




We described the case of a 12-year-old patient who presented isolated contracture of the left rectus femoris muscle with subsequent traumatic rupture of the distal myotendinous junction; for this reason she did not present contracture in extension of the knee but she presented dynamic contracture in flexion of the hip (Ely positive test), which generated great impact on walking. Surgical management with tenotomy of the anterior rectum was performed, obtaining good results. This pathology has low incidence and it has been reported little in the literature, so it is important to suspect it. We provide an updated diagnostic and therapeutic approach.
Describimos el caso de una paciente de 12 años de edad, quien presentó contractura aislada del músculo recto femoral izquierdo con posterior ruptura traumática de la unión miotendinosa distal; razón por la cual no presentaba contractura en extensión de la rodilla pero cursaba con contractura dinámica en flexión de la cadera (prueba de Ely positiva), que generaba gran impacto en la marcha. Se realizó manejo quirúrgico con tenotomía del recto anterior, obteniendo buenos resultados. Esta patología tiene baja incidencia y se ha reportado poco en la literatura, por lo que es importante sospecharla. Brindamos un abordaje diagnóstico y terapéutico actualizado.
Contracture of the quadriceps muscle in children has been little reported in the literature. This pathology usually mostly affects the rectus femoris muscle in isolation but singular changes to the vastus lateralis medialis and intermedialis femoris muscle may occur, and even mixed presentations may also be found.1
The majority of cases described and treated for contracture of the quadriceps muscle refer to a contracture on extension of the knee, due to fibrosis of this muscle.2–5 The main cause of this fibrosis is usually its acquisition on injecting vaccines or medication into this area. However, cases of patients with congenital contracture have been reported.4,6 we present the case of a patient with single contracture of the left rectus femoris muscle, who had no contracture with knee extension but who had a positive Ely test. In other words, when the knee was bent in prone position flexion of the hip occurred
Clinical caseA 12-year-old female patient, with changes to gait from 14 months of age. She had been assessed by multiple orthopaedists since the age of two, but no specific diagnosis had been made and conservative treatment always ensued. The patient had no pain, the parents did not refer to any other type of previous trauma or any relationship to the application of vaccines, but the patient complained of a marked left limp. At nine years of age, the symptoms became more marked, and physiotherapy was administered. During this, the patient presented with intense pain in the dismal region of the muscle, and therefore withdrew from any treatment up to the present time.
She came to our hospital where she was found to have a positive left Ely test with normal knee mobility, without dissymmetry in the length of the lower limbs but with a significant alteration in gait. Magnetic resonance of the thigh was requested which reported complete former rupture of the distal myotendinous junction of the rectus femoris muscle, with proximal retraction of muscle fibres of 25mm (Fig. 1A), and no abnormal findings in the medial and proximal region (Fig. 1B).
 Shows the trauma rupture of the distal myotendinous junctions of the rectus femoris muscle (see arrow). B) No changes were observed in the medial and proximal area of the quadriceps.")
Biomechanical compromise of gait was assessed, with a physical examination and a computerized study. In the physical examination the following findings were discovered:
- 1
Negative bilateral Thomas test.
- 2
Negative right and positive left Ober test.
- 3
Negative right and positive left Phelps sign.
- 4
Negative right and positive left Ely test.
- 5
Negative right and positive left Silfverskiöld test.
- 6
Bilateral negative knee extension lag.
- 7
Absence of joint hypermobility in both limbs.
