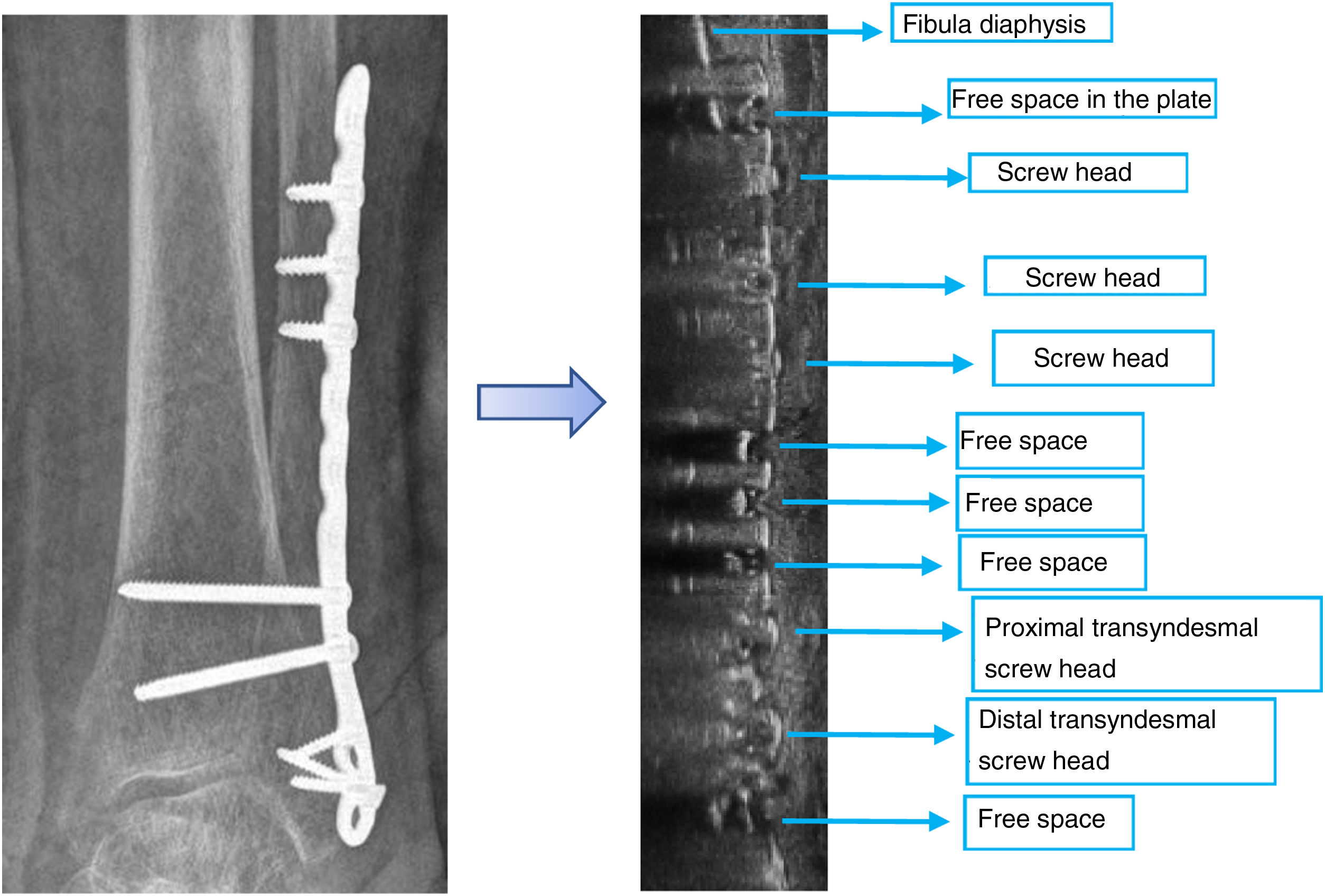
In supine position and using a Sonoscape X3 with lineal 4–16MHz probe in longitudinal and transversal projection to the tibia/fibula diaphyseal axis, the segment to be treated was scanned, visualising the osteosynthesis hardware to be removed and its relationship with any noble structures at risk. We identified all the screw heads for the exact location of the hardware to be removed, stopping and marking in the centre of the probe, the screw to be extracted, together with any major structures at risk in the area (Figs. 1 and 2).
