




Aplasia of the posterior arches of the atlas is an uncommon condition caused by a defect in their closure. It is usually associated with different syndromes.
Case reportWe present 2 asymptomatic patients with aplasia of C1 posterior bodies.
ConclusionsFurther studies are required on these lesions in order to take possible protection measures against trauma, and the selection between conservative or surgical treatment.
La aplasia de los cuerpos posteriores del atlas es una afección poco frecuente, causada por un defecto en el cierre de los mismos. Habitualmente se asocia a diferentes síndromes.
Casos clínicosPresentamos 2 casos clínicos de pacientes asintomáticos con aplasia de los cuerpos posteriores del atlas.
ConclusionesEs necesario estudiar más a fondo este tipo de lesiones de cara a valorar la posibilidad de tomar medidas de protección ante traumatismos y escoger entre el tratamiento conservador y el quirúrgico.
Alterations in the posterior arches of the atlas are rare anomalies (<4% among the general population1) which are usually associated with some type of syndrome, such as Klippel–Feil, Turner, Di Giorge or Arnold–Chiari, and also with other alterations of the axial skeleton (torticollis, spina bifida, short neck, etc.),2,3 so their presence in healthy patients is rare.
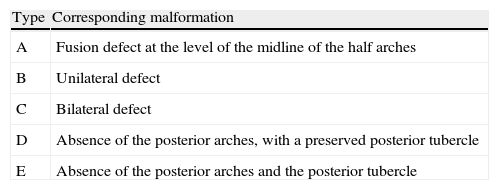
Currarino et al.4 classified defects in the posterior arches of the atlas into different degrees, as shown in Table 1.
Classification of anomalies of the posterior arches of the atlas elaborated by Currarino.
| Type | Corresponding malformation |
| A | Fusion defect at the level of the midline of the half arches |
| B | Unilateral defect |
| C | Bilateral defect |
| D | Absence of the posterior arches, with a preserved posterior tubercle |
| E | Absence of the posterior arches and the posterior tubercle |
We present 2 cases of Currarino type D congenital aplasia of the posterior arches of the atlas.
Case report 1The patient was a 54-year-old woman with a history of intervention due to right carpal tunnel syndrome (CTS). She attended consultation due to cervicalgias of long duration, which she suffered 13years earlier linked to a car accident. She also reported suffering frequent cervical contractures, with pain radiating to the right deltoid and occasional headaches with tensional characteristics (2–3/month). In addition, she suffered occasional mild paresthesias and slight loss of strength in both hands, more noticeable on the right side. She reported taking NSAIDs during the symptomatic periods, with only temporary improvement.
We observed a moderate contracture of the cervical paravertebral and trapezoid musculature (more noticeable on the right side), with mild pain on palpation. Her cervical mobility presented scarce functional limitation, as well as discomfort in the limbs, without radiation. The Valsalva and Lhermitte signs were negative.
- –
Fist strength: right – 10kgf; left – 20kgf (JAMAR® dynamometer).
- –
Grip strength: right – 4kgf; left – 5kgf (JAMAR® dynamometer).
- –
Strength in lower limbs (LL): 5/5.
- –
Preserved and symmetrical osteotendinous reflexes (OTR) in upper limbs (UL) and LL.
- –
Normal sensitivity.
Simple radiography (Rx) revealed the existence of a defect in the posterior arch of C1 with a preserved posterior tubercle (Currarino type D). We verified the stability of the tubercle through Rx in flexion and extension (Fig. 1A).
 Lateral radiograph of case 1. (B) Lateral radiograph of case 2, showing a remnant of the right arch. (C) 3D CT scan image of case 1.")
A computed tomography (CT) scan confirmed aplasia of the posterior arches of C1, with a preserved posterior tubercle (Fig. 1C). A magnetic resonance imaging (MRI) scan did not report any findings suggestive of spinal disorders.
We decided to follow a conservative treatment with exercises to strengthen the cervical muscles, stretching and postural hygiene. We recommended avoiding any situations which could cause hyperextension of the neck.
After several months of treatment, the patient reported slight improvement of headaches and neck pain.
Case report 2The patient was a 6-year-old boy, with no previous relevant history, who presented cervical pain of several weeks duration after suffering trauma whilst tumbling.
Physical examination did not appreciate contractures or facial asymmetry. There was slight discomfort on palpation of the paravertebral cervical and trapezoid musculature.
Cervical mobility was complete, with normal strength for the age, and without pain or alteration of OTR. Sensitivity was also normal.
Plain Rx (Fig. 1B) showed a defect in the posterior arch of the atlas (Currarino type D). We verified the stability of the remaining bone of the posterior arch with Rx in flexion and extension. We also obtained an MRI scan which confirmed the defect of the posterior arches of the atlas, with traces of the right arch and tubercle, and without spinal alterations.
In the absence of symptoms, the patient is currently advised to avoid any activity or situation which might cause cervical hyperextension.
ResultsThe evolution of both patients is satisfactory.
DiscussionAlterations of the posterior arch of the atlas are rare (<4%). This is especially true of type D cases, such as those presented in this work, which have a prevalence under 0.2%.1,4
When not associated with a syndrome (Down, Turner, Di Giorge, etc.), these patients are usually asymptomatic and the finding is incidental,5 mostly due to imaging studies performed after trauma or chronic neck pain.1,4 More rarely, patients may present cervicobrachialgia,6 Lhermitte's sign upon mobilising the neck,6,7 significant loss of strength and even transient tetraparesis after minimal trauma.5,7
Regarding treatment, the literature contains reports supporting different opinions. Some authors recommend treating all patients who retain the posterior tubercle by removing it, thus avoiding the risk of impaction on the spinal cord,7,8 whilst others support conservative treatment, with or without preventive measures, reserving surgery only for those cases with clear and proven symptoms due to compression by the tubercle.1,4
In our case, we decided to follow a conservative treatment, avoiding situations of risk, since there were no spinal alterations or signs of instability. We consider that, as a general rule, excision of the tubercle is overly aggressive in patients with no symptoms and may even cause instability. Moreover, we do not consider it to be indicated since, in the review by Senoglu et al.,1 most cases were incidental findings.
In cases showing neurological symptoms, we advocate testing these symptoms by means of dynamic nuclear magnetic resonance (NMR) and excision of the tubercle.
In conclusion, we believe that abnormalities of the posterior arches of the atlas are rare and usually asymptomatic, although potentially dangerous for the spine. Unfortunately, the literature is scarce and with a low level of evidence. Therefore, we believe it would be interesting to study more cases, in order to establish the possible indications for surgery and the usefulness of preventive measures (such as restricting sports activities or using a rigid collar when in cars), or whether these cases are benign deviations from the standard and do not require treatment or prevention.
Level of evidenceLevel of evidence V.
Ethical responsibilitiesProtection of people and animalsThe authors declare that this investigation did not require experiments on humans or animals.
Confidentiality of dataThe authors declare that this work does not reflect any patient data.
Right to privacy and informed consentThe authors declare that this work does not reflect any patient data.
Please cite this article as: Quinteiro Antolín T, et al. Aplasia de los arcos posteriores del atlas: a propósito de 2 casos. Rev Esp Cir Ortop Traumatol. 2012;56:381–4.
