



Associated neurovascular injuries to injured knee ligaments without dislocation are uncommon. We report the case of a young athlete who after a sports injury, suffered complete rupture of the anterior cruciate and the lateral collateral ligament. He had an associated paralysis of the peroneal nerve. The patient required two-stage surgery for stabilization, with ligament repair and reconstruction of the knee and surgery of the sequelae of the nerve injury, with very good functional results.
Despite the unusual association of nerve damage in this type of trauma, we need to identify this nerve damage early in order to establish optimal treatment.
Las lesiones vasculonerviosas asociadas a lesiones de los ligamentos de la rodilla sin luxación de la misma son infrecuentes. Se presenta el caso de un joven deportista que tras traumatismo deportivo, sufre rotura completa del ligamento cruzado anterior y ligamento lateral externo. Se le asoció parálisis completa del nervio ciático poplíteo externo. El paciente precisó reparación quirúrgica en dos tiempos, con estabilización de la rodilla mediante la reconstrucción y reparación ligamentosa, con muy buenos resultados funcionales y cirugía de las secuelas de la lesión nerviosa posteriormente. A pesar de la inusual asociación de lesiones nerviosas a este tipo de traumatismos, debemos saber identificarlas precozmente para precisar los tiempos terapéuticos de manera adecuada.
Anterior cruciate ligament (ACL) tear is common in contact sports, with 2/3 occurring during the playing of sports with a high prevalence (3/10,000inhabitants/year).1
Few articles have been published, either in this country or around the world, on the associated injuries to knee ligaments2 and the external popliteal sciatic nerve,3,4 possibly because of the infrequency of this association. High-energy trauma results in a dislocation and spontaneous reduction within tenths of a second, which has significant consequences for the capsule and ligaments. It is important that these so-called “hidden” dislocations be kept in mind, for a careful neurovascular evaluation should be performed to identify possible associated lesions.5
Posterolateral instability is relatively uncommon, the incidence being 2% of all knee ligament injuries and 9.1% in acute knee injuries with hemarthrosis.6,7 They are frequently associated with ACL and PCL injuries and with fractures of the tibial stem.8
Associated injury of the external popliteal sciatic or peroneal nerve is seen in a very wide range of 9–49% in knee dislocations and includes conditions from neuropraxia to neurotmesis3,4,9; it is uncommon in low-energy injuries without dislocation of the knee or injury to the PCL. The incidence of peroneal nerve injury increases following a posterolateral dislocation and in lateral and posterolateral ligament (PLA) tears. It is impossible to predict whether function will be restored to this nerve, and in more than half of the cases, it is not recoverable, according to published series.9 The case of a young patient is presented, who, following a sports injury to the knee with no apparent dislocation, had neurological involvement associated with the ligament injuries.
Clinical caseThe patient was a 27-year-old male who, while playing his accustomed sport, suffered a serious sports injury to the knee, with combined forced flexion and anterolateral rotation of this joint.
Upon examination, the knee was swollen, with fluid in the joint, varus tilt on full extension, and positive anterior drawer sign and Lachman test. Patient underwent an arthrocentesis, which showed bloody fluid in the joint. Patient also presented with hypaesthesia on the dorsum of the left foot, which he was unable to dorsiflex due to 0/5 weakness of the anterolateral muscles.