 Figure 2.
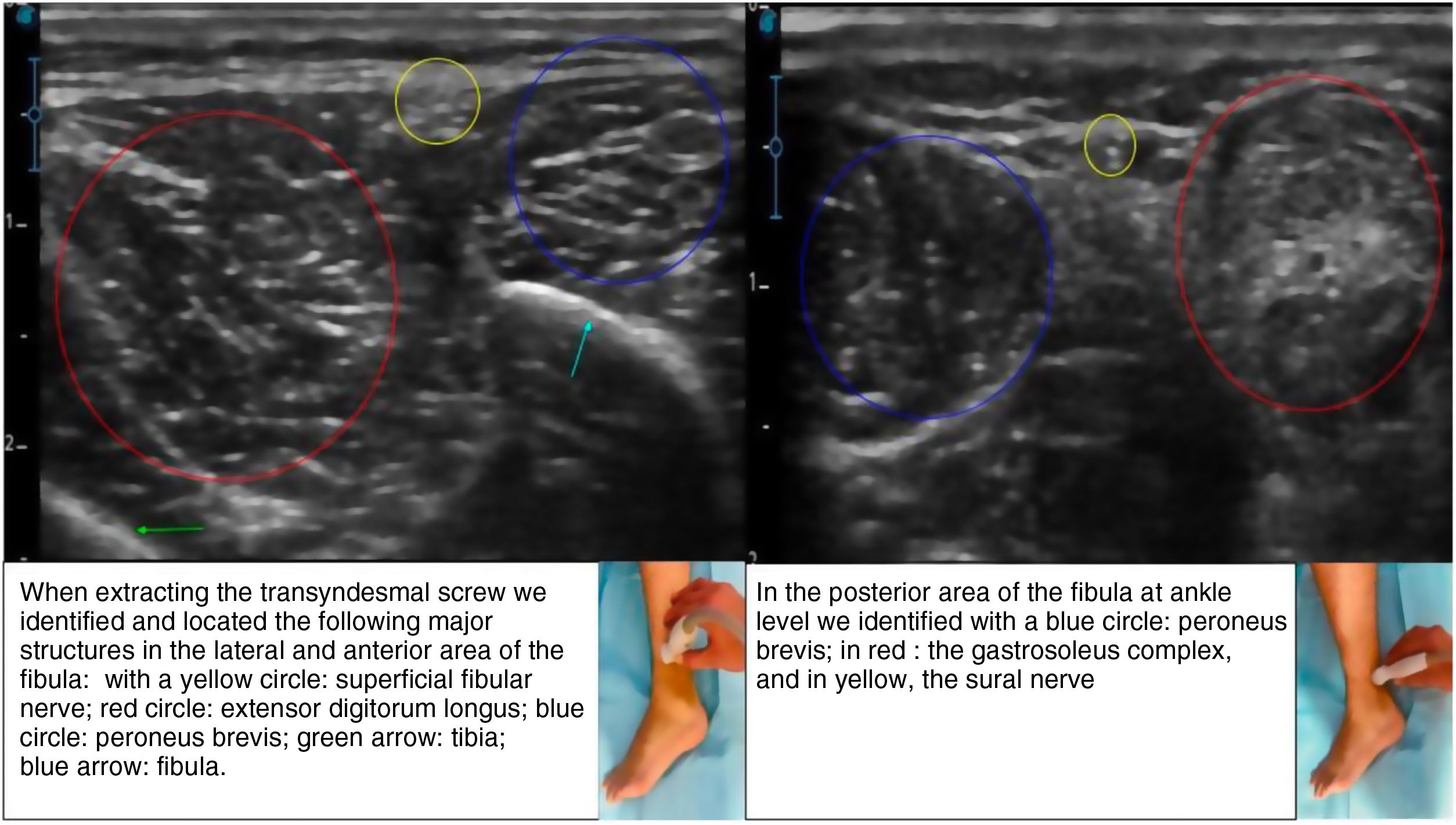
Figure 2.Identification by ultrasound of neurovascular and ligamentous structures. When extracting the transyndesmal screw we identified and located the following major structures in the lateral and anterior area of the fibula: with a yellow circle: superficial fibular nerve; red circle: extensor digitorum longus; blue circle: peroneus brevis; green arrow: tibia; blue arrow: fibula. In the posterior area of the fibula at ankle level we identified with a blue circle: peroneus brevis; in red: the gastrosoleus complex, and in yellow, the sural nerve.