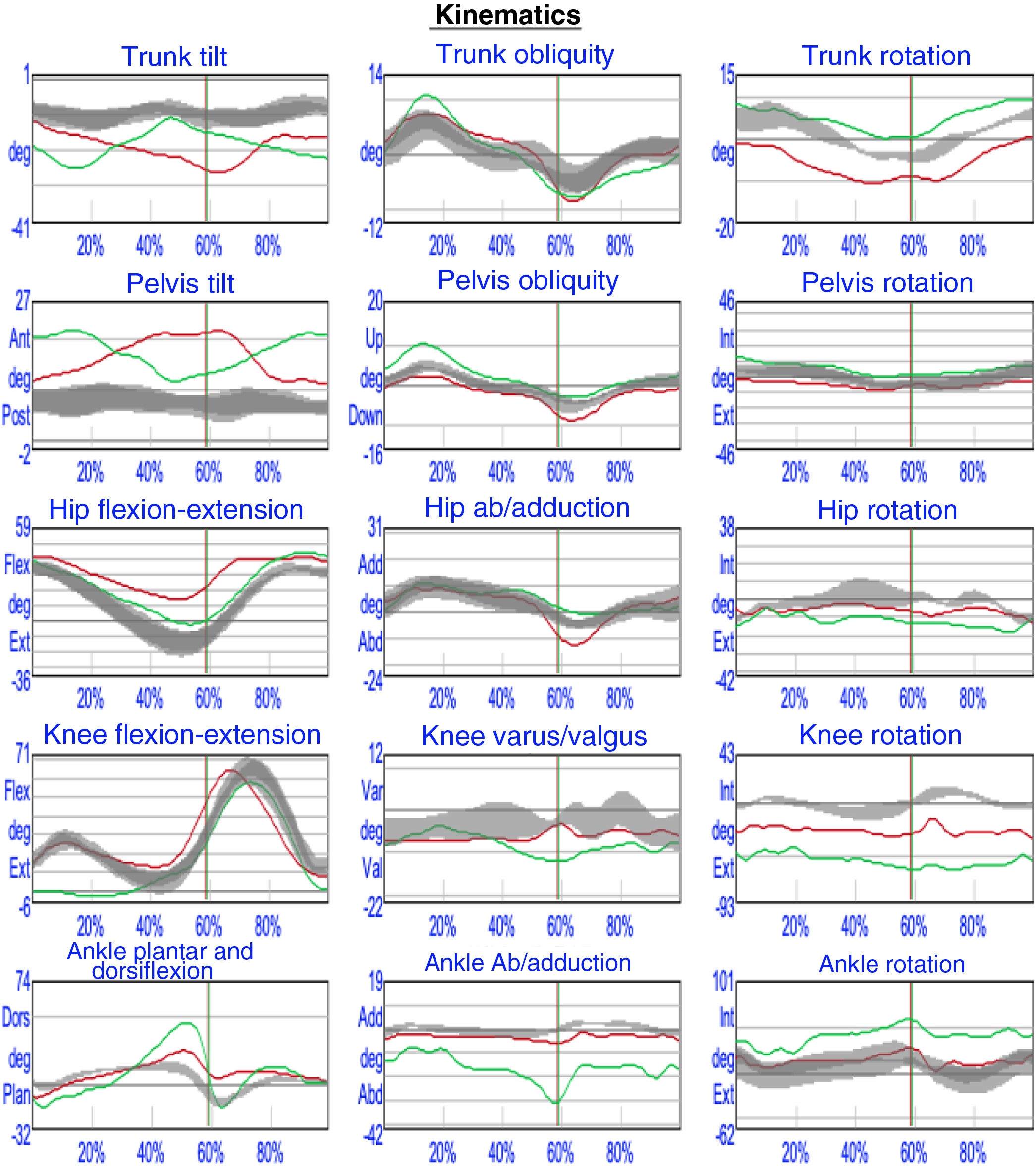
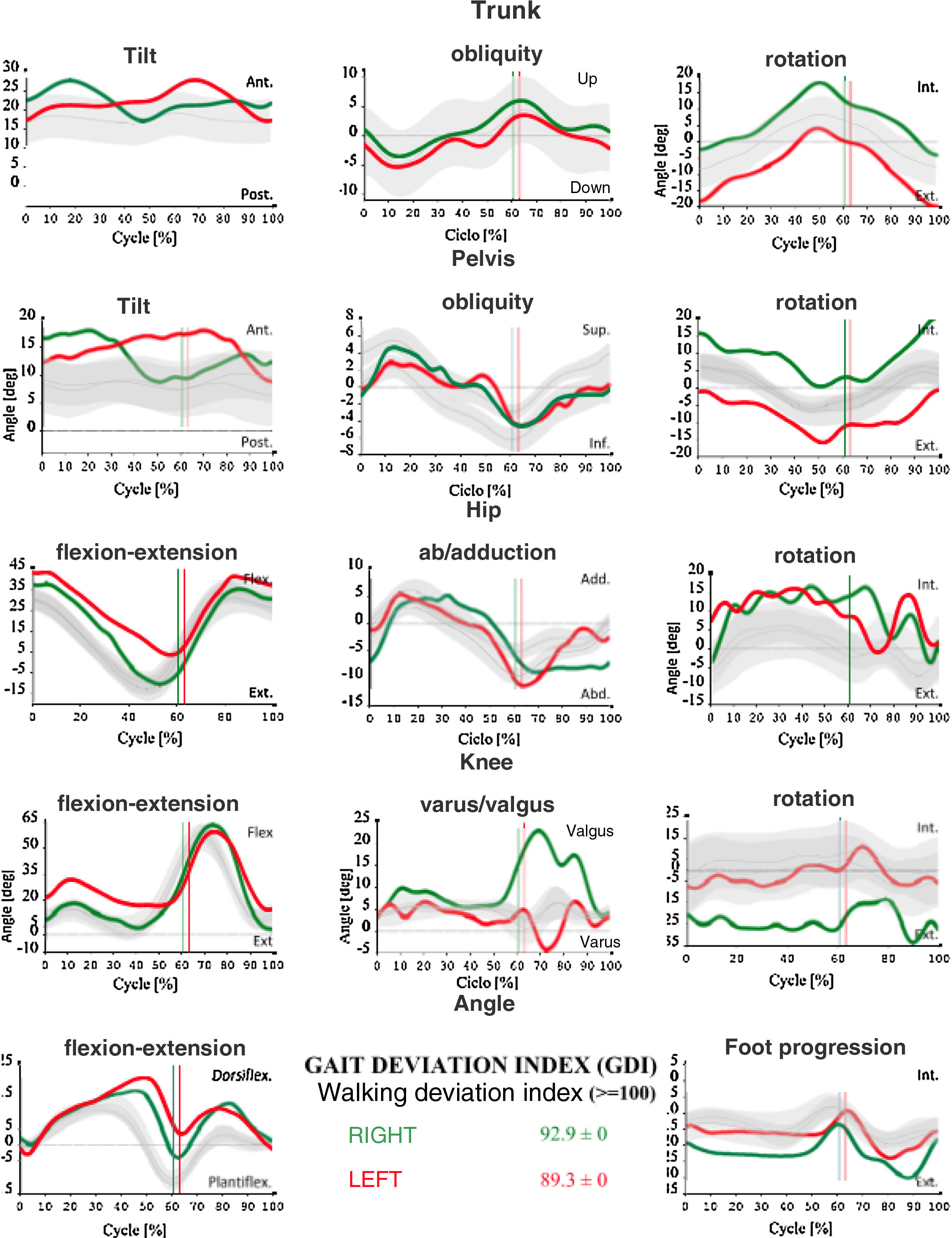
And the computerised study of gait revealed the following (Fig. 2):
- 1
Tilt of the left pelvis during the whole gait cycle.
- 2
Increase in flexion of the left hip during the whole gait cycle.
- 3
Reduction of left hip extension in the average support.
- 4
Bilateral absence of ankle equinus in saggital plane.
- 5
Drop of left pelvis and abduction of ipsilateral hip during the swing phase.
- 6
Hyperextension of right knee during support phase, secondary to tilt of the trunk.
- 7
No change to the flexion peak of the left knee during the oscillation phase, which could be explained by the previously mentioned traumatic rupture of the distal myotendinous junction.