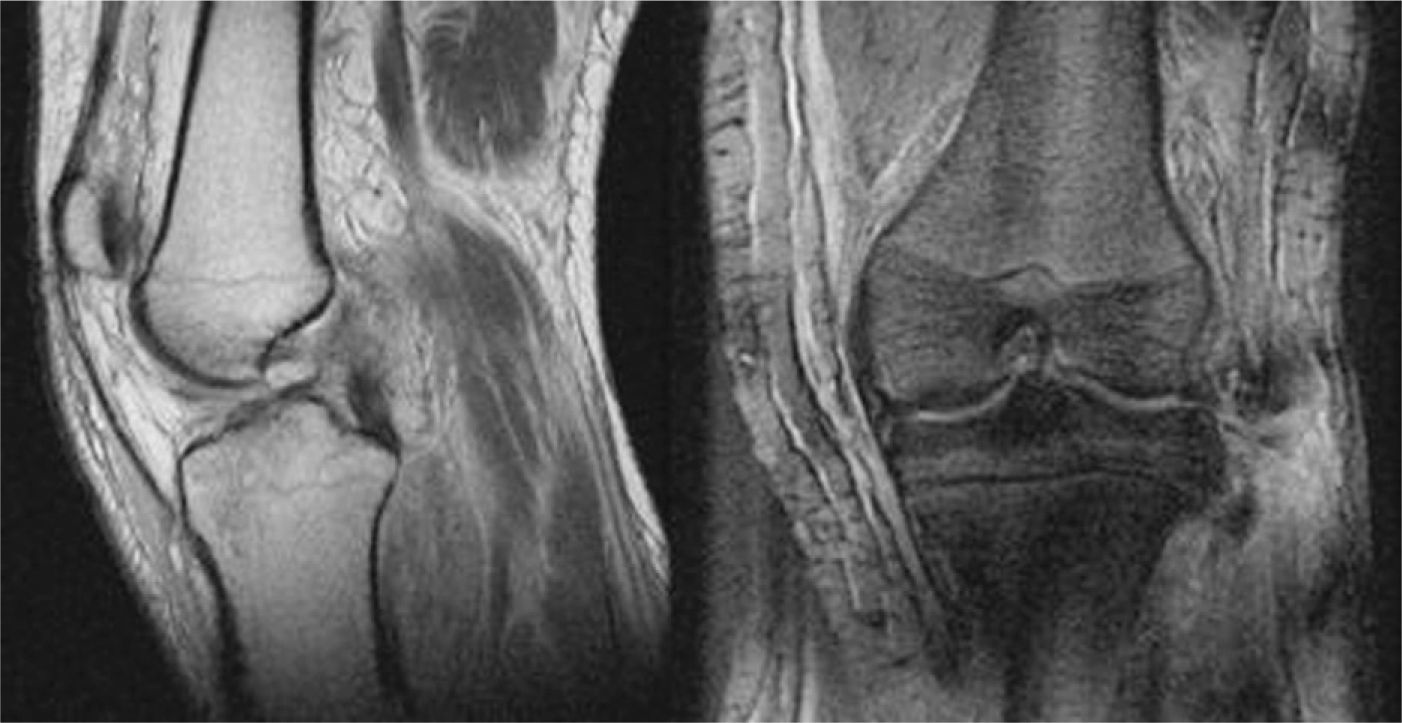
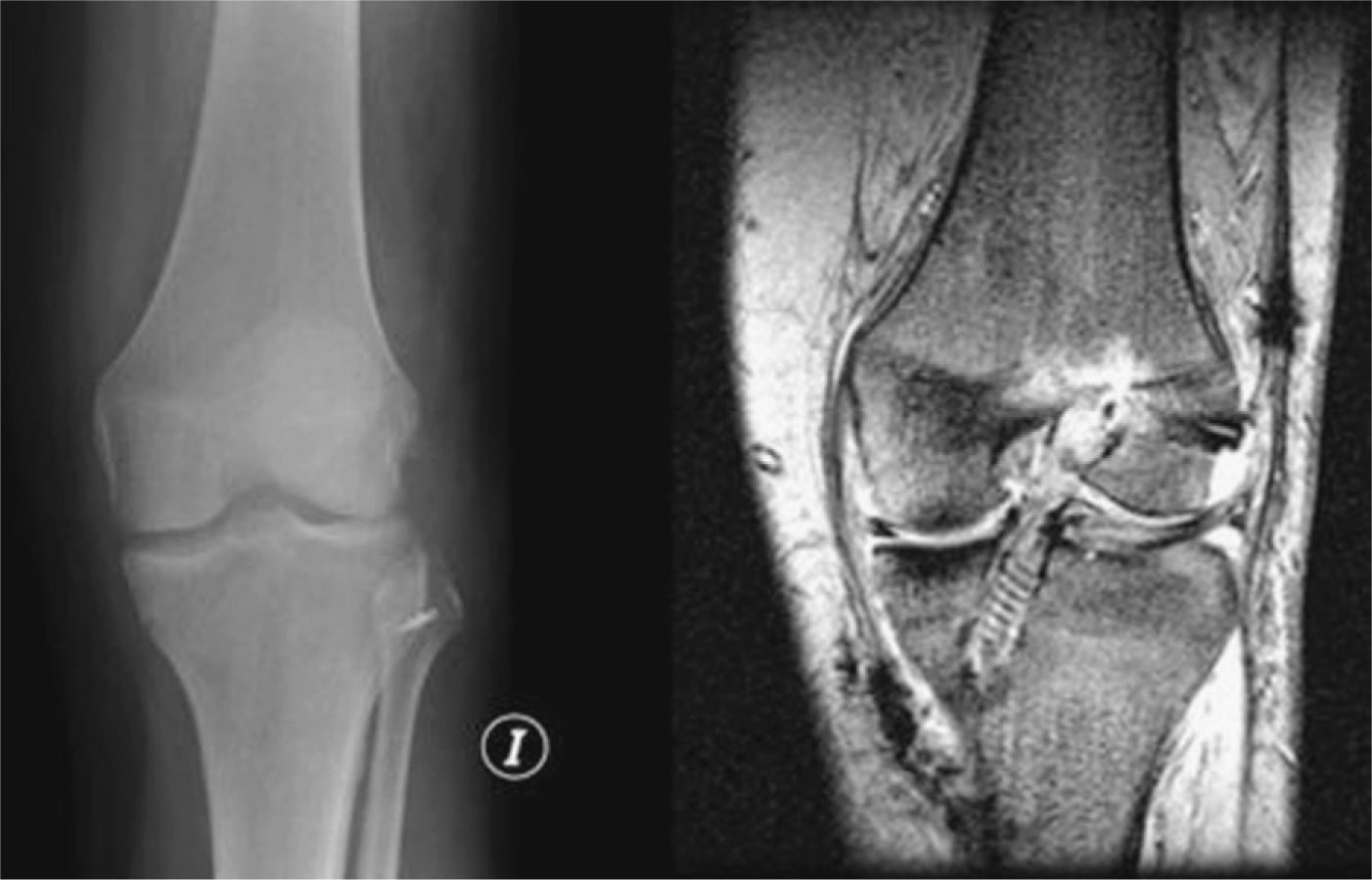
Plain X-rays showed no bony injuries. On MRI, there was evidence of a complete tear of the ACL and the external lateral ligament (ELL) near the insertion of the fibular head, together with a grade I–II tear of the muscle fibres in the middle, distal, and deep third of the soleus. The external popliteal sciatic nerve (EPS) did not show solution of continuity but had marked oedema and inflammation surrounding it (Fig. 1), with confirmation on the neuroelectromyogram (NEMG), where a severe axonal neuropathy of this nerve was observed showing a combined posterolateral and anterolateral rotational instability.

The patient underwent surgery for repair of the ACL and ELL lesions; a hamstring plasty of the semitendinosus and internal rectus was performed, together with reconstruction of the ELL using a wire hook for anchoring to the fibular head and suture reinforcement ascending from the ELL with support to biceps femoris (Fig. 2). Neurolysis of the peroneal nerve was performed simultaneously, and its integrity was confirmed but with deficit of motor potentials in the anterior tibial and extensor hallucis longus muscles on the intra-operative neurophysiological study.

Patient was discharged with an anti-equinus splint and a knee brace; he was allowed 0–90° range of motion and limited weight-bearing for 6 weeks. After these 6 weeks had passed, weight bearing and full flexion–extension of the knee was permitted.
There was favourable progression of the ACL and ELL injuries, with the knee stable upon examination and dynamic testing and full range of flexion and extension (0°/0°/120°), but the neurological deficit in the peroneal nerve continued.