(0,33MB). - 2)
The site was prepared with alcoholic chlorhexidine and sterile cloths. In the area of the previously indicated mark, with ultrasound guidance, 2–4ml of 1% mepivacaine was infiltrated into the skin, subsequently reaching down to the osteosynthesis material. Infiltration could also be guided by ultrasound.
- 3)
Following this, incision was made in the skin and subcutaneous cellular tissue, releasing adhesions until the screw head was reached. After cleaning the surrounding material, the specific hardware was removed. Lavage with physiological saline solution was then performed.
- 4)
Verification of correct extraction with an ultrasound can be carried out optionally. However, the length of the extracted hardware, if it has several screws around it, or the absence of this if it is a single screw, would confirm correct extraction. The procedure was completed with skin closure and dressing (Fig. 3).



Immediate confirmatory postoperative X-rays were not obtained, but were requested when necessary for subsequent clinical reviews.
Data were analysed using SPSS® for Mac (SPSS, Inc., an IBM company, Chicago, Illinois, USA). For quantitative variables, measures of central tendency and dispersion were calculated and normality was checked with the Shapiro–Wilk test. The results of the qualitative variables were expressed as percentages and frequencies, and the quantitative variables as mean, proportion and/or percentage.
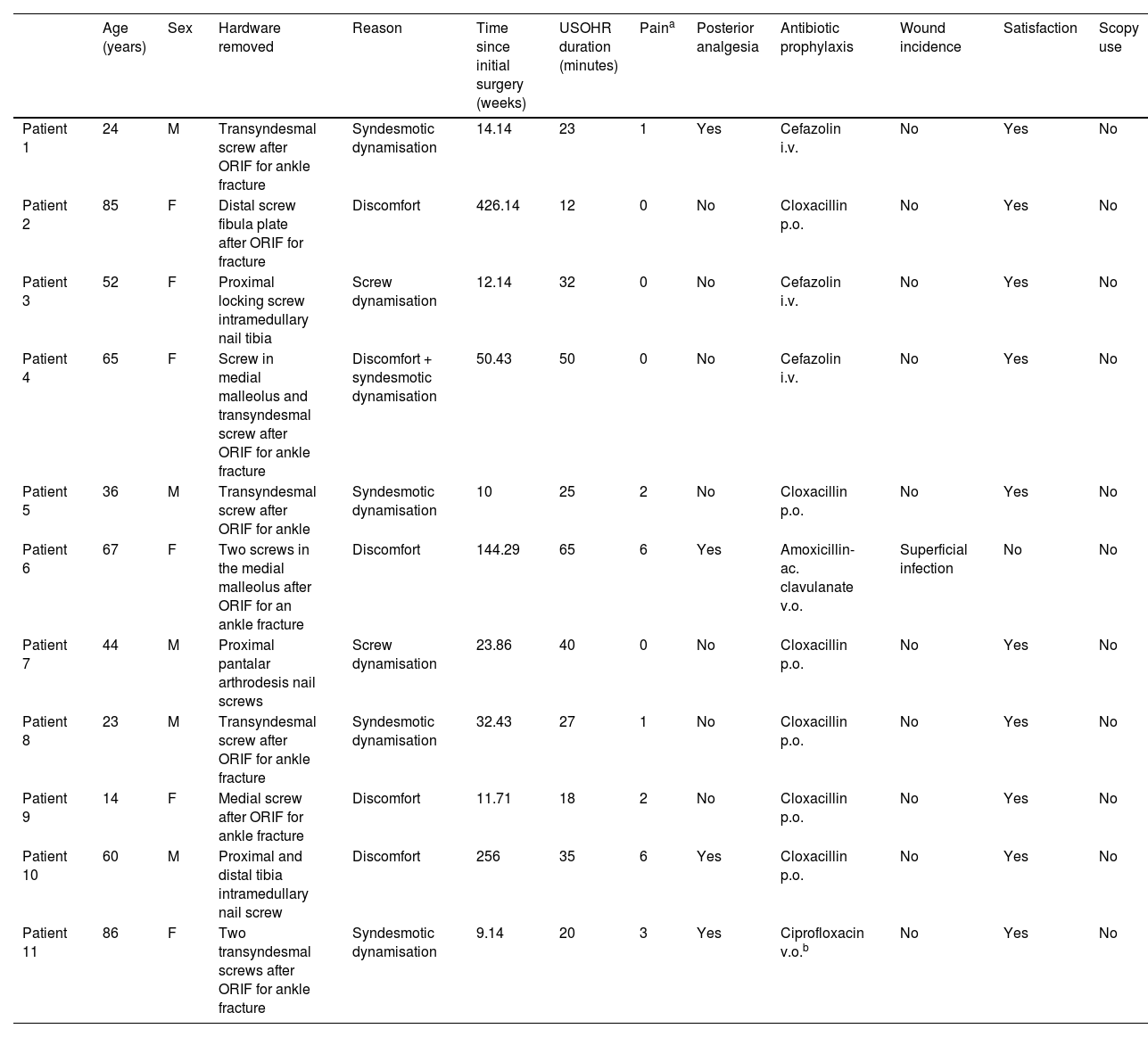
ResultsEleven patients were included in the study. Demographically, the sample distribution comprised 5 men (45.45%) and 6 women (54.55%), aged between 14 and 86years, with an average of 50.54years. Regarding the reason for extraction, syndesmotic dynamisation stands out in 5/11 patients, accounting for 45.45% of the extractions, followed by tibial nail dynamisations in 2/11 patients (18.2%).
The average extraction time was 31.45 minutes. A 100% extraction rate with ultrasound without the need for a fluoroscope was obtained. The average obtained on the VAS pain scale was 1.91 points. Four out of eleven patients (36.4%) required step one of the World Health Organisation (WHO) analgesic ladder during the first postoperative 24h. Regarding the percentage of intra- or postoperative complications, this was 9.09%, with only one superficial infection of the surgical wound being recorded, and which was resolved with oral antibiotics. The degree of satisfaction was 91% (10 of the 11 patients would recommend the surgery and would have it performed again). The data is reflected in Table 1.