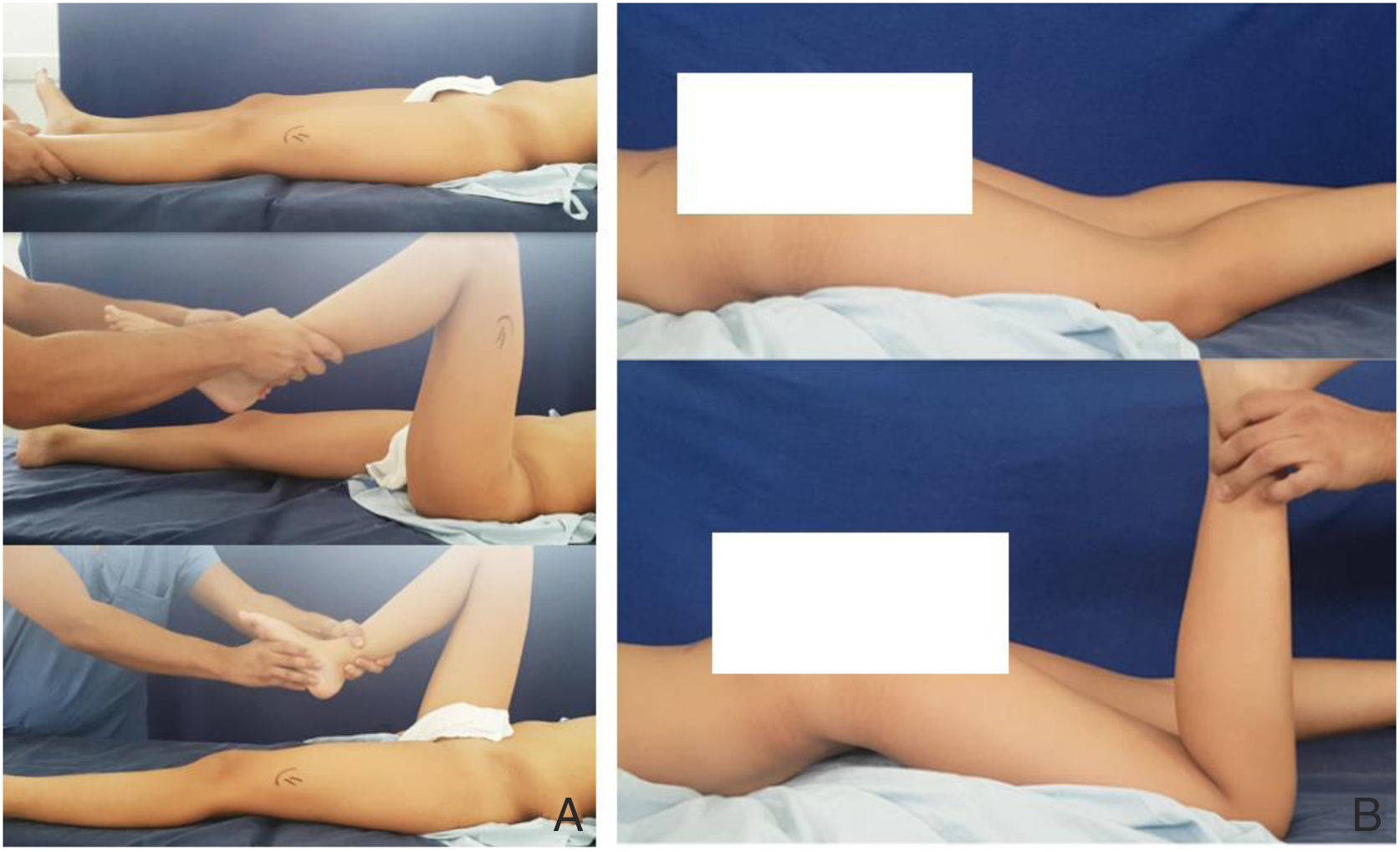
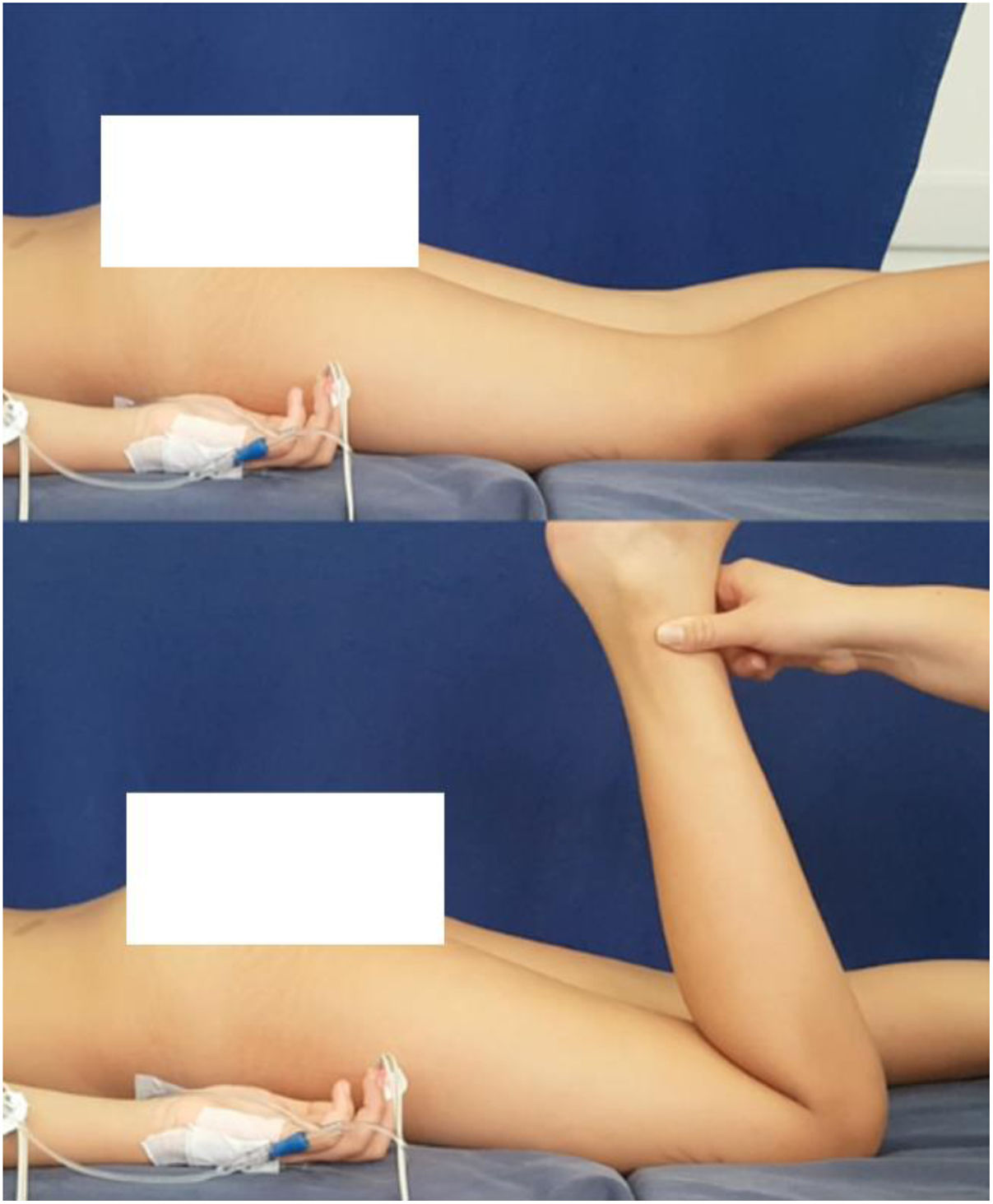
We decided to perform proximal release with tenotomy of the anterior rectum. The patient was assessed under anaesthesia in the operating theatre, with confirmation of negative Thomas test presence in the left hip and positive Ely test (Fig. 3).
 and positive Ely test B).")