The NEMG at 6 months showed a complete axonotmesis-type lesion of the EPS with no sign of renervation, so the decision was made to re-operate, and the patient underwent a transposition (re-routing) of the posterior tibial tendon to the base of the second cuneiform.
Six months after the transposition, patient showed limited plantar flexion and a reduction in steppage gait not dependent on the brace.
DiscussionThere are few references in the literature on associated ACL, PLA, and EPS injuries; the references are mainly about their surgical repair, with the results of direct intervention on these ligaments being published.2,5
Most authors recommended surgical repair as opposed to conservative treatment,2 and in the literature reviewed, there were very few studies relating peroneal nerve damage to knee ligament injury.
Peroneal nerve damage should be suspected whenever there are combination injuries of this type to the ligaments. It is essential that the knee be stabilized and that joint function be recovered as soon as possible by checking for possible associated neurological damage in the same surgical procedure and then, in a second time, performing direct surgery on the peroneal nerve, in the event of a complete neurotmesis or the sequelae.
Although the clinical case presented is not very common, when it does occur, it is a serious matter; therefore, in combination injuries of this type to ligaments of the knee, we should bear in mind the possibility of an associated injury of the external popliteal sciatic nerve.
Evidence levelEvidence level V (case presentation).
Protection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of DataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.
Please cite this article as: Pescador Hernández D, et al. Lesión del nervio ciático poplíteo externo, asociado a lesio-nes del ligamento cruzado anterior y del ángulo posterolateral de la rodilla. Rev Esp Cir Ortop Traumatol. 2011;55(6):457–459.