Patient characteristics and study variables.
| Age (years) | Sex | Hardware removed | Reason | Time since initial surgery (weeks) | USOHR duration (minutes) | Paina | Posterior analgesia | Antibiotic prophylaxis | Wound incidence | Satisfaction | Scopy use | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient 1 | 24 | M | Transyndesmal screw after ORIF for ankle fracture | Syndesmotic dynamisation | 14.14 | 23 | 1 | Yes | Cefazolin i.v. | No | Yes | No |
| Patient 2 | 85 | F | Distal screw fibula plate after ORIF for fracture | Discomfort | 426.14 | 12 | 0 | No | Cloxacillin p.o. | No | Yes | No |
| Patient 3 | 52 | F | Proximal locking screw intramedullary nail tibia | Screw dynamisation | 12.14 | 32 | 0 | No | Cefazolin i.v. | No | Yes | No |
| Patient 4 | 65 | F | Screw in medial malleolus and transyndesmal screw after ORIF for ankle fracture | Discomfort + syndesmotic dynamisation | 50.43 | 50 | 0 | No | Cefazolin i.v. | No | Yes | No |
| Patient 5 | 36 | M | Transyndesmal screw after ORIF for ankle | Syndesmotic dynamisation | 10 | 25 | 2 | No | Cloxacillin p.o. | No | Yes | No |
| Patient 6 | 67 | F | Two screws in the medial malleolus after ORIF for an ankle fracture | Discomfort | 144.29 | 65 | 6 | Yes | Amoxicillin-ac. clavulanate v.o. | Superficial infection | No | No |
| Patient 7 | 44 | M | Proximal pantalar arthrodesis nail screws | Screw dynamisation | 23.86 | 40 | 0 | No | Cloxacillin p.o. | No | Yes | No |
| Patient 8 | 23 | M | Transyndesmal screw after ORIF for ankle fracture | Syndesmotic dynamisation | 32.43 | 27 | 1 | No | Cloxacillin p.o. | No | Yes | No |
| Patient 9 | 14 | F | Medial screw after ORIF for ankle fracture | Discomfort | 11.71 | 18 | 2 | No | Cloxacillin p.o. | No | Yes | No |
| Patient 10 | 60 | M | Proximal and distal tibia intramedullary nail screw | Discomfort | 256 | 35 | 6 | Yes | Cloxacillin p.o. | No | Yes | No |
| Patient 11 | 86 | F | Two transyndesmal screws after ORIF for ankle fracture | Syndesmotic dynamisation | 9.14 | 20 | 3 | Yes | Ciprofloxacin v.o.b | No | Yes | No |
i.v.: intravenous; p.o.: oral route; USOHR: ultrasound-guided osteosynthesis hardware removal.