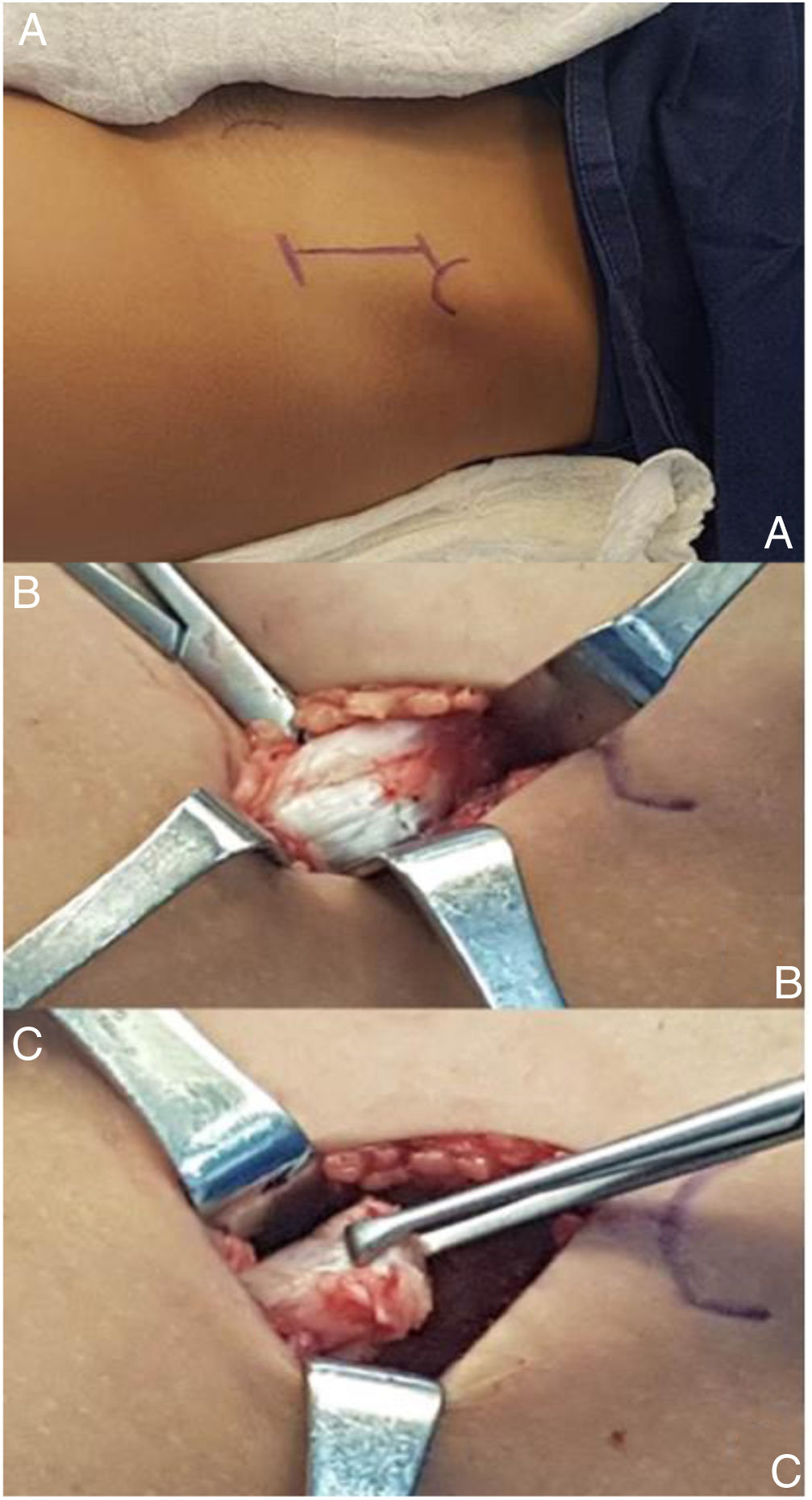
An anterior approach was performed, taking as the point of reference the antero superior iliac spine. Dissection was made between the muscle levels to locate the anterior rectus femoris tendon, which had hypertrophied. We proceeded to perform proximal tenotomy of the anterior rectum with mobilization distally, without reinsertion of the same (Fig. 4). The Ely test was performed again, which had normalized (Fig. 5). The patient’s postoperative recovery was optimum.