Hardware extractions are very common surgeries in trauma and orthopaedic surgery operating rooms, with a prevalence of up to 5% of all interventions.1 Although its implementation is not widespread and continues to be a matter for debate, some centres use protocolised indications, as occurs with the removal of transyndesmal screws after an ankle fracture or in patients undergoing surgery using locked intramedullary nails for dynamisation.7 In these cases, the operating rooms are “completed” with what we conventionally call simple or routine surgeries, which are not risk-free for the patient and also entail a significant cost, since their brevity and the application of local aesthetic do not exempt them from requiring the use of surgical space or the collaboration of an anaesthetist in case their intervention is necessary.8 Furthermore, currently the standard tool for locating the osteosynthesis material to be extracted is conventional radiology with a fluoroscope, which entails having to use ionising radiation for the second time in a surgical procedure for the same patient.
Our study presents an ultrasound-guided extraction rate of 100% with 91% of the patients recommending surgery and only one superficial infection of the surgical wound, a complication percentage comparable to that obtained in the literature.9 It should be noted that the patient with the complication underwent dental implant surgery the week prior to the extraction of the osteosynthesis hardware, which we consider of interest due to its possible influence. The incidence was resolved with oral antibiotics. Regarding prophylaxis with oral antibiotic therapy, although current literature does not recommend its routine use (regardless of the hardware removed from the foot and ankle) and in many cases the decision depends on the protocol of each institution, we recommend its use because it does not pose an additional risk to the patient and thus avoids possible complications derived from the intervention. Although the number of patients was limited, the surgical wound infection rate obtained was 9.09%, which represents a proportion similar to that shown in other studies (13.2%) in the arm of patients treated with antibiotics.9 Tolerance to extraction with local anaesthesia could be classified as acceptable, since the average VAS was 1.91, and only 4 of the 11 patients needed first-ladder analgesic mediation after the intervention.
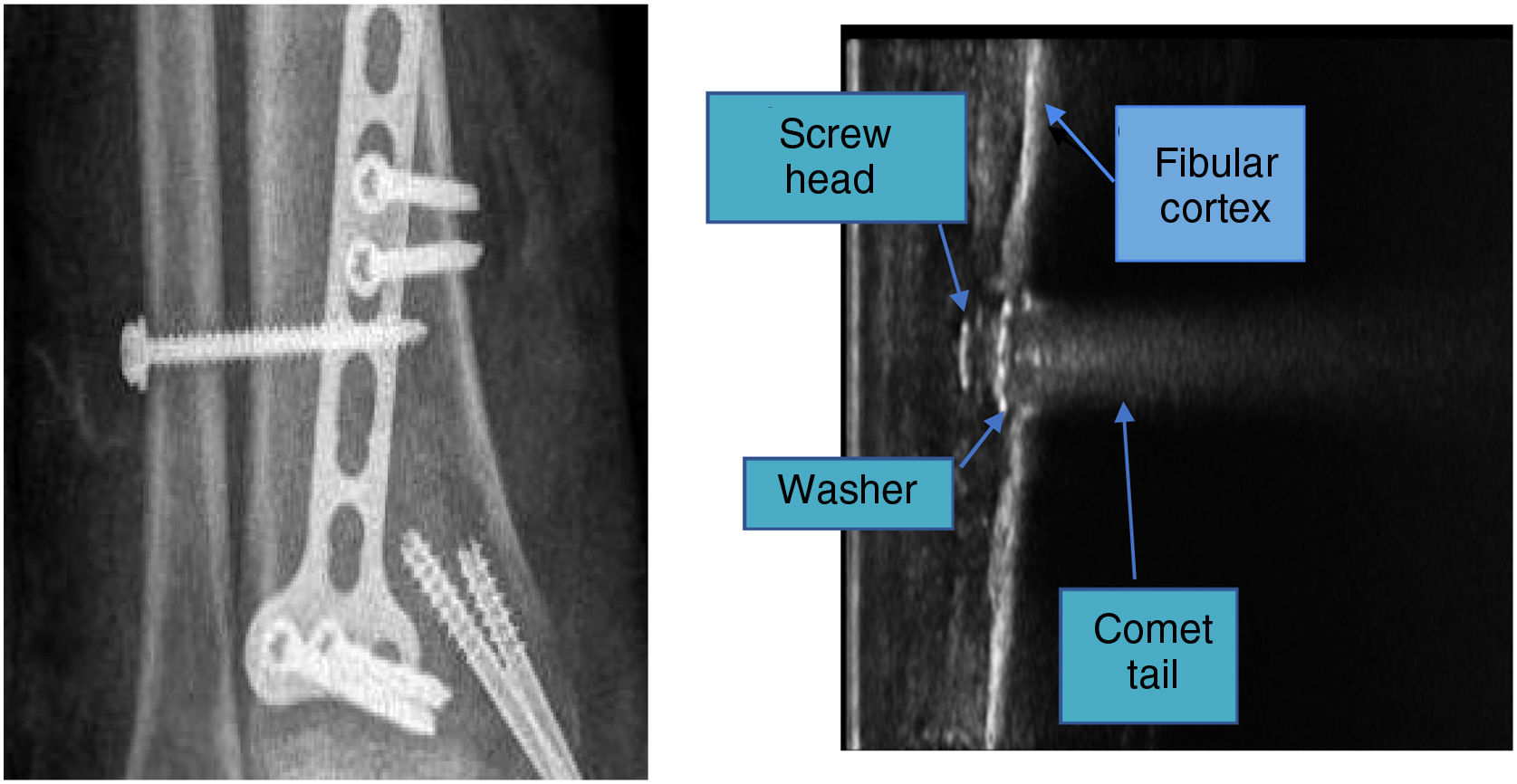
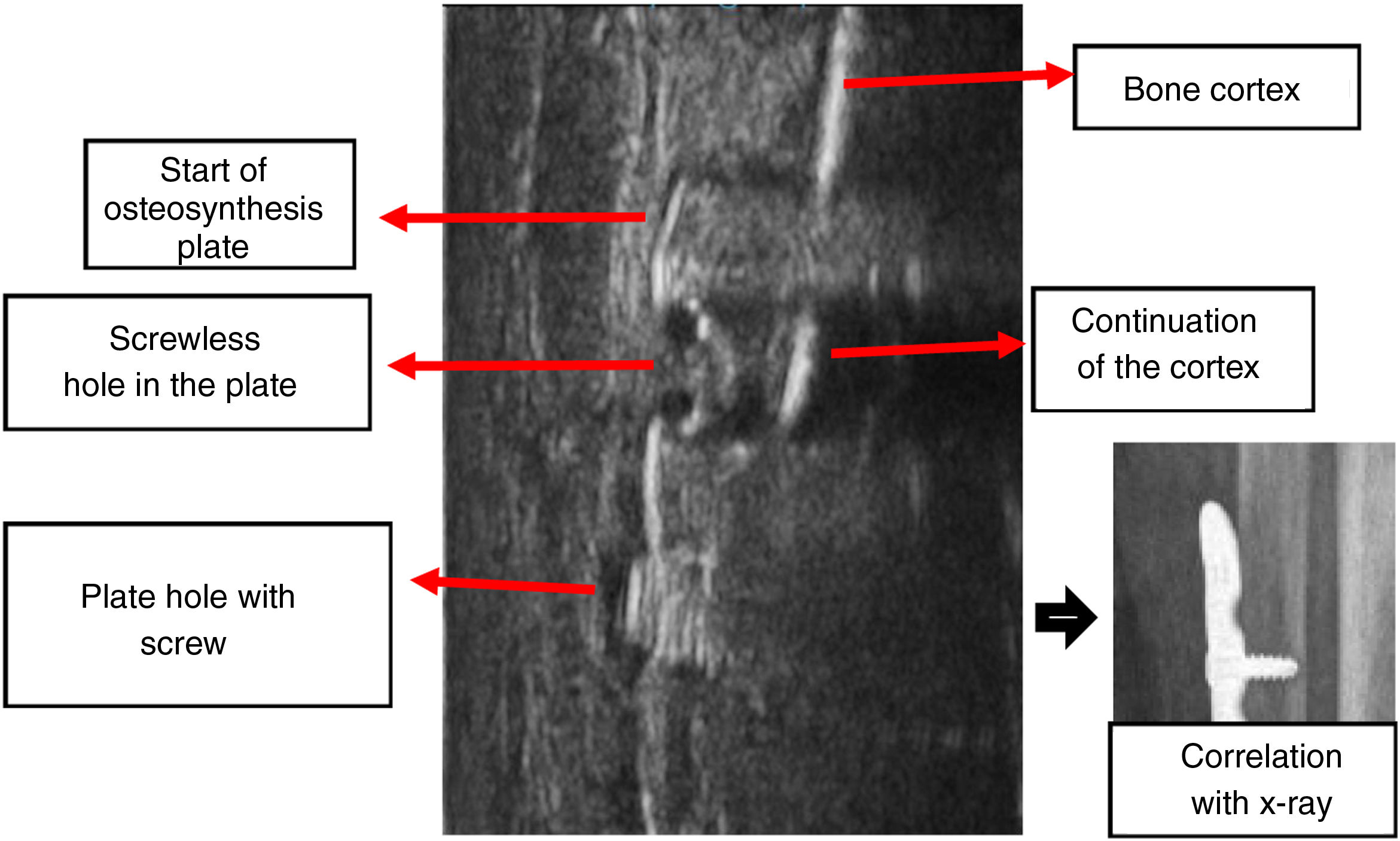
During the course of this study and based on our experience, in the most tortuous areas with more abrupt anatomy, scanning with conventional linear probes can be a challenge. This difficulty does not lie so much in the identification of the material, since metallic objects are easy to identify in ultrasound due to the comet tail image10,11 (Figs. 4 and 5), but in clearly defining the three-dimensionality of the location if the anatomical area to be treated has uneven areas in the three spatial planes, as occurs in our case in the medial malleolus. We consider that this fact may justify the increase in time in cases of extraction of screws located in the tibial malleolus with respect to other segments of the tibia or fibula exposed in Table 1.


“Comet tail” image obtained with ultrasound: in the area of the plate with a screwless hole, the continuation of the bone cortex treated with the osteosynthesis plate is observed; On both sides of it the artefact produced by the metal in the shape of a “comet tail” which obscures the bone cortex in the area of the plate without holes can be seen, together with its correlation with the simple X-ray.
Through this study we wished to highlight ultrasound as another alternative to traditional fluoroscopy when performing this type of intervention. It has the advantage of enabling real time assessment of hardware extraction and its immediate confirmation, in addition to being providing visualisation of adjacent tissues that may lead to complications in the procedure, such as nervous, vascular or tendon structures and