 Anterosuperior iliac crest as anatomical point during the anterior approach. B) Hypertrophy of the tendon of the anterior rectus muscle visualised. C) proximal tenotomy of the anterior rectus muscle.")

At present, after eight months of follow-up, the patient and her parents state gait has fully improved. On physical examination, the Silfverskiöld sign is now negative. The new computerised gait analysis shows a partial reduction of left pelvis tilt, reduction of the left hip flexion throughout the whole cycle of gait, nearly normal extension of the left hip in the supportive medium, absence of left hip drop which was recorded during swing with consequent correction of hip abduction and lastly, no previous mentioned hyperextension of the right knee was observed (Fig. 6).
Discussion
Contracture of the quadriceps muscle is a rare pathology, characterized by presenting with the progressive loss of knee flexion. It is classified in keeping with the compromised muscle with the intermediate vastus femoris as the most frequent, followed by the rectus femoris and lastly mixed presentation.7 The most common cause is intramuscular application of medicines, which leads to fibrosis of the muscle group. However, this is not the only cause since cases of congenital origin have been reported.4 Among the anatomopathological findings observed in this type of patient are excess of collagen and replacement of muscle tissue through fatty or fibrous tissue.8
Patients with quadriceps muscle contracture usually have limited flexion of the knee in supine position and even more so in prone position. Our patient presented with complete knee mobility in both supine and prone positions, due to the fact that during the course of her disease, the physiotherapy sessions aimed at recovering range of motion which led to a rupture of the anterior rectus femoris tendon in the distal part of the muscle. However, we considered that, as the change in the hip persisted, together with factors such as time of evolution and growth of tissues, more symptoms followed, converting them into the main problem of the hip flexion in the support phase.
Surgical treatment is directed at the affected muscle, releasing the attached regions which have previously shown up in imaging tests. In our case, we found the rectus femoris tendon to be ruptured in the distal region, which was why the standard clinical presentation of the progressive loss of knee flexion was not present and had confused the diagnosis. Computerised analysis of gait provided specific information regarding findings and provided treatment guidelines on demonstrating the muscle changes with their negative effect on gait cycle.
Indirectly, tendon rupture in the distal region shows us another surgical treatment option in patients who present exclusively with anterior rectum fibrosis, i.e. those patients who present with the typical symptoms of progressive restriction of knee flexion. Distal and proximal tenotomy of the rectus femoris tendon becomes a therapeutic alternative.
Although the frequency of this pathology is not very high, it should be included in differential diagnoses. Early diagnosis of the flexion deficit is required, with the performing of an accurate physical examination and establishing its cause so as to offer appropriate and pertinent treatment. Two diagnostic aids must be taken into consideration: nuclear magnetic resonance, to establish lesion compromise and location, and computerized analysis of gait, which provides information about the magnitude of the biomechanical compromise in the gait cycle and offers us with a further reason for operating on the patient.
Only two cases of contracture of the rectus femoris muscle in adults have been described in the recent literature. They were published in 2006 and 2011.2,7 However, this pathology has not been reported in paediatric patients since 1963 and 1974.9,10 The description of our case provides an updated diagnostic-therapeutic approach which extends all existing knowledge.
Level of evidenceLevel of evidence V.
FinancingThis study did not receive any type of financing.
Conflict of interestsThe authors have no conflict of interests to declare
Please cite this article as: Vela Rodríguez F, Jara Santana AB, Mafla Gómez M. Contractura aislada del músculo recto femoral: notificación y revisión de la patología a propósito de un caso. Rev Esp Cir Ortop Traumatol. 2021;65:158–163.