other sources of possible discomfort associated with the material, such as haematomas or seromas. This ultrasound technique is notably free from ionising radiation. With this objective in mind, other authors have already described other methods to locate hardware without scopy. These would entail counting the palpable screw heads or following the skin staple tracing or the surgical scar. One of the advantages that ultrasound presents with respect to these techniques is to ensure localisation with direct visualisation and avoid the problems that we could encounter in attempting to find hardware in larger ankles (Fig. 6).

The major limitation of our study is that it is descriptive, without a control group, and the number of patients is low. A greater number of osteosynthesis hardware removals should be performed and analysed using this technique. If the patient's favourable tolerance and the absence of the need to perform it using scopy are confirmed, then it may be compared with the standard technique and assessment may be made as to whether the procedure could be performed as minor surgery. This could take place, for example, in an outpatient consultation room if it were possible to have a fluoroscope available in case of complications during the procedure, such as fractures secondary to extraction or problems with the osteosynthesis hardware.
ConclusionWe may conclude that ultrasound is a useful tool in assisting the occasional extraction of osteosynthesis hardware. It may also be sufficient alone, without the need for bulky devices with ionising radiation, such as traditional fluoroscopy and it may be considered an alternative for performing in an out-of-hospital setting.
Level of evidenceLevel of evidence iii.
Use of artificial intelligenceNo artificial intelligence was used in the preparation of this study.
FundingThis research did not receive specific support from public sector agencies, the commercial sector or non-profit entities.
Conflict of interestsThe authors have no conflict of interests to declare.